Pharmacotherapeutic group: HMG-CoA reductase inhibitors in combination with other lipid modifying agents.
ATC code: C10BA02.
Pharmacology: Pharmacodynamics: VYTORIN (ezetimibe/simvastatin) is a lipid-lowering product that selectively inhibits the intestinal absorption of cholesterol and related plant sterols and inhibits the endogenous synthesis of cholesterol.
Mechanism of action: VYTORIN: Plasma cholesterol is derived from intestinal absorption and endogenous synthesis. VYTORIN contains ezetimibe and simvastatin, two lipid-lowering compounds with complementary mechanisms of action. VYTORIN reduces elevated total cholesterol (total-C), LDL-C, apolipoprotein B (Apo B), triglycerides (TG), and non-high-density lipoprotein cholesterol (non-HDL-C), and increases high-density lipoprotein cholesterol (HDL-C) through dual inhibition of cholesterol absorption and synthesis.
Ezetimibe: Ezetimibe inhibits the intestinal absorption of cholesterol. Ezetimibe is orally active and has a mechanism of action that differs from other classes of cholesterol-reducing compounds (e.g., statins, bile acid sequestrants [resins], fibric acid derivatives, and plant stanols). The molecular target of ezetimibe is the sterol transporter, Niemann-Pick C1-Like 1 (NPC1L1), which is responsible for the intestinal uptake of cholesterol and phytosterols.
Ezetimibe localises at the brush border of the small intestine and inhibits the absorption of cholesterol, leading to a decrease in the delivery of intestinal cholesterol to the liver; statins reduce cholesterol synthesis in the liver and together these distinct mechanisms provide complementary cholesterol reduction. In a 2-week clinical study in 18 hypercholesterolaemic patients, ezetimibe inhibited intestinal cholesterol absorption by 54%, compared with placebo.
A series of preclinical studies was performed to determine the selectivity of ezetimibe for inhibiting cholesterol absorption. Ezetimibe inhibited the absorption of [
14C]-cholesterol with no effect on the absorption of triglycerides, fatty acids, bile acids, progesterone, ethinyl estradiol, or fat soluble vitamins A and D.
Simvastatin: After oral ingestion, simvastatin, which is an inactive lactone, is hydrolysed in the liver to the corresponding active β-hydroxyacid form which has a potent activity in inhibiting HMG-CoA reductase (3 hydroxy - 3 methylglutaryl CoA reductase). This enzyme catalyses the conversion of HMG-CoA to mevalonate, an early and rate-limiting step in the biosynthesis of cholesterol.
Simvastatin has been shown to reduce both normal and elevated LDL-C concentrations. LDL is formed from very-low-density protein (VLDL) and is catabolized predominantly by the high affinity LDL receptor. The mechanism of the LDL-lowering effect of simvastatin may involve both reduction of VLDL-cholesterol (VLDL-C) concentration and induction of the LDL receptor, leading to reduced production and increased catabolism of LDL-C. Apolipoprotein B also falls substantially during treatment with simvastatin. In addition, simvastatin moderately increases HDL-C and reduces plasma TG. As a result of these changes, the ratios of total- to HDL-C and LDL- to HDL-C are reduced.
Clinical efficacy and safety: In controlled clinical studies, VYTORIN significantly reduced total-C, LDL-C, Apo B, TG, and non-HDL-C, and increased HDL-C in patients with hypercholesterolaemia.
Prevention of Cardiovascular Events: VYTORIN has been shown to reduce major cardiovascular events in patients with coronary heart disease and ACS event history.
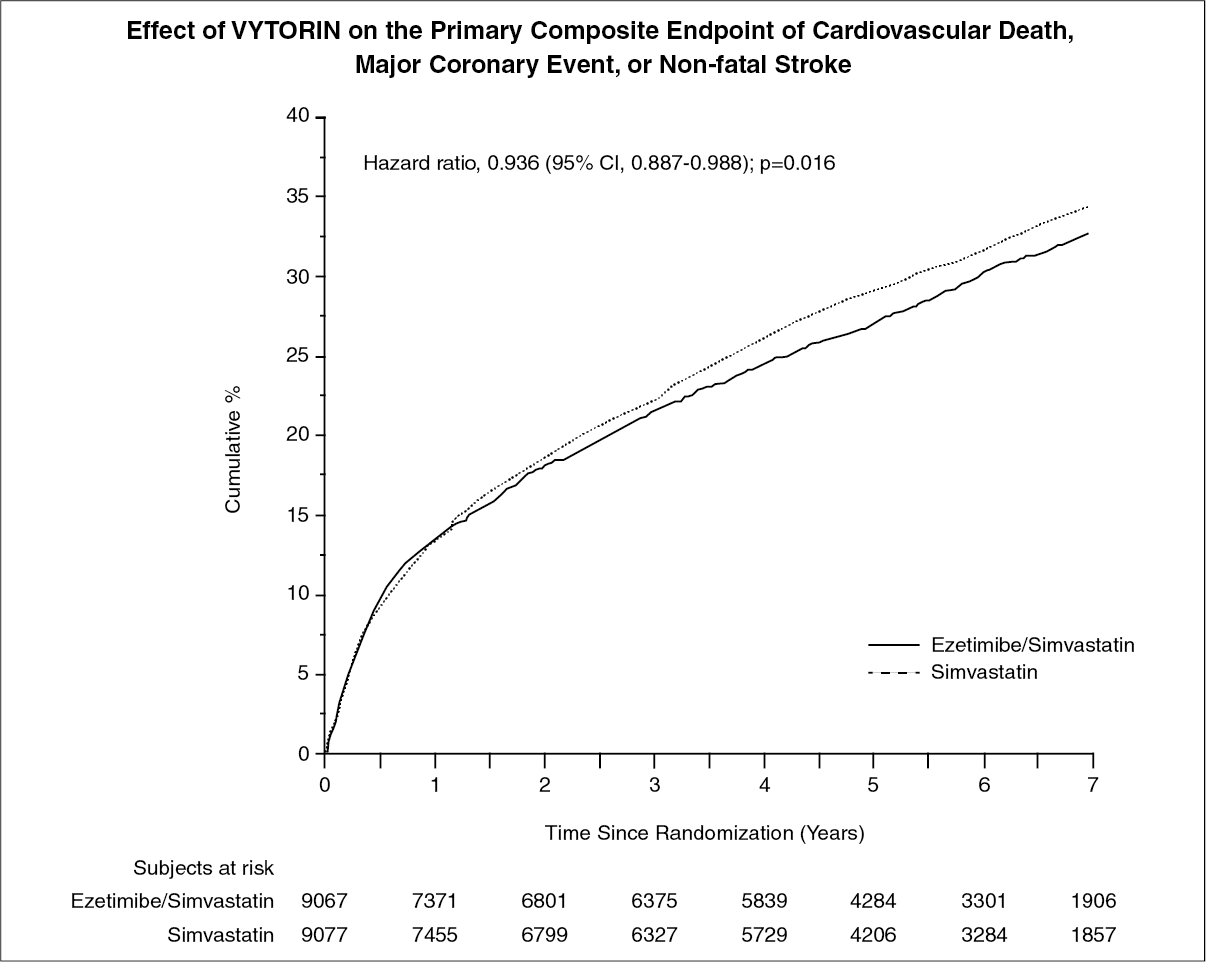
The IMProved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT) was a multicentre, randomised, double-blind, active-control study of 18,144 patients enrolled within 10 days of hospitalisation for acute coronary syndrome (ACS; either acute myocardial infarction [MI] or unstable angina [UA]). Patients had an LDL-C ≤125 mg/dL (≤3.2 mmol/L) at the time of presentation with ACS if they had not been taking lipid-lowering therapy, or ≤100 mg/dL (≤2.6 mmol/L) if they had been receiving lipid-lowering therapy. All patients were randomised in a 1:1 ratio to receive either ezetimibe/simvastatin 10/40 mg (n=9067) or simvastatin 40 mg (n=9077) and followed for a median of 6.0 years.
Patients had a mean age of 63.6 years; 76% were male, 84% were Caucasian, and 27% were diabetic. The average LDL-C value at the time of study qualifying event was 80 mg/dL (2.1 mmol/L) for those on lipid-lowering therapy (n=6390) and 101 mg/dL (2.6 mmol/L) for those not on previous lipid-lowering therapy (n=11594). Prior to the hospitalisation for the qualifying ACS event, 34% of the patients were on statin therapy. At one year, the average LDL-C for patients continuing on therapy was 53.2 mg/dL (1.4 mmol/L) for the VYTORIN group and 69.9 mg/dL (1.8 mmol/L) for the simvastatin monotherapy group. Lipid values were generally obtained for patients who remained on study therapy.
The primary endpoint was a composite consisting of cardiovascular death, major coronary events (MCE; defined as non-fatal myocardial infarction, documented unstable angina that required hospitalisation, or any coronary revascularisation procedure occurring at least 30 days after randomised treatment assignment) and non-fatal stroke. The study demonstrated that treatment with VYTORIN provided incremental benefit in reducing the primary composite endpoint of cardiovascular death, MCE, and non-fatal stroke compared with simvastatin alone (relative risk reduction of 6.4%, p=0.016). The primary endpoint occurred in 2572 of 9067 patients (7-year Kaplan-Meier [KM] rate 32.72%) in the VYTORIN group and 2742 of 9077 patients (7-year KM rate 34.67%) in the simvastatin alone group. (See figure and Table 1.) Total mortality was unchanged in this high risk group (see Table 1).
There was an overall benefit for all strokes; however there was a small non-significant increase in hemorrhagic stroke in the ezetimibe-simvastatin group compared with simvastatin alone (see Table 1). The risk of hemorrhagic stroke for ezetimibe co-administered with higher potency statins in long-term outcome studies has not been evaluated.
The treatment effect of ezetimibe/simvastatin was generally consistent with the overall results across many subgroups, including sex, age, race, medical history of diabetes mellitus, baseline lipid levels, prior statin therapy, prior stroke, and hypertension. (See figure and Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Primary Hypercholesterolaemia: In a double-blind, placebo-controlled, 8-week study, 240 patients with hypercholesterolaemia already receiving simvastatin monotherapy and not at National Cholesterol Education Program (NCEP) LDL-C goal (2.6 to 4.1 mmol/l [100 to 160 mg/dl], depending on baseline characteristics) were randomised to receive either ezetimibe 10 mg or placebo in addition to their on-going simvastatin therapy. Among simvastatin-treated patients not at LDL-C goal at baseline (~80%), significantly more patients randomised to ezetimibe co-administered with simvastatin achieved their LDL-C goal at study endpoint compared to patients randomised to placebo co-administered with simvastatin, 76% and 21.5%, respectively.
The corresponding LDL-C reductions for ezetimibe or placebo co-administered with simvastatin were also significantly different (27% or 3%, respectively). In addition, ezetimibe co-administered with simvastatin significantly decreased total-C, Apo B, and TG compared with placebo co-administered with simvastatin.
In a multicentre, double-blind, 24-week trial, 214 patients with type 2 diabetes mellitus treated with thiazolidinediones (rosiglitazone or pioglitazone) for a minimum of 3 months and simvastatin 20 mg for a minimum of 6 weeks with a mean LDL-C of 2.4 mmol/L (93 mg/dl), were randomised to receive either simvastatin 40 mg or the co-administered active ingredients equivalent to VYTORIN 10 mg/20 mg. VYTORIN 10 mg/20 mg was significantly more effective than doubling the dose of simvastatin to 40 mg in further reducing LDL-C (-21% and 0%, respectively), total-C (-14% and -1%, respectively), Apo B (-14% and -2%, respectively), and non-HDL-C (-20% and -2%, respectively) beyond the reductions observed with simvastatin 20 mg. Results for HDL-C and TG between the two treatment groups were not significantly different. Results were not affected by type of thiazolidinedione treatment.
The efficacy of the different dose-strengths of VYTORIN (10/10 to 10/80 mg/day) was demonstrated in a multicentre, double-blind, placebo-controlled 12-week trial that included all available doses of VYTORIN and all relevant doses of simvastatin. When patients receiving all doses of VYTORIN were compared to those receiving all doses of simvastatin, VYTORIN significantly lowered total-C, LDL-C, and TG (see Table 2) as well as Apo B (-42% and -29%, respectively), non-HDL-C (-49% and -34%, respectively) and C-reactive protein (-33% and -9%, respectively). The effects of VYTORIN on HDL-C were similar to the effects seen with simvastatin. Further analysis showed VYTORIN significantly increased HDL-C compared with placebo. (See Table 2.)
Click on icon to see table/diagram/image
In a similarly designed study, results for all lipid parameters were generally consistent. In a pooled analysis of these two studies, the lipid response to VYTORIN was similar in patients with TG levels greater than or less than 200 mg/dl.
In a multicentre, double-blind, controlled clinical study (ENHANCE), 720 patients with heterozygous familial hypercholesterolaemia were randomised to receive ezetimibe 10 mg in combination with simvastatin 80 mg (n = 357) or simvastatin 80 mg (n = 363) for 2 years. The primary objective of the study was to investigate the effect of the ezetimibe/simvastatin combination therapy on carotid artery intima-media thickness (IMT) compared to simvastatin monotherapy. The impact of this surrogate marker on cardiovascular morbidity and mortality is still not demonstrated.
The primary endpoint, the change in the mean IMT of all six carotid segments, did not differ significantly (p= 0.29) between the two treatment groups as measured by B-mode ultrasound. With ezetimibe 10 mg in combination with simvastatin 80 mg or simvastatin 80 mg alone, intima-medial thickening increased by 0.0111 mm and 0.0058 mm, respectively, over the study's 2 year duration (baseline mean carotid IMT 0.68 mm and 0.69 mm respectively).
Ezetimibe 10 mg in combination with simvastatin 80 mg lowered LDL-C, total-C, Apo B, and TG significantly more than simvastatin 80 mg. The percent increase in HDL-C was similar for the two treatment groups. The adverse reactions reported for ezetimibe 10 mg in combination with simvastatin 80 mg were consistent with its known safety profile.
VYTORIN contains simvastatin. In two large placebo-controlled clinical trials, the Scandinavian Simvastatin Survival Study (20-40 mg; N=4,444 patients) and the Heart Protection Study (40 mg; N=20,536 patients), the effects of treatment with simvastatin were assessed in patients at high risk of coronary events because of existing coronary heart disease, diabetes, peripheral vessel disease, history of stroke or other cerebrovascular disease. Simvastatin was proven to reduce: the risk of total mortality by reducing CHD deaths; the risk of non-fatal myocardial infarction and stroke; and the need for coronary and non-coronary revascularisation procedures.
The Study of the Effectiveness of Additional Reductions in Cholesterol and Homocysteine (SEARCH) evaluated the effect of treatment with simvastatin 80 mg versus 20 mg (median follow-up 6.7 yrs) on major vascular events (MVEs; defined as fatal CHD, non-fatal MI, coronary revascularisation procedure, non-fatal or fatal stroke, or peripheral revascularisation procedure) in 12,064 patients with a history of myocardial infarction. There was no significant difference in the incidence of MVEs between the 2 groups; simvastatin 20 mg (n = 1553; 25.7 %) vs. simvastatin 80 mg (n = 1477; 24.5 %); RR 0.94, 95 % CI: 0.88 to 1.01. The absolute difference in LDL-C between the two groups over the course of the study was 0.35 ± 0.01 mmol/L. The safety profiles were similar between the two treatment groups except that the incidence of myopathy was approximately 1.0 % for patients on simvastatin 80 mg compared with 0.02 % for patients on 20 mg. Approximately half of these myopathy cases occurred during the first year of treatment. The incidence of myopathy during each subsequent year of treatment was approximately 0.1 %.
Paediatric population: In a multicentre, double-blind, controlled study, 142 boys (Tanner stage II and above) and 106 post-menarchal girls, 10 to 17 years of age (mean age 14.2 years) with heterozygous familial hypercholesterolaemia (HeFH) with baseline LDL-C levels between 4.1 and 10.4 mmol/l were randomised to either ezetimibe 10 mg co-administered with simvastatin (10, 20 or 40 mg) or simvastatin (10, 20 or 40 mg) alone for 6 weeks, co-administered ezetimibe and 40 mg simvastatin or 40 mg simvastatin alone for the next 27 weeks, and open-label co-administered ezetimibe and simvastatin (10 mg, 20 mg, or 40 mg) for 20 weeks thereafter.
At Week 6, ezetimibe co-administered with simvastatin (all doses) significantly reduced total-C (38 % vs 26 %), LDL-C (49 % vs 34 %), Apo B (39 % vs 27 %), and non-HDL-C (47 % vs 33 %) compared to simvastatin (all doses) alone. Results for the two treatment groups were similar for TG and HDL-C (-17 % vs -12 % and +7 % vs +6 %, respectively). At Week 33, results were consistent with those at Week 6 and significantly more patients receiving ezetimibe and 40 mg simvastatin (62 %) attained the NCEP AAP ideal goal (< 2.8 mmol/L [110 mg/dL]) for LDL-C compared to those receiving 40 mg simvastatin (25 %). At Week 53, the end of the open label extension, the effects on lipid parameters were maintained.
The safety and efficacy of ezetimibe co-administered with doses of simvastatin above 40 mg daily have not been studied in paediatric patients 10 to 17 years of age. The long-term efficacy of therapy with ezetimibe in patients below 17 years of age to reduce morbidity and mortality in adulthood has not been studied.
The European Medicines Agency has waived the obligation to submit the results of studies with VYTORIN in all subsets of the paediatric population in Hypercholesterolaemia (see Dosage & Administration for information on paediatric use).
Homozygous Familial Hypercholesterolaemia (HoFH): A double-blind, randomised, 12-week study was performed in patients with a clinical and/or genotypic diagnosis of HoFH. Data were analysed from a subgroup of patients (n=14) receiving simvastatin 40 mg at baseline. Increasing the dose of simvastatin from 40 to 80 mg (n=5) produced a reduction of LDL-C of 13% from baseline on simvastatin 40 mg. Co-administered ezetimibe and simvastatin equivalent to VYTORIN (10 mg/40 mg and 10 mg/80 mg pooled, n=9), produced a reduction of LDL-C of 23% from baseline on simvastatin 40 mg. In those patients co-administered ezetimibe and simvastatin equivalent to VYTORIN (10 mg/80 mg, n=5), a reduction of LDL-C of 29% from baseline on simvastatin 40 mg was produced.
Prevention of Major Vascular Events in Chronic Kidney Disease (CKD): The Study of Heart and Renal Protection (SHARP) was a multi-national, randomised, placebo-controlled, double-blind study conducted in 9438 patients with chronic kidney disease, a third of whom were on dialysis at baseline. A total of 4650 patients were allocated to VYTORIN 10/20 and 4620 to placebo, and followed for a median of 4.9 years. Patients had a mean age of 62 and 63 % were male, 72 % Caucasian, 23 % diabetic and, for those not on dialysis, the mean estimated glomerular filtration rate (eGFR) was 26.5 ml/min/1.73 m
2. There were no lipid entry criteria. Mean LDL-C at baseline was 108 mg/dL. After one year, including patients no longer taking study medication, LDL-C was reduced 26 % relative to placebo by simvastatin 20 mg alone and 38 % by VYTORIN 10/20 mg.
The SHARP protocol-specified primary comparison was an intention-to-treat analysis of "major vascular events" (MVE; defined as non-fatal MI or cardiac death, stroke, or any revascularisation procedure) in only those patients initially randomised to the VYTORIN (n=4193) or placebo (n=4191) groups. Secondary analyses included the same composite analysed for the full cohort randomised (at study baseline or at year 1) to VYTORIN (n=4650) or placebo (n=4620) as well as the components of this composite.
The primary endpoint analysis showed that VYTORIN significantly reduced the risk of major vascular events (749 patients with events in the placebo group vs. 639 in the VYTORIN group) with a relative risk reduction of 16 % (p=0.001).
Nevertheless, this study design did not allow for a separate contribution of the monocomponent ezetimibe to efficacy to significantly reduce the risk of major vascular events in patients with CKD.
The individual components of MVE in all randomised patients are presented in Table 3. VYTORIN significantly reduced the risk of stroke and any revascularisation, with non-significant numerical differences favouring VYTORIN for non-fatal MI and cardiac death. (See Table 3.)
Click on icon to see table/diagram/image
The absolute reduction in LDL cholesterol achieved with VYTORIN was lower among patients with a lower baseline LDL-C (<2.5 mmol/l) and patients on dialysis at baseline than the other patients, and the corresponding risk reductions in these two groups were attenuated.
Aortic Stenosis: The Simvastatin and Ezetimibe for the Treatment of Aortic Stenosis (SEAS) study was a multicentre, double-blind, placebo-controlled study with a median duration of 4.4 years conducted in 1873 patients with asymptomatic aortic stenosis (AS), documented by Doppler-measured aortic peak flow velocity within the range of 2.5 to 4.0 m/s. Only patients who were considered not to require statin treatment for purposes of reducing atherosclerotic cardiovascular disease risk were enrolled. Patients were randomised 1:1 to receive placebo or co-administered ezetimibe 10 mg and simvastatin 40 mg daily.
The primary endpoint was the composite of major cardiovascular events (MCE) consisting of cardiovascular death, aortic valve replacement (AVR) surgery, congestive heart failure (CHF) as a result of progression of AS, non-fatal myocardial infarction, coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), hospitalisation for unstable angina, and non-hemorrhagic stroke. The key secondary endpoints were composites of subsets of the primary endpoint event categories.
Compared to placebo, ezetimibe/simvastatin 10/40 mg did not significantly reduce the risk of MCE. The primary outcome occurred in 333 patients (35.3%) in the ezetimibe / simvastatin group and in 355 patients (38.2%) in the placebo group (hazard ratio in the ezetimibe / simvastatin group, 0.96; 95% confidence interval, 0.83 to 1.12; p = 0.59). Aortic valve replacement was performed in 267 patients (28.3%) in the ezetimibe / simvastatin group and in 278 patients (29.9%) in the placebo group (hazard ratio, 1.00; 95% CI, 0.84 to 1.18; p = 0.97). Fewer patients had ischemic cardiovascular events in the ezetimibe / simvastatin group (n=148) than in the placebo group (n=187) (hazard ratio, 0.78; 95% CI, 0.63 to 0.97; p = 0.02), mainly because of the smaller number of patients who underwent coronary artery bypass grafting.
Cancer occurred more frequently in the ezetimibe / simvastatin group (105 versus 70, p = 0.01). The clinical relevance of this observation is uncertain as in the bigger SHARP trial the total number of patients with any incident cancer (438 in the ezetimibe / simvastatin versus 439 placebo group) did not differ. In addition, in the IMPROVE-IT trial the total number of patients with any new malignancy (853 in the ezetimibe / simvastatin group versus 863 in the simvastatin group) did not differ significantly and therefore the finding of SEAS trial could not be confirmed by SHARP or IMPROVE-IT.
Pharmacokinetics: No clinically significant pharmacokinetic interaction was seen when ezetimibe was co-administered with simvastatin.
Absorption: VYTORIN: VYTORIN is bioequivalent to co-administered ezetimibe and simvastatin.
Ezetimibe: After oral administration, ezetimibe is rapidly absorbed and extensively conjugated to a pharmacologically active phenolic glucuronide (ezetimibe-glucuronide). Mean maximum plasma concentrations (C
max) occur within 1 to 2 hours for ezetimibe-glucuronide and 4 to 12 hours for ezetimibe. The absolute bioavailability of ezetimibe cannot be determined as the compound is virtually insoluble in aqueous media suitable for injection.
Concomitant food administration (high-fat or non-fat meals) had no effect on the oral bioavailability of ezetimibe when administered as 10-mg tablets.
Simvastatin: The availability of the active β-hydroxyacid to the systemic circulation following an oral dose of simvastatin was found to be less than 5% of the dose, consistent with extensive hepatic first-pass extraction. The major metabolites of simvastatin present in human plasma are the β-hydroxyacid and four additional active metabolites.
Relative to the fasting state, the plasma profiles of both active and total inhibitors were not affected when simvastatin was administered immediately before a test meal.
Distribution: Ezetimibe: Ezetimibe and ezetimibe-glucuronide are bound 99.7% and 88 to 92% to human plasma proteins, respectively.
Simvastatin: Both simvastatin and the β-hydroxyacid are bound to human plasma proteins (95%).
The pharmacokinetics of single and multiple doses of simvastatin showed that no accumulation of drug occurred after multiple dosing. In all of the previously mentioned pharmacokinetic studies, the maximum plasma concentration of inhibitors occurred 1.3 to 2.4 hours post-dose.
Biotransformation: Ezetimibe: Ezetimibe is metabolised primarily in the small intestine and liver via glucuronide conjugation (a phase II reaction) with subsequent biliary excretion. Minimal oxidative metabolism (a phase I reaction) has been observed in all species evaluated. Ezetimibe and ezetimibe-glucuronide are the major drug-derived compounds detected in plasma, constituting approximately 10 to 20% and 80 to 90% of the total drug in plasma, respectively. Both ezetimibe and ezetimibe-glucuronide are slowly eliminated from plasma with evidence of significant enterohepatic recycling. The half-life for ezetimibe and ezetimibe-glucuronide is approximately 22 hours.
Simvastatin: Simvastatin is an inactive lactone which is readily hydrolysed
in vivo to the corresponding β-hydroxyacid, a potent inhibitor of HMG-CoA reductase. Hydrolysis takes place mainly in the liver; the rate of hydrolysis in human plasma is very slow.
In man simvastatin is well absorbed and undergoes extensive hepatic first-pass extraction. The extraction in the liver is dependent on the hepatic blood flow. The liver is its primary site of action, with subsequent excretion of drug equivalents in the bile. Consequently, availability of active drug to the systemic circulation is low.
Following an intravenous injection of the β-hydroxyacid metabolite, its half-life averaged 1.9 hours.
Elimination: Ezetimibe: Following oral administration of
14C-ezetimibe (20 mg) to human subjects, total ezetimibe accounted for approximately 93% of the total radioactivity in plasma. Approximately 78% and 11% of the administered radioactivity were recovered in the faeces and urine, respectively, over a 10-day collection period. After 48 hours, there were no detectable levels of radioactivity in the plasma.
Simvastatin: Simvastatin acid is taken up actively into the hepatocytes by the transporter OATP1B1.
Simvastatin is a substrate of the efflux transporter BCRP.
Following an oral dose of radioactive simvastatin to man, 13% of the radioactivity was excreted in the urine and 60% in the faeces within 96 hours. The amount recovered in the faeces represents absorbed drug equivalents excreted in bile as well as unabsorbed drug. Following an intravenous injection of the β-hydroxyacid metabolite, an average of only 0.3% of the IV dose was excreted in urine as inhibitors.
Special Populations: Paediatric Population: The absorption and metabolism of ezetimibe are similar between children and adolescents (10 to 18 years) and adults. Based on total ezetimibe, there are no pharmacokinetic differences between adolescents and adults. Pharmacokinetic data in the paediatric population < 10 years of age are not available. Clinical experience in paediatric and adolescent patients includes patients with HoFH, HeFH, or sitosterolaemia. (See Dosage & Administration.)
Elderly: Plasma concentrations for total ezetimibe are about 2-fold higher in the elderly (≥65 years) than in the young (18 to 45 years). LDL-C reduction and safety profile are comparable between elderly and younger subjects treated with ezetimibe. (See Dosage & Administration.)
Hepatic impairment: After a single 10-mg dose of ezetimibe, the mean AUC for total ezetimibe was increased approximately 1.7-fold in patients with mild hepatic impairment (Child-Pugh score 5 or 6), compared to healthy subjects. In a 14-day, multiple-dose study (10 mg daily) in patients with moderate hepatic impairment (Child-Pugh score 7 to 9), the mean AUC for total ezetimibe was increased approximately 4-fold on Day 1 and Day 14 compared to healthy subjects. No dosage adjustment is necessary for patients with mild hepatic impairment. Due to the unknown effects of the increased exposure to ezetimibe in patients with moderate or severe (Child-Pugh score > 9) hepatic impairment, ezetimibe is not recommended in these patients (see Dosage & Administration and Precautions).
Renal impairment: Ezetimibe: After a single 10-mg dose of ezetimibe in patients with severe renal disease (n=8; mean CrCl ≤30 ml/min), the mean AUC for total ezetimibe was increased approximately 1.5-fold, compared to healthy subjects (n=9). (See Dosage & Administration.)
An additional patient in this study (post-renal transplant and receiving multiple medications, including ciclosporin) had a 12-fold greater exposure to total ezetimibe.
Simvastatin: In a study of patients with severe renal impairment (creatinine clearance < 30 ml/min), the plasma concentrations of total inhibitors after a single dose of a related HMG-CoA reductase inhibitor were approximately two-fold higher than those in healthy volunteers.
Gender: Plasma concentrations for total ezetimibe are slightly higher (approximately 20%) in women than in men. LDL-C reduction and safety profile are comparable between men and women treated with ezetimibe.
SLCO1B1 polymorphism: Carriers of the SLCO1B1 gene c.521T>C allele have lower OATP1B1 activity. The mean exposure (AUC) of the main active metabolite, simvastatin acid is 120% in heterozygote carriers (CT) of the C allele and 221% in homozygote (CC) carriers relative to that of patients who have the most common genotype (TT). The C allele has a frequency of 18% in the European population. In patients with SLCO1B1 polymorphism there is a risk of increased exposure of simvastatin acid, which may lead to an increased risk of rhabdomyolysis (see Precautions).
Toxicology: Preclinical safety data: VYTORIN: In co-administration studies with ezetimibe and simvastatin, the toxic effects observed were essentially those typically associated with statins. Some of the toxic effects were more pronounced than observed during treatment with statins alone. This is attributed to pharmacokinetic and/or pharmacodynamic interactions following co-administration. No such interactions occurred in the clinical studies. Myopathies occurred in rats only after exposure to doses that were several times higher than the human therapeutic dose (approximately 20 times the AUC level for simvastatin and 1800 times the AUC level for the active metabolite). There was no evidence that co-administration of ezetimibe affected the myotoxic potential of simvastatin.
In dogs co-administered ezetimibe and statins, some liver effects were observed at low exposures (≤1 times human AUC). Marked increases in liver enzymes (ALT, AST) in the absence of tissue necrosis were seen. Histopathologic liver findings (bile duct hyperplasia, pigment accumulation, mononuclear cell infiltration and small hepatocytes) were observed in dogs co-administered ezetimibe and simvastatin. These changes did not progress with longer duration of dosing up to 14 months. General recovery of the liver findings was observed upon discontinuation of dosing. These findings were consistent with those described with HMG-CoA inhibitors or attributed to the very low cholesterol levels achieved in the affected dogs.
The co-administration of ezetimibe and simvastatin was not teratogenic in rats. In pregnant rabbits a small number of skeletal deformities (fused caudal vertebrae, reduced number of caudal vertebrae) were observed.
In a series of
in vivo and
in vitro assays, ezetimibe, given alone or co-administered with simvastatin, exhibited no genotoxic potential.
Ezetimibe: Animal studies on the chronic toxicity of ezetimibe identified no target organs for toxic effects. In dogs treated for four weeks with ezetimibe (≥0.03 mg/kg/day) the cholesterol concentration in the cystic bile was increased by a factor of 2.5 to 3.5. However, in a one year study on dogs given doses of up to 300 mg/kg/day no increased incidence of cholelithiasis or other hepatobiliary effects were observed. The significance of these data for humans is not known. A lithogenic risk associated with the therapeutic use of ezetimibe cannot be ruled out.
Long-term carcinogenicity tests on ezetimibe were negative.
Ezetimibe had no effect on the fertility of male or female rats, nor was it found to be teratogenic in rats or rabbits, nor did it affect prenatal or post-natal development. Ezetimibe crossed the placental barrier in pregnant rats and rabbits given multiple doses of 1000 mg/kg/day.
Simvastatin: Based on conventional animal studies regarding pharmacodynamics, repeated dose toxicity, genotoxicity and carcinogenicity, there are no other risks for the patient than may be expected on account of the pharmacological mechanism. At maximally tolerated doses in both the rat and the rabbit, simvastatin produced no foetal malformations, and had no effects on fertility, reproductive function or neonatal development.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image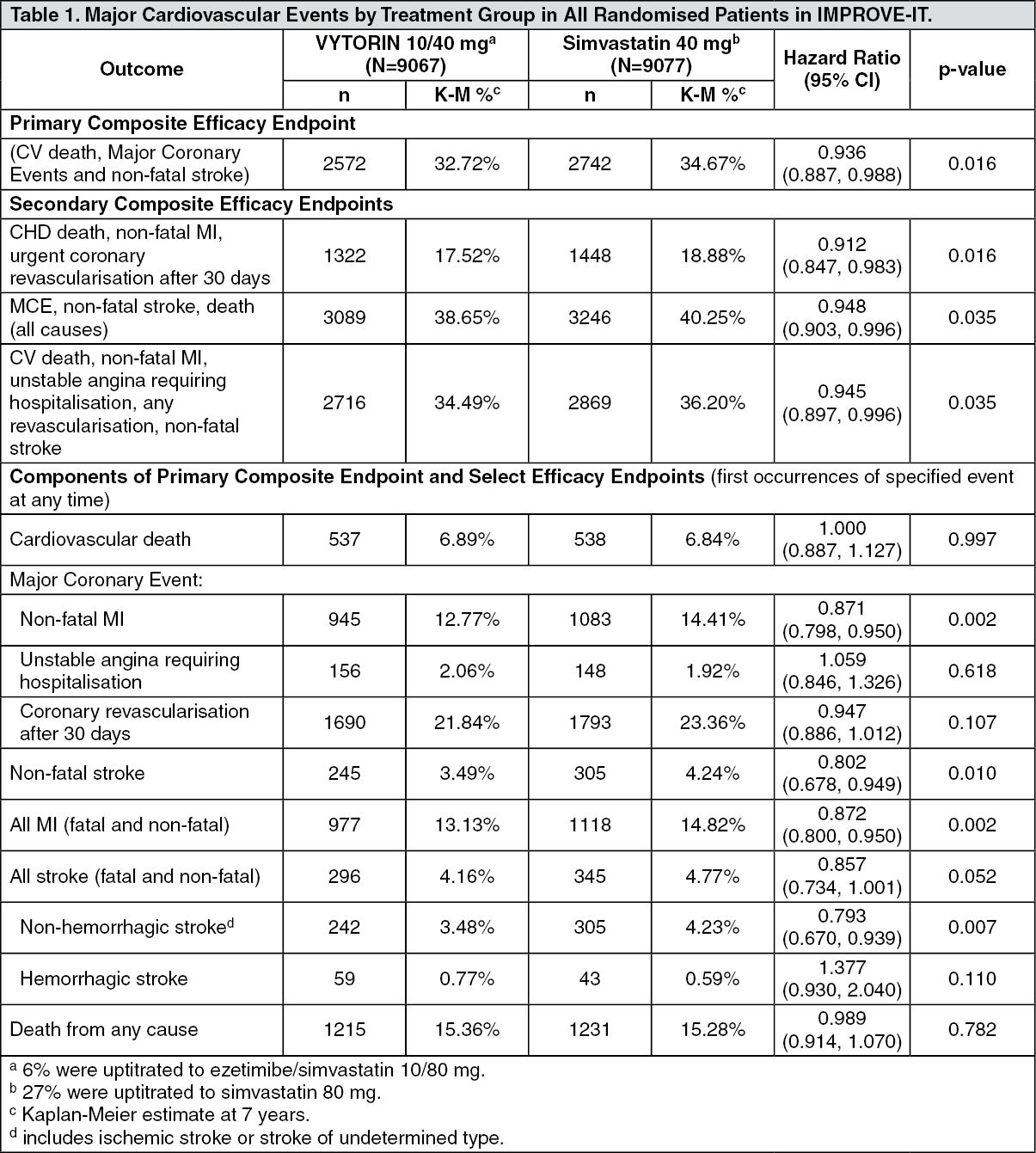 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image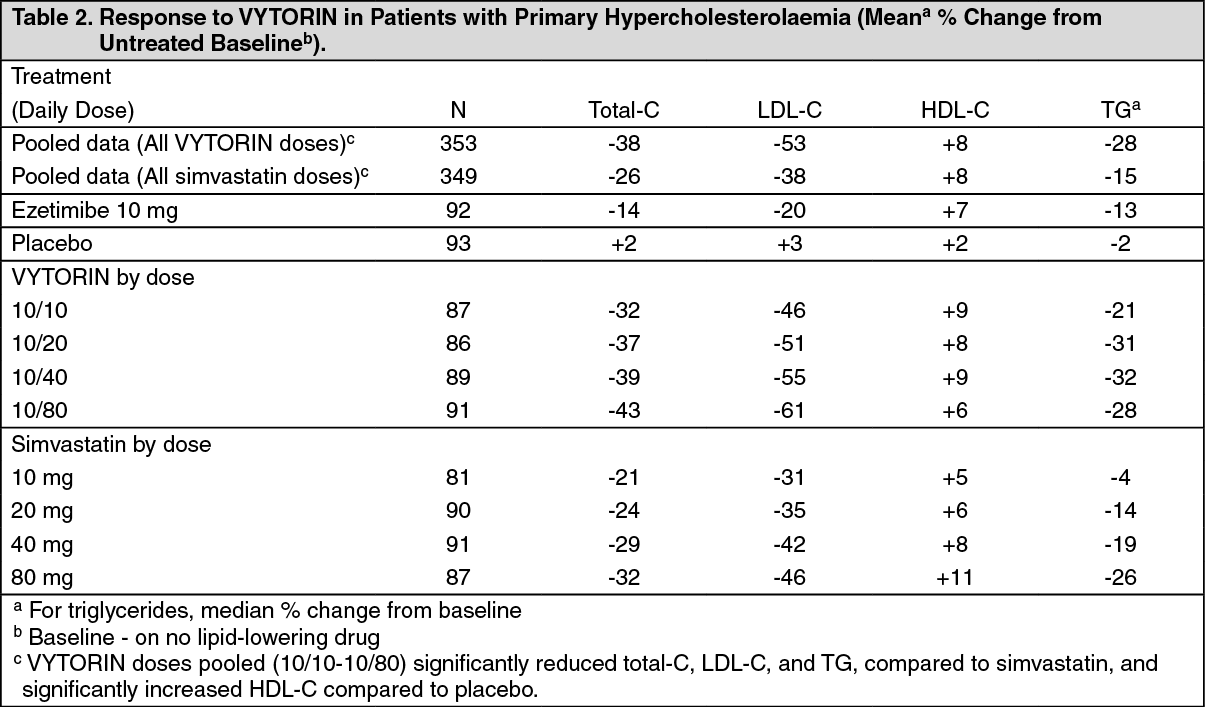 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image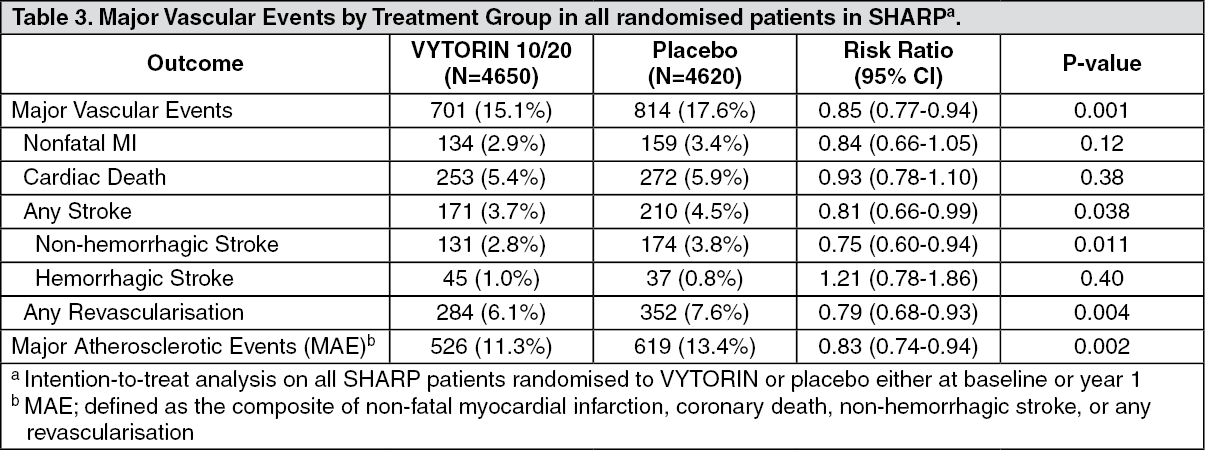 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
