Pharmacology: Mechanism of Action: The active moiety of Xofigo is the alpha-particle emitting isotope radium-223 (as radium Ra 223 dichloride), which mimics calcium and forms complexes with the bone mineral hydroxyapatite at areas of increased bone turnover, such as bone metastases (see Table 2). The high linear energy transfer of alpha emitters (80 keV/micrometer) leads to a high frequency of double-strand DNA breaks in adjacent cells, resulting in an anti-tumor effect on bone metastases. The alpha particle range from radium-223 dichloride is less than 100 micrometers (less than 10 cell diameters) which limits damage to the surrounding normal tissue.
Pharmacodynamics: Compared with placebo, there was a significant difference in favor of Xofigo for all five serum biomarkers for bone turnover studied in a phase 2 randomized study (bone formation markers: bone alkaline phosphatase [ALP], total ALP and procollagen I N propeptide [PINP], bone resorption markers: C-terminal crosslinking telopeptide of type I collagen [S-CTX-I] and type I collagen crosslinked C-telopeptide [ICTP]).
Clinical Studies: The efficacy and safety of Xofigo were evaluated in a double-blind, randomized, placebo-controlled phase 3 clinical trial of patients with castration-resistant prostate cancer with symptomatic bone metastases. Patients with visceral metastases and malignant lymphadenopathy exceeding 3 cm were excluded. The primary efficacy endpoint was overall survival. A key secondary efficacy endpoint was time to first symptomatic skeletal event (SSE) defined as external beam radiation therapy (EBRT) to relieve skeletal symptoms, new symptomatic pathologic bone fracture, occurrence of spinal cord compression, or tumor-related orthopedic surgical intervention. There were no scheduled radiographic assessments performed on study. All patients were to continue androgen deprivation therapy. At the cut-off date of the pre-planned interim analysis, a total of 809 patients had been randomized 2:1 to receive Xofigo 55 kBq (1.49 microcurie)/kg intravenously every 4 weeks for 6 cycles (n = 541) plus best standard of care or matching placebo plus best standard of care (n = 268). Best standard of care included local EBRT, corticosteroids, antiandrogens, estrogens, estramustine or ketoconazole. Therapy was continued until unacceptable toxicity or initiation of cytotoxic chemotherapy, other systemic radioisotope, hemi-body EBRT or other investigational drug. Patients with Crohn's disease, ulcerative colitis, prior hemibody radiation or untreated imminent spinal cord compression were excluded from the study. In patients with bone fractures, orthopedic stabilization was performed before starting or resuming treatment with Xofigo.
The following patient demographics and baseline diseases characteristics were balanced between the arms. The median age was 71 (range 44-94) with a racial distribution of 94% Caucasian, 4% Asian, 2% Black and <1% Other. Patients were enrolled predominantly from Europe (85%) with 4% of patients enrolled from North America. ECOG performance status was 0-1 in 86% of patients. Eighty-five percent of patients had 6 or more bone scan lesions and of those 40% had > 20 lesions or a superscan. Opiate pain medications were used for cancer-related pain in 54% of patients, non-opiate pain medications in 44% of patients and no pain medications in 2% of patients. Patients were stratified by baseline ALP, biphosphonate use, and prior docetaxel exposure. Prior biphosphonates were used by 41% of patients and 58% had received prior docetaxel. During the treatment period, 83% of Xofigo patients and 82% of placebo patients received gonadotropin-releasing hormone agonists and 21% of Xofigo patients and 34% of placebo patients received concomitant antiandrogens. Use of systemic steroids (41%) and biphosphonates (40%) was balanced between the arms.
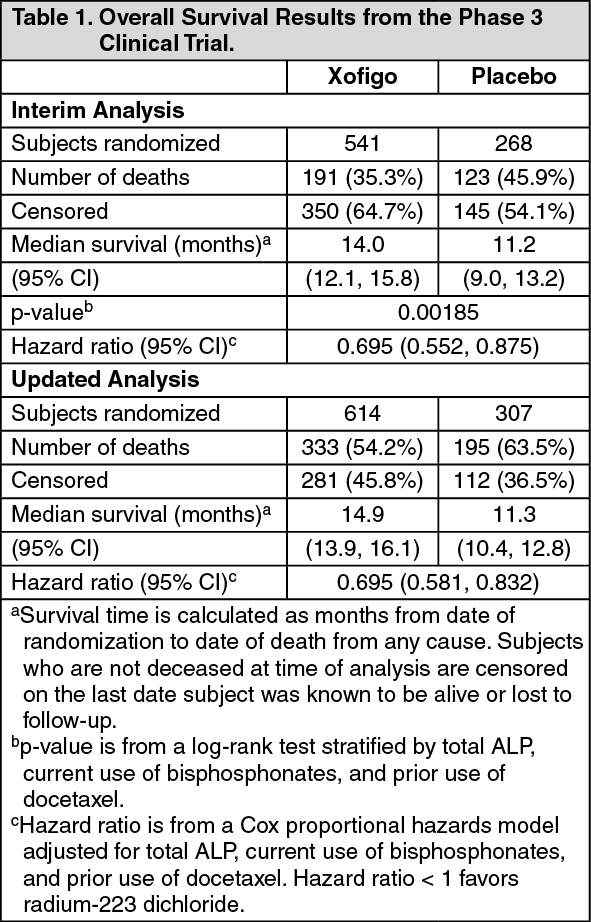
The pre-specified interim analysis of overall survival revealed a statistically significant improvement in patients receiving XOFIGO plus best standard of care compared with patients receiving placebo plus best standard of care. An exploratory updated overall survival analysis performed before patient crossover with an additional 214 events resulted in findings consistent with the interim analysis (Table 1). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The Kaplan-Meier curves for overall survival based on the updated survival results are shown in figure. (See figure.)
Click on icon to see table/diagram/image
The survival results were supported by a delay in the time to first SSE favoring the Xofigo arm. The majority of events consisted of external beam radiotherapy to bone metastases.
Pharmacokinetics: The pharmacokinetics of radium-223 dichloride in blood was linear in terms of dose proportionality and time independence in the dose range investigated (51 to 276 kBq [1.38 to 7.46 microcurie] per kg body weight).
Distribution: After intravenous injection, radium-223 is rapidly cleared from the blood and is distributed primarily into bone or is excreted into intestine. Fifteen minutes post-injection, about 20% of the injected radioactivity remained in blood. At 4 hours, about 4% of the injected radioactivity remained in blood, decreasing to less than 1% at 24 hours after the injection. At 10 minutes post-injection, radioactivity was observed in bone and in intestine. At 4 hours post-injection, the percentage of the radioactive dose present in bone and intestine was approximately 61% and 49%, respectively. No significant uptake was seen in other organs such as heart, liver, kidneys, urinary bladder, and spleen at 4 hours post-injection (see Dosage and Administration).
Metabolism: Radium-223 is an isotope that decays and is not metabolized.
Elimination: The whole body measurements indicated that approximately 63% of the administered radioactivity was excreted from the body within 7 days after injection (after correcting for decay). Fecal excretion is the major route of elimination from the body. At 48 hours after injection, the cumulative fecal excretion was 13% (range 0 - 34%), and the cumulative urine excretion was 2% (range 1 - 5%). There was no evidence of hepato-biliary excretion based on imaging data.
The rate of elimination of radium-223 dichloride from the gastrointestinal tract is influenced by the high variability in intestinal transit rates across the population. Patients with a slower intestinal transit rate could potentially receive a higher intestinal radiation exposure. It is not known whether this will result in increased gastrointestinal activity.
Special Populations: Pediatric patients: Safety and effectiveness of Xofigo have not been established in children and adolescents below 18 years of age.
Patients with hepatic impairment: No dedicated pharmacokinetic study in patients with hepatic impairment has been conducted. However, since radium-223 is not metabolized and there is no evidence of hepato-biliary excretion based on imaging data, hepatic impairment is not expected to affect the pharmacokinetics of radium-223 dichloride.
Patients with renal impairment: No dedicated pharmacokinetic study in patients with renal impairment has been conducted. However, since excretion in urine is minimal and the major route of elimination is via the feces, renal impairment is not expected to affect the pharmacokinetics of radium-223 dichloride.
Cardiac Electrophysiology: The effect of a single dose of 55 kBq/kg of radium-223 dichloride on the QTc interval was evaluated in a subgroup of 29 patients (21 received Xofigo and 8 received placebo) in the randomized clinical trial. No large changes in the mean QTc interval (i.e., greater than 20 ms) were detected up to 6 hours post-dose. The potential for delayed effects on the QT interval after 6 hours was not evaluated.
Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Animal studies have not been conducted to evaluate the carcinogenic potential of radium-223 dichloride. However, in repeat-dose toxicity studies in rats, osteosarcomas, a known effect of bone-seeking radionuclides, were observed at clinically relevant doses 7 to 12 months after the start of treatment. The presence of other neoplastic changes, including lymphoma and mammary gland carcinoma, was also reported in 12- to 15-month repeat-dose toxicity studies in rats.
Genetic toxicology studies have not been conducted with radium-223 dichloride. However, the mechanism of action of radium-223 dichloride involves induction of double-strand DNA breaks, which is a known effect of radiation.
Animal studies have not been conducted to evaluate the effects of radium-223 dichloride on male or female fertility or reproductive function. Xofigo may impair fertility and reproductive function in humans based on its mechanism of action.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image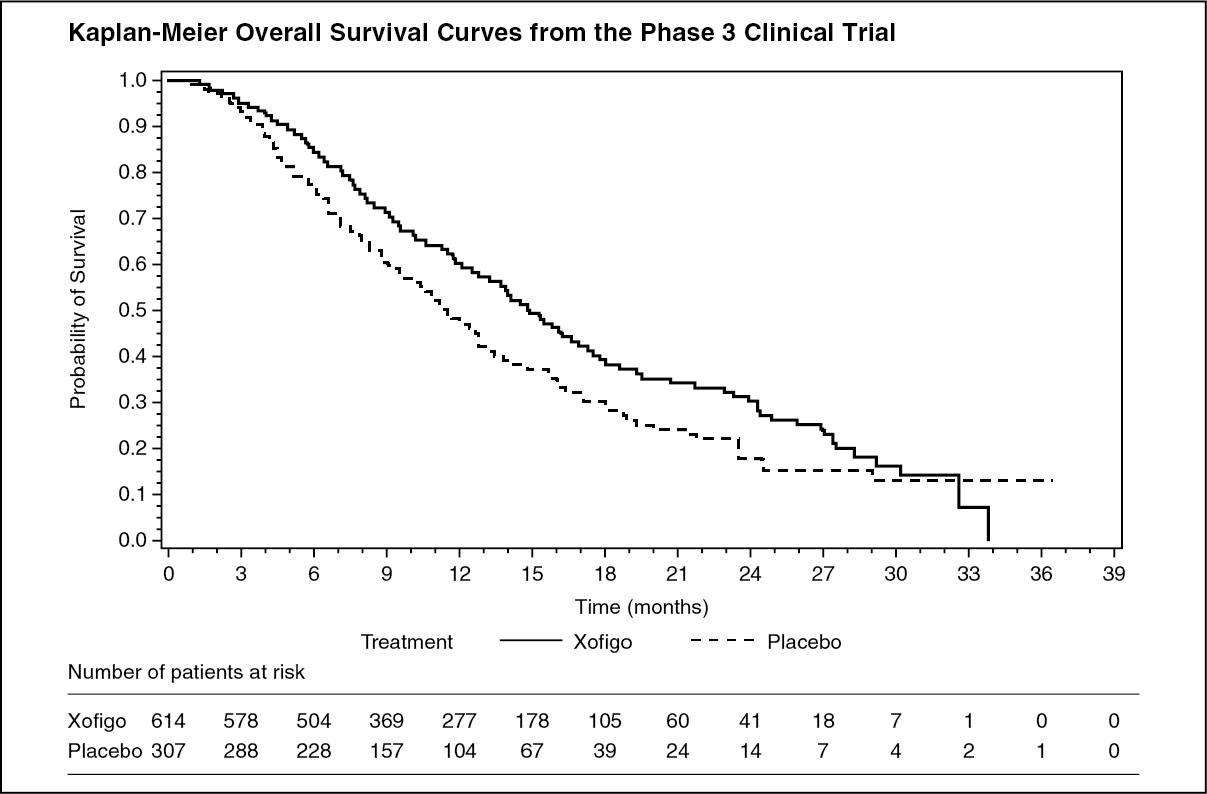 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image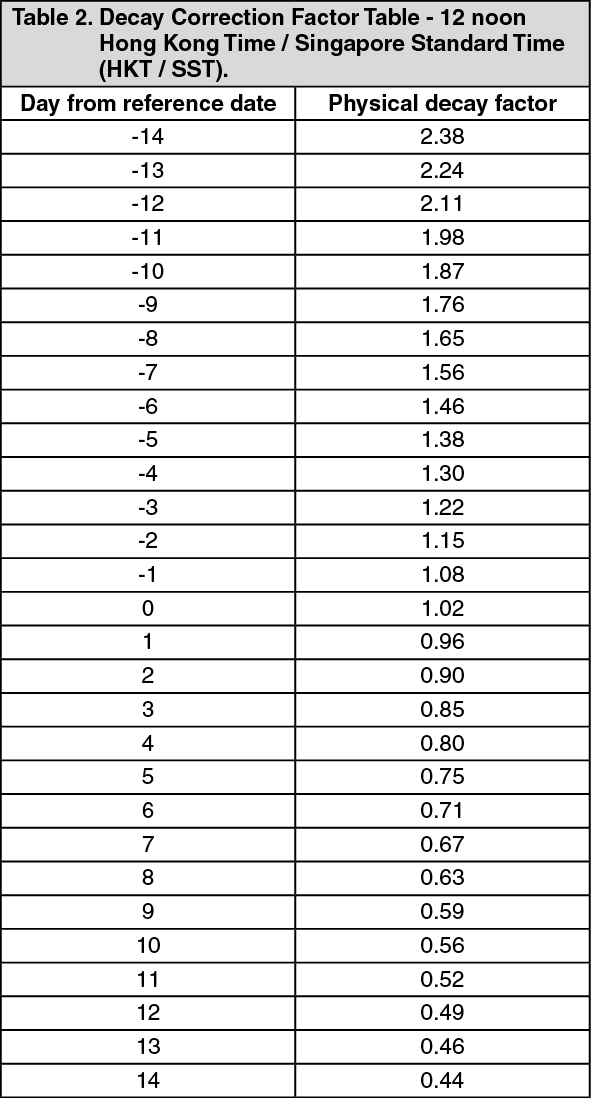 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image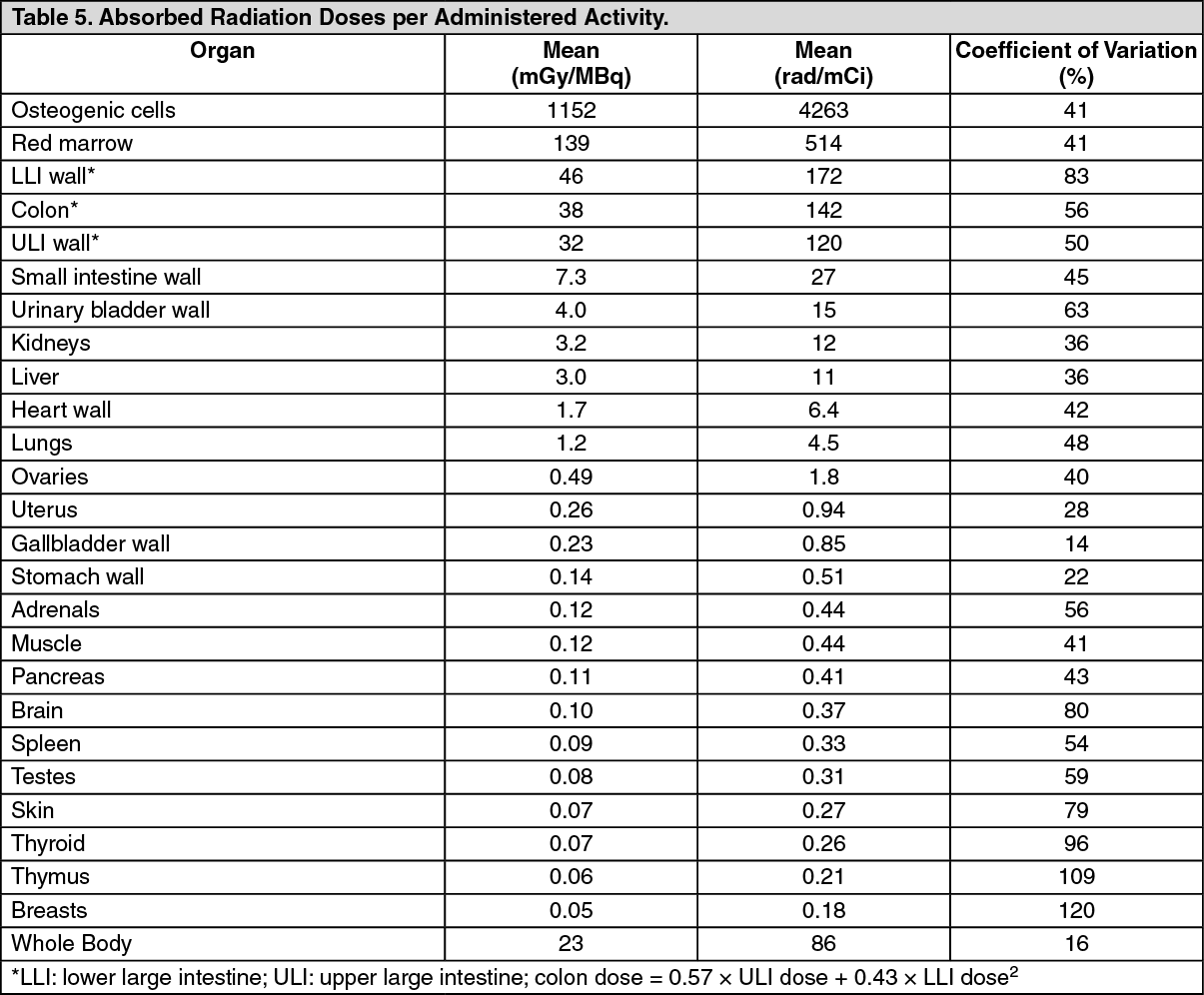 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out