


 Sign Out
Sign Out
The most commonly reported adverse reactions during treatment with VELCADE are nausea, diarrhoea, constipation, vomiting, fatigue, pyrexia, thrombocytopenia, anaemia, neutropenia, peripheral neuropathy (including sensory), headache, paraesthesia, decreased appetite, dyspnoea, rash, herpes zoster and myalgia.
Tabulated summary of adverse reactions: Multiple Myeloma: Undesirable effects in Table 13 were considered by the investigators to have at least a possible or probable causal relationship to VELCADE. These adverse reactions are based on an integrated data set of 5,476 patients of whom 3,996 were treated with VELCADE at 1.3 mg/m2 and included in Table 13.
Overall, VELCADE was administered for the treatment of multiple myeloma in 3,974 patients.
Adverse reactions are listed below by system organ class and frequency grouping. Frequencies are defined as: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Table 13 has been generated using Version 14.1 of the MedDRA.
Post marketing adverse reactions not seen in clinical trials are also included.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMantle Cell Lymphoma (MCL): The safety profile of VELCADE in 240 MCL patients treated with VELCADE at 1.3 mg/m2 in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone (VcR-CAP) versus 242 patients treated with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone [R-CHOP] was relatively consistent to that observed in patients with multiple myeloma with main differences described below. Additional adverse drug reactions identified associated with the use of the combination therapy (VcR-CAP) were hepatitis B infection (<1%) and myocardial ischaemia (1.3%). The similar incidences of these events in both treatment arms, indicated that these adverse drug reactions are not attributable to VELCADE alone. Notable differences in the MCL patient population as compared to patients in the multiple myeloma studies were a ≥5% higher incidence of the haematological adverse reactions (neutropenia, thrombocytopenia, leukopenia, anemia, lymphopenia), peripheral sensory neuropathy, hypertension, pyrexia, pneumonia, stomatitis, and hair disorders.
Adverse drug reactions identified as those with a ≥1% incidence, similar or higher incidence in the VcR-CAP arm and with at least a possible or probable causal relationship to the components of the VcR-CAP arm, are listed in Table 14. Also included are adverse drug reactions identified in the VcR-CAP arm that were considered by investigators to have at least a possible or probable causal relationship to VELCADE based on historical data in the multiple myeloma studies.
Adverse reactions are listed as follows by system organ class and frequency grouping. Frequencies are defined as: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Table 14 has been generated using Version 16 of the MedDRA.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of Selected Adverse Reactions: Herpes Zoster Virus Reactivation: Multiple Myeloma: Antiviral prophylaxis was administered to 26% of the patients in the Vc+M+P arm. The incidence of herpes zoster among patients in the Vc+M+P treatment group was 17% for patients not administered antiviral prophylaxis compared to 3% for patients administered antiviral prophylaxis.
Mantle Cell Lymphoma: Antiviral prophylaxis was administered to 137 of 240 patients (57%) in the VcR-CAP arm. The incidence of herpes zoster among patients in the VcR-CAP arm was 10.7% for patients not administered antiviral prophylaxis compared to 3.6% for patients administered antiviral prophylaxis (see Precautions).
Hepatitis B Virus (HBV) Reactivation and Infection: Mantle Cell Lymphoma: HBV infection with fatal outcomes occurred in 0.8% (n=2) of patients in the non VELCADE treatment group (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; R-CHOP ) and 0.4% (n=1) of patients receiving VELCADE in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone (VcR-CAP). The overall incidence of hepatitis B infections was similar in patients treated with VcR-CAP or with R-CHOP (0.8% vs 1.2% respectively).
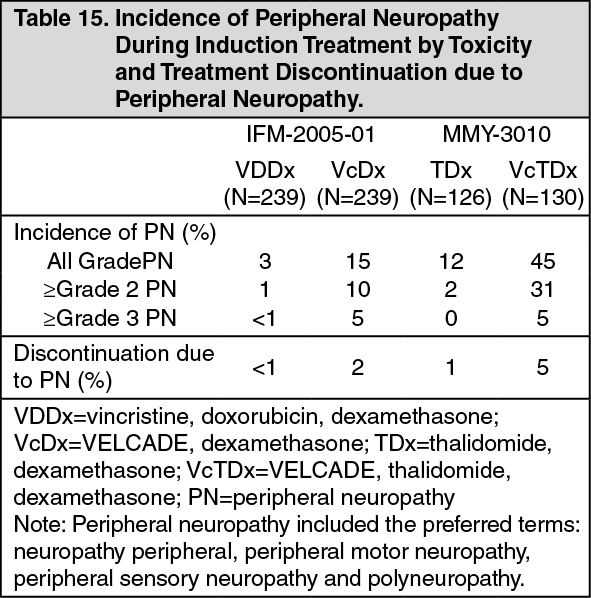
Peripheral Neuropathy in Combination Regimens: Multiple Myeloma: In trials in which VELCADE was administered as induction treatment in combination with dexamethasone (study IFM-2005-01), and dexamethasone thalidomide (study MMY-3010), the incidence of peripheral neuropathy in the combination regimens is presented in Table 15.
 Click on icon to see table/diagram/image
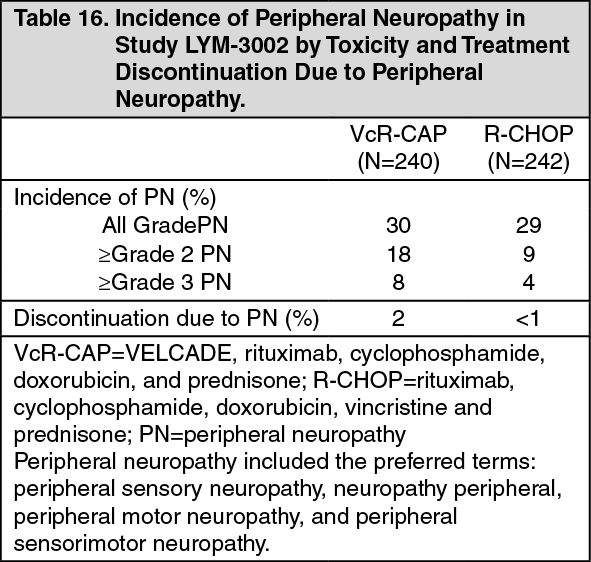
Click on icon to see table/diagram/imageMantle Cell Lymphoma: In study LYM-3002 in which VELCADE was administered with cyclophosphamide, doxorubicin, and prednisone (R-CAP), the incidence of peripheral neuropathy in the combination regimens is presented in Table 16.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageElderly MCL Patients: 42.9% and 10.4% of patients in the VcR-CAP arm were in the range 65-74 years and ≥75 years of age, respectively. Although in patients aged ≥75 years, both VcR-CAP and R-CHOP were less tolerated, the serious adverse event rate in the VcR-CAP groups was 68%, compared to 42% in the R-CHOP group.
Notable Differences in the Safety Profile of VELCADE Administered Subcutaneously Versus Intravenously as Single Agent: In the Phase III study patients who received VELCADE subcutaneously compared to intravenous administration had 13% lower overall incidence of treatment emergent adverse reactions that were Grade 3 or higher in toxicity, and a 5% lower incidence of discontinuation of VELCADE. The overall incidence of diarrhoea, gastrointestinal and abdominal pain, asthenic conditions, upper respiratory tract infections and peripheral neuropathies were 12% 15% lower in the subcutaneous group than in the intravenous group. In addition, the incidence of Grade 3 or higher peripheral neuropathies was 10% lower, and the discontinuation rate due to peripheral neuropathies 8% lower for the subcutaneous group as compared to the intravenous group.
Six percent of patients had an adverse local reaction to subcutaneous administration, mostly redness. Cases resolved in a median of 6 days, dose modification was required in two patients. Two (1%) of the patients had severe reactions; 1 case of pruritus and 1 case of redness.
The incidence of death on treatment was 5% in the subcutaneous treatment group and 7% in the intravenous treatment group. Incidence of death from “Progressive disease” was 18% in the subcutaneous group and 9% in the intravenous group.
Retreatment of Patients with Relapsed Multiple Myeloma: In a study in which VELCADE retreatment was administered in 130 patients with relapsed multiple myeloma, who previously had at least partial response on a VELCADE containing regimen, the most common all grade adverse events occurring in at least 25% of patients were thrombocytopenia (55%), neuropathy (40%), anaemia (37%), diarrhoea (35%), and constipation (28%). All grade peripheral neuropathy and grade ≥3 peripheral neuropathy were observed in 40% and 8.5% of patients, respectively.
Reporting of Suspected Adverse Reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
View ADR Monitoring Form