Adverse Drug Reaction Overview: Adverse effects of ULTRACET (tramadol hydrochloride and paracetamol) tablets are similar to those of other opioid analgesics, and represent an extension of pharmacological effects of the drug class. The major hazards of opioids include respiratory and central nervous system depression and to a lesser degree, circulatory depression, respiratory arrest, shock and cardiac arrest.
The most frequently observed adverse effects of ULTRACET are headache, dizziness, nausea, constipation and somnolence as presented in Table 2.
Clinical Trial Adverse Drug Reactions: Because clinical trials are conducted under very specific conditions the adverse reaction rates observed in the clinical trials may not reflect the rates observed in practice and should not be compared to the rates in the clinical trials of another drug. Adverse drug reaction information from clinical trials is useful for identifying drug-related adverse events and for approximating rates.
ULTRACET (tramadol hydrochloride and paracetamol) tablets were administered to 1,597 patients during the double-blind or open-label extension periods in studies of chronic non-malignant pain. Of these patients, 539 were 65 years old or older. The most frequently reported events were in the central nervous and gastrointestinal systems. These are common effects associated with other drugs with opioid agonist activity. (See Table 2.)
 Click on icon to see table/diagram/image
Incidence at least 1% - Causal Relationship at Least Possible or Greater:
Click on icon to see table/diagram/image
Incidence at least 1% - Causal Relationship at Least Possible or Greater: The following lists treatment-emergent adverse reactions that occurred with an incidence of at least 1% in clinical trials with a population of 2,836 tramadol/paracetamol-exposed subjects in the 18 acute and chronic pain studies combined.
Body as a Whole: asthenia, fatigue, hot flushes.
Central and Peripheral Nervous System: dizziness, headache, tremor.
Gastrointestinal System: abdominal pain, constipation, diarrhea, dyspepsia, flatulence, dry mouth, nausea, vomiting.
Psychiatric Disorders: anorexia, anxiety, confusion, euphoria, insomnia, nervousness, somnolence.
Skin and Appendages: pruritus, rash, increased sweating.
Among these, the most common (≥ 5% of subjects) treatment-emergent adverse events were nausea (14%), dizziness (10%), somnolence (9%), constipation (8%), vomiting (5%), and headache (5%). These data are consistent with data presented in Table 2.
Sedation: Sedation is a common side effect of opioid analgesics, especially in opioid naïve individuals. Sedation may also occur partly because patients often recuperate from prolonged fatigue after the relief of persistent pain. Most patients develop tolerance to the sedative effects of opioids within three to five days and, if the sedation is not severe, will not require any treatment except reassurance. If excessive sedation persists beyond a few days, the dose of the opioid should be reduced and alternate causes investigated. Some of these are: concurrent CNS depressant medication, hepatic or renal dysfunction, brain metastases, hypercalcemia and respiratory failure. If it is necessary to reduce the dose, it can be carefully increased again after three or four days if it is obvious that the pain is not being well controlled. Dizziness and unsteadiness may be caused by postural hypotension, particularly in elderly or debilitated patients, and may be alleviated if the patient lies down.
Nausea and Vomiting: Nausea is a common side effect on initiation of therapy with opioid analgesics and is thought to occur by activation of the chemoreceptor trigger zone, stimulation of the vestibular apparatus and through delayed gastric emptying. The prevalence of nausea declines following continued treatment with opioid analgesics. When instituting therapy with an opioid for chronic pain, the routine prescription of an antiemetic should be considered. In the cancer patient, investigation of nausea should include such causes as constipation, bowel obstruction, uremia, hypercalcemia, hepatomegaly, tumor invasion of celiac plexus and concurrent use of drugs with emetogenic properties. Persistent nausea which does not respond to dosage reduction may be caused by opioid-induced gastric stasis and may be accompanied by other symptoms including anorexia, early satiety, vomiting and abdominal fullness. These symptoms respond to chronic treatment with gastrointestinal prokinetic agents.
Constipation: Practically all patients become constipated while taking opioids on a persistent basis. In some patients, particularly the elderly or bedridden, fecal impaction may result. It is essential to caution the patients in this regard and to institute an appropriate regimen of bowel management at the start of prolonged opioid therapy. Stimulant laxatives, stool softeners, and other appropriate measures should be used as required. As fecal impaction may present as overflow diarrhea, the presence of constipation should be excluded in patients on opioid therapy prior to initiating treatment for diarrhea.
The following adverse effects occur less frequently with opioid analgesics and include those reported in ULTRACET clinical trials, whether related or not to tramadol and paracetamol.
Less Common Clinical Trial Adverse Drug Reactions (<1%): The following lists clinically relevant treatment-emergent adverse reactions that occurred with an incidence of less than 1% in tramadol/paracetamol clinical trials.
Body as a Whole: chest pain, rigors, syncope, withdrawal syndrome, allergic reaction.
Cardiovascular Disorders: hypertension, aggravated hypertension, hypotension, dependent edema.
Central and Peripheral Nervous System: ataxia, convulsions, hypertonia, migraine, aggravated migraine, involuntary muscle contractions, paresthesia, stupor, vertigo.
Gastrointestinal System: dysphagia, melena, tongue edema.
Hearing and Vestibular Disorders: tinnitus.
Heart Rate and Rhythm Disorders: arrhythmia, palpitation, tachycardia.
Liver and Biliary System: abnormal hepatic function, SGPT (ALAT) increased, SGOT (ASAT) increased.
Metabolic and Nutritional Disorders: weight decrease, hypoglycemia, increased alkaline phosphatase, weight increase.
Musculoskeletal System Disorders: arthralgia.
Platelets, Bleeding and Clotting Disorders: increased coagulation time, purpura.
Psychiatric Disorders: amnesia, depersonalisation, depression, drug abuse, emotional lability, hallucination, impotence, bad dreams, abnormal thinking.
Red Blood Cell Disorders: anemia.
Respiratory System: dyspnea, bronchospasm.
Skin and Appendages Disorders: dermatitis, erythematous rash.
Urinary System: albuminuria, micturition disorder, oliguria, urinary retention.
Vision Disorders: abnormal vision.
White Cell and RES Disorders: granulocytopenia and leukocytosis.
Other Clinically Significant Adverse Experiences Previously Reported in Clinical Trials or Post-marketing Reports with Tramadol: Other events which have been reported with the use of tramadol products and for which a causal association has not been determined include: vasodilation, orthostatic hypotension, myocardial ischemia, pulmonary edema, allergic reactions (including anaphylaxis and urticaria, Stevens- Johnson syndrome/TENS), cognitive dysfunction, difficulty concentrating, suicidal tendency, hepatitis, liver failure, worsening of asthma, and gastrointestinal bleeding. Reported laboratory abnormalities included elevated creatinine and liver function tests.
Additional events which have been reported with the use of tramadol products and for which a causal association has not been determined include: abdominal discomfort, agitation, chest discomfort, cold sweat, disorientation, dry throat, ear discomfort, feeling abnormal, feeling jittery, gait disturbance, irritability, lethargy, malaise, memory impairment, prothrombin time prolonged, psychomotor hyperactivity, sleep disorder, thirst, vision blurred.
Serotonin syndrome (whose symptoms may include mental status change, hyperreflexia, fever, shivering, tremor, agitation, diaphoresis, seizures and coma) has been reported with tramadol when used concomitantly with other serotonergic agents such as SSRIs and MAOIs.
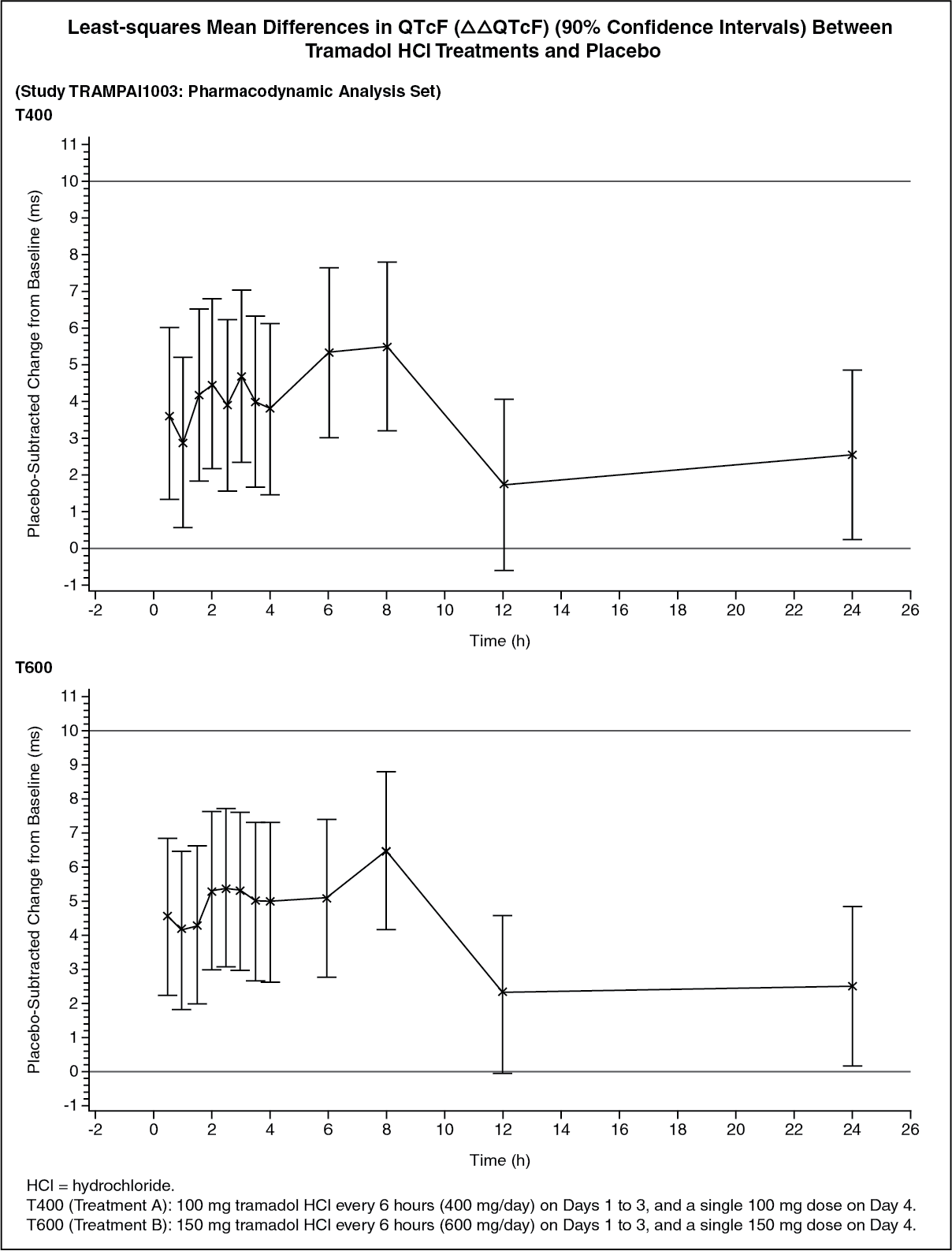
Post-marketing experience with the use of tramadol containing products included rare reports of delirium, miosis, mydriasis, and speech disorder, and very rare reports of movement disorder including dyskinesia and dystonia. Electrocardiogram QT prolonged, ventricular fibrillation, and ventricular tachycardia have been reported during post-market use.
Cases of hypoglycemia have been reported in patients taking tramadol, mostly in patients with pre-disposing risk factors, including diabetes, elderly and renal insufficiency. Caution should be exercised when prescribing tramadol to diabetic patients. More frequent monitoring of blood glucose levels may be appropriate, including at initiation or dose increase.
Cases of hyponatremia and/or SIADH have been reported very rarely in patients taking tramadol, usually in patients with predisposing risk factors, such as the elderly or those using concomitant medications that may cause hyponatremia.
Androgen deficiency: Chronic use of opioids may influence the hypothalamic-pituitary-gonadal axis, leading to androgen deficiency that may manifest as low libido, impotence, erectile dysfunction, amenorrhea, or infertility. The causal role of opioids in the clinical syndrome of hypogonadism is unknown because the various medical, physical, lifestyle, and psychological stressors that may influence gonadal hormone levels have not been adequately controlled for in studies conducted to date. Patients presenting with symptoms of androgen deficiency should undergo laboratory evaluation.
Other Clinically Significant Adverse Experiences Previously Reported in Clinical Trials or Post-marketing Reports with Paracetamol: Allergic reactions (primarily skin rash) or reports of hypersensitivity secondary to paracetamol are rare and generally controlled by discontinuation of the drug and, when necessary, symptomatic treatment. There have been several reports that suggest that paracetamol may produce hypoprothrombinemia when administered with warfarin-like compounds. In other studies, prothrombin time did not change.
Additional events which have been reported with the use of paracetamol products and for which a causal association has not been determined include: feeling hot, fixed eruption, pruritus generalized.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image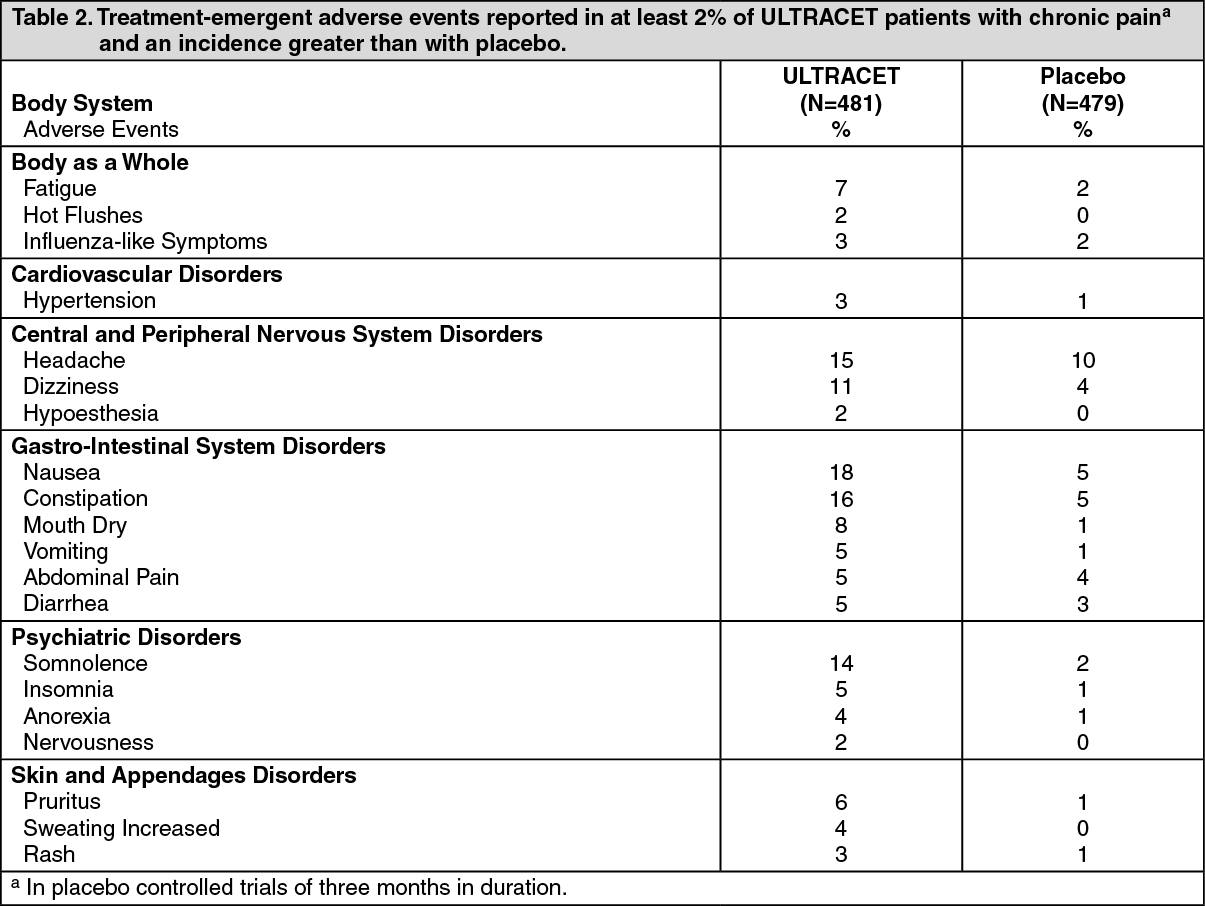 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image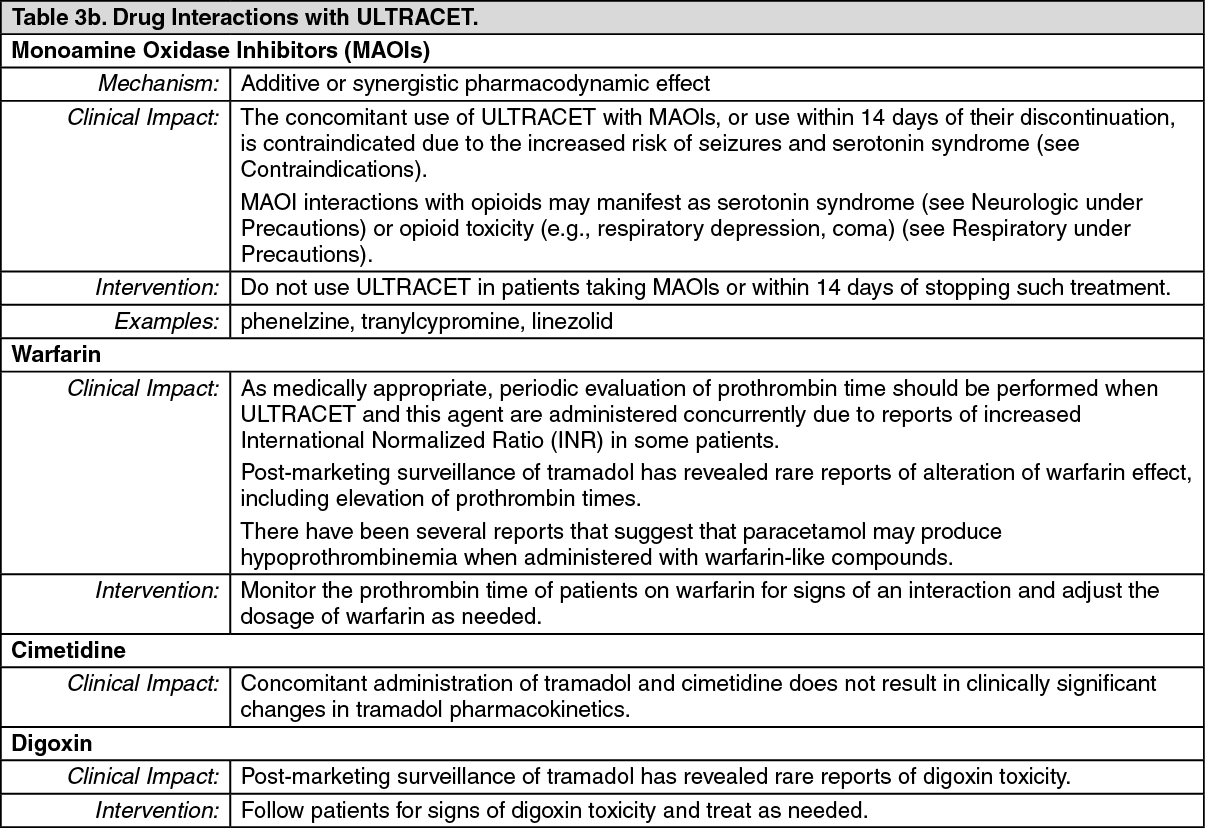 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out