
Content on this page:
Content:
Introduction
Dementia is a clinical syndrome characterized by impairment of ≥1 cognitive functions that include memory, orientation, calculation, language, judgement, executive function, visuo-spatial function and visuo-motor. May be due to various etiologies, such as Alzheimer’s disease (AD), cerebrovascular disease, other neurodegenerative conditions (eg Parkinson’s disease dementia, dementia with Lewey bodies [DLB]) and other diseases affecting the brain.
Epidemiology
As of 2023, more than 55 million people suffer from dementia, with over 60% living in low-and middle-income countries. Nearly 10 million cases are diagnosed every year. It is predicted that by 2030, the number will increase to as much as 82 million, and more than 130 million by 2050. Currently, the age-standardized prevalence of dementia ranges from 5-7%, with women being more disproportionately affected. In Asia, there are 22.9 million people living with dementia, with as many as 3.6 million people being affected in Southeast Asia. This number is expected to balloon to 12.09 million by 2050.
Pathophysiology
The pathophysiology of dementia is complex and
multifactorial. The final pathway involves the accumulation and aggregation of
products, including misfolded proteins, and/or the association with
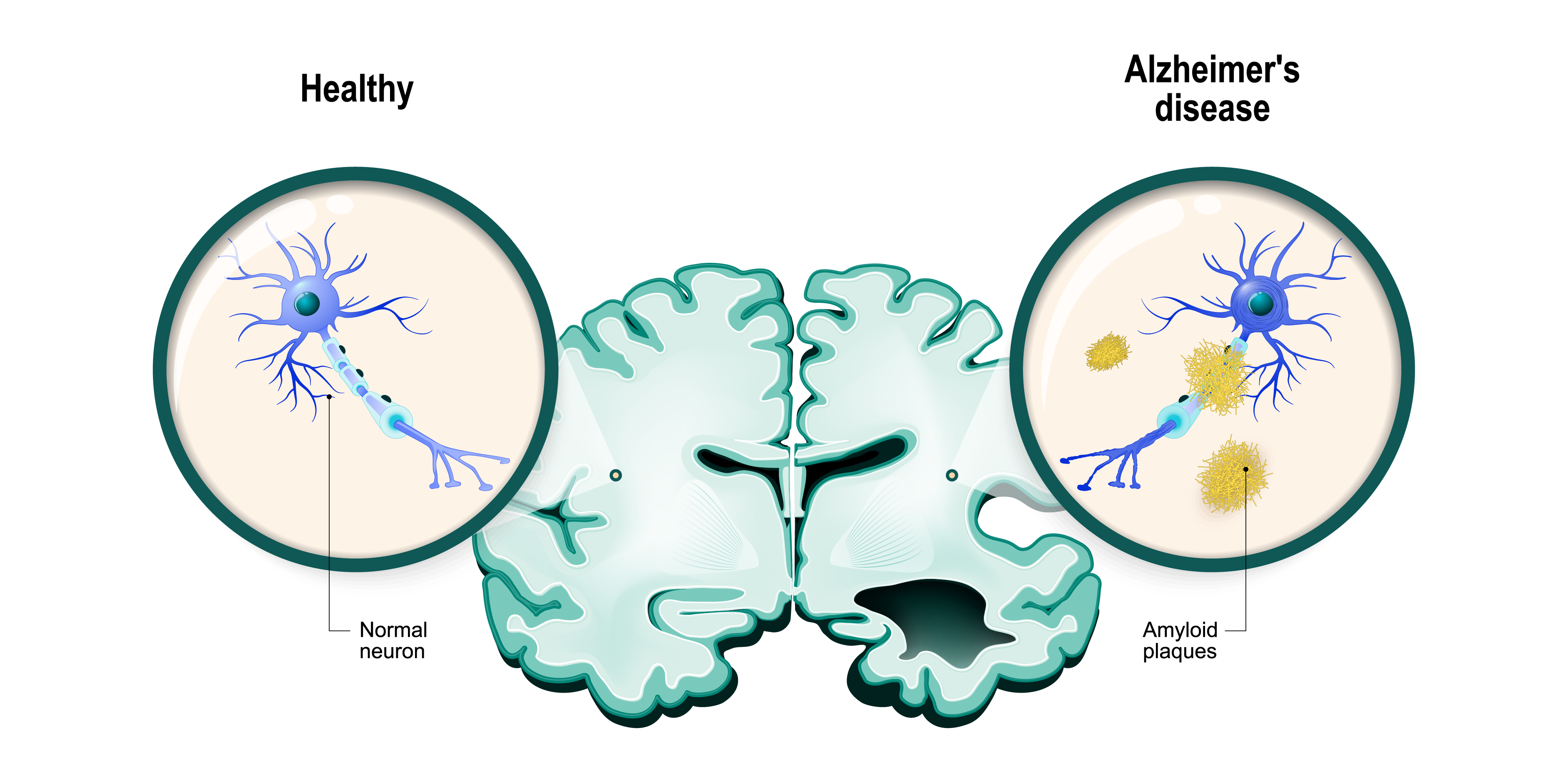
cerebrovascular disease. In the case of AD, pathologic features include the
accumulation of amyloid cerebral plaques and neurofibrillary tangles. In AD,
there is an overproduction and/or decreased clearance of amyloid β
peptides. With this, there is noted hyperphosphorylation of the tau protein, a
microtubule-associated protein that aids in microtubule assembly. Next
to AD, DLB is characterized by accumulation of the synaptic protein α-synuclein
into Lewy bodies and neurites in the. Oher factors, such as depletion of
neurotransmitters, loss of neural synapses, mitochondrial dysfunction,
oxidative stress, inflammation ischemia, abnormal insulin signaling, and
cholesterol metabolism also play a role in the pathophysiology of dementia.
Etiology
Potentially reversible causes of dementia include:
- Infections (eg meningitis, encephalitis)
- Toxic or metabolic encephalopathies (eg hypothyroidism, vitamin B12 deficiency, alcohol-related syndromes)
- Inflammatory disorders (eg autoimmune encephalopathy)
- Intracranial neoplasms
- Hydrocephalus (obstructive or normal-pressure hydrocephalus)
- Delirium
- Epilepsy
- Depression and other psychiatric conditions
- Drugs that increase anticholinergic burden
- Traumatic brain injury
- Sensory impairment (eg hearing or vision loss)
Irreversible causes of dementia include:
- Degenerative diseases (eg AD, Parkinson’s disease, frontotemporal dementia, DLB)
- Cerebrovascular disease (eg stroke, small-vessel disease)
- Genetic disorders (eg Down syndrome)
Risk Factors
Dementia is multifactorial, caused by a combination of
genetic and environmental factors. These factors can be classified into
modifiable and nonmodifiable risk factors.
Nonmodifiable risk factors include:
- Advanced age: Age ≥65 years is a risk factor for any dementia
- Sex: Females have a greater risk of dementia, especially AD
-
Genetic:
- Early-onset AD: Caused by an autosomal dominant mutation in three identified genes; the amyloid β-protein precursor on chromosome 21, presenilin 1 on chromosome 14, and presenilin 2 on chromosome 1
- Late-onset (>65 years): Multifactorial but involves a strong genetic predisposition that is complex and heterogeneous
- Apolipoprotein gene: The presence of the ε4 variant contributes to the development of both late-onset and sporadic early-onset AD
Modifiable risk factors include:
- Cardiovascular: Hypertension, diabetes mellitus (DM), obesity, and smoking
- Psychiatric illness: Late-life depression is associated with a two-fold increase of dementia
- Lifestyle: Excessive alcohol consumption, physical inactivity and impaired social relationships
Classification
Alzheimer's Disease (AD)
AD is the most common cause of dementia. The majority of patients are 65
years or older, while familial types, which are rarer, are seen in patients
younger than 65 years of age. In AD, the most common early symptom is
short-term memory loss, followed by cognitive impairment in other spheres
several years after. After memory loss, there is loss of executive function, language
dysfunction, personality and behavioral changes, difficulties with activities
of daily living (ADL), and loss of visuo-spatial function are experienced.
Neuropsychiatric symptoms such as depression, irritability, anxiety, apathy,
agitation and aggression are common. Seizures and myoclonus usually manifest
late in the disease.
Vascular Dementia
Reported to be the second most common cause of dementia, it is a type of dementia
caused by the effects of cerebrovascular disease on cognitive functioning.
Vascular dementia may either present abruptly or in a stepwise progression. Patients
would have a history of stroke or associated focal neurological signs and
symptoms. The hallmark of the disease is the prominent impairment of executive functions
which may also be accompanied by apraxia, progressive decline in gait,
attention, and planning. Cognitive deficits will depend on what part of the
brain is affected by vascular lesions. Vascular dementia frequently coexists
with AD, known as mixed dementia, that is characterized by gradual progressive
dementia occurring in the setting of a known cerebrovascular disease.
Young-onset vascular dementia may have a genetic origin.
Dementia with Lewy Bodies (DLB)
DLB is characterized by dementia, parkinsonian features (eg
bradykinesia, rigidity, and/or postural instability), fluctuating cognition,
prominent and recurrent visual hallucinations. DLB is noted to have a more
rapid evolution of symptoms than AD. Compared to those with AD, patients with
DLB have more problems in executive functions such as planning, prioritizing
and sequencing, and visuospatial function impairment. However, DLB patients
perform better with verbal memory than AD patients. Supportive features of DLB
include neuroleptic sensitivity, repeated falls, and syncope or episodes of
transient loss of consciousness. The onset of cognitive symptoms in relation to
motor slowing is usually ≤1 year. It is important to recognize DLB from life-threatening
reactions, specifically extrapyramidal side effects, of antipsychotic
medications.
Parkinson’s Disease Dementia (PDD)
In patients with Parkinson’s disease, as much as ¾ of the patients develop
dementia 10 years after. PDD is characterized by cognitive and motor slowing,
memory impairment, and executive dysfunction. It must be noted that it is
difficult to differentiate DLB and PDD clinically from each other. However, in
DLB, the onset of dementia and parkinsonism occurs within a year, whereas motoric
dysfunction occurs years (10-15 years) before onset of dementia.
*Please see Parkinson’s Disease & Parkinson’s Disease Dementia
disease management chart for further
information.
Frontotemporal Dementia (FTD)
FTD, also known as frontotemporal lobar degeneration, occurs in patients aged
50-60 years old. People with FTD present a significant portion of people with
dementia under the age of 65. In the early stages of the disease, patients
present with changes in personality, accompanied by deterioration of social
skills, emotional blunting, early language disturbance, executive dysfunction,
and significant apathy. Patients with FTD present with progressive decline in
interpersonal skills, loss of emotional responsivity, and with emergence of
abnormal behaviors such as disinhibition, obsessions, rituals, stereotypies,
and alterations in feeding and other appetitive functions. Memory difficulties,
apraxia, and other features of dementia would usually follow later as FTD
progresses. Brain computed tomography (CT) or magnetic resonance imaging (MRI)
will show frontal love or anterior temporal atrophy. While single-photon
emission computed tomography (SPECT) or positron emission tomography (PET) will
show frontal hypoperfusion or hypometabolism. The course of FTD is progressive
and more rapid than in AD.
Other Progressive Dementing Disorders
Huntington’s Disease
Huntington’s disease is an autosomal dominant disease that primarily
affects the basal ganglia and other subcortical structures. The disease
manifests with motor (eg chorea), mood, behavioral, and cognitive symptoms.
Creutzfeld-Jakob Disease (CJD)
The disease is characterized by rapidly progressive encephalopathy, rapid
cognitive decline, and death within 1.5 years.