White film-coated round biconvex tablets, scored with a wide pressure-sensitive division mark on one side and debossed with 'M9MN' and '10' on the other side.
Each film coated tablet contains 10 mg of Memantine hydrochloride.
Excipients/Inactive Ingredients: Lactose monohydrate, microcrystalline cellulose, talc, colloidal anhydrous silica, magnesium stearate, hypromellose, titanium dioxide, PEG 4000.
Pharmacotherapeutic group: Anti-dementia drugs. ATC code: N06DX01.
Pharmacology: Pharmacodynamics: There is increasing evidence that malfunctioning of glutamatergic neurotransmission, in particular at NMDA-receptors, contributes to both expression of symptoms and disease progression in neurodegenerative dementia.
Memantine is a voltage-dependent, moderate-affinity uncompetitive NMDA-receptor antagonist. It modulates the effects of pathologically elevated tonic levels of glutamate that may lead to neuronal dysfunction.
Pharmacokinetics: The pharmacokinetics parameters of 16 subjects (16 subjects were included in the study and all 16 subjects completed all 2 study periods) were calculated and results were statistically analyzed to demonstrate bioequivalence in a 2-period, crossover design study. After oral administration of Memantine HCl 10 mg film coated tablets (test product) the mean of the maximum plasma concentration (Cmax) (rate of absorption) was 12.32 ng/mL the mean Tmax 6.31 h. The extent of absorption is expressed in Area Under the Curve (AUC)0-72 and AUC0-inf the mean values were 576.54 ng·h/mL and 891.98 ng·h/mL respectively. The mean elimination half life (T1/2) of Memantine HCl 10 mg film coated tablets was 47.68 h.
The ratios and confidence intervals between test and reference product were as following: for Cmax the ratio was 98.89% (95.52% - 102.39%). For AUC0-72 the ratio was 99.33% (96.36% - 102.38%). The results of the study showed that the ratios and confidence intervals are within the acceptance range for bioequivalence, therefore it can be concluded that the test product, Memantine HCl 10 mg film coated tablets, is bioequivalence with the reference product.
Treatment of patients with moderate to severe Alzheimer's disease.
Treatment should be initiated and supervised by a physician experienced in the diagnosis and treatment of Alzheimer's dementia. Therapy should only be started if a caregiver is available who will regularly monitor drug intake by the patient. Diagnosis should be made according to current guidelines. The tolerance and dosing of Memantine should be reassessed on a regular basis, preferably within three month after start of treatment. Thereafter, the clinical benefit of Memantine and the patients tolerance of treatment should be reassessed on a regular basis according to current clinical guidelines. Maintenance treatment can be continued for as long as a therapeutic benefit is favourable and the patient tolerates treatment with Memantine. Discontinuation of Memantine should be considered when evidence of a therapeutic effect is no longer present or if the patient does not tolerate treatment.
Memantine should be administered once a day and should be taken at the same time every day. The film coated tablets can be taken with or without food.
Adults: Dose titration: The maximum daily dose is 20 mg per day. In order to reduce the risk of undesirable effects, the maintenance dose is achieved by upward titration of 5 mg per week over the first 3 weeks as follows: Week 1 (day 1-7): The patient should take a half a 10 mg film coated tablet (5mg) per day for 7 days.
Week 2 (day 8-14): The patient should take one 10 mg film coated tablet (10 mg) per day for 7 days.
Week 3 (day 15-21): The patient should take one and a half 10 mg film coated tablets (15 mg) per day for 7 days.
From week 4 on: The patient should take two 10 mg film coated tablets (20 mg) per day.
Maintenance dose: The recommended maintenance dose is 20 mg per day.
Elderly: the recommended dose for patients over the age of 65 years is 20 mg per day (two 10 mg film coated tablets once a day) as described previously.
Children and adolescents under the age of 18 years: due to lack of data on safety and efficacy.
Renal impairment: In patients with mildly impaired renal function (creatinine clearance 50-80 ml/min) no dose adjustment is required. In patients with moderate renal impairment (creatinine clearance 3Q-49 ml/min) daily dose should be 10 mg per day. If tolerated well after at least 7 days of treatment, the dose could be increased up to 20 mg/day according to standard titration scheme. In patients with severe renal impairment (creatinine clearance 5-29 ml/min) daily dose should be 10 mg per day.
Hepatic impairment: in patients with mild or moderate hepatic impaired function (Child-Pugh A and Child-Pugh B), no dose adjustment is needed. No data on the use of Memantine in patients with severe hepatic impairment are available. Administration of Memantine is not recommended in patients with severe hepatic impairment.
Symptoms: Relative large overdose (200 mg and 105 mg/day for 3 days, respectively) have been associated with either only symptoms of tiredness, weakness and/or diarrhoea or no symptoms. In the overdose cases below 140 mg or unknown dose the patients revealed symptoms from central nervous system (confusion, drowsiness, somnolence, vertigo, agitation, aggression, hallucination, and gait disturbance) and/or of gastrointestinal origin (vomiting and diarrhoea).
In the most extreme case of overdose, the patients survived the oral intake of a total of 2000 mg Memantine with effects on the central nervous system (coma for 10 days, and later diplopia and agitation). The patients received symptomatic treatment and plasmapheresis. The patients recovered without permanent sequelae.
In another case of a large overdose, the patients also survived and recovered.
The patient had received 400 mg Memantine orally. The patient experienced central nervous system symptoms such as restlessness, psychosis, visual hallucinations, proconvulsiveness, somnolence, stupor, and unconsciousness.
Treatment: In the event of overdose, treatment should be symptomatic.
No specific antidote for intoxication or overdose is available. Standard clinical procedures to remove active substance material, e.g. gastric lavage, carbo medicinalis (interruption of potential entero-hepatic recirculation), acidification of urine, forced diuresis should be used as appropriate. In case of signs and symptoms of general central nervous system (CNS) overstimulation, careful symptomatic clinical treatment should be considered.
Hypersensitivity to the active substance or to any of the excipients. Concomitant use of medication that contains the N-methyl-D-aspartate (NMDA)-antagonist dextromethorphan, which is an ingredient of many anti-tussive preparations.
Caution is recommended with patients suffering from epilepsy.
Concomitant use of N-methyl-D-aspartate (NMDA)-antagonist such as amantadine, ketamine or dextromethorphan should be avoided. These compounds act at the same receptor system as Memantine, and therefore adverse drug reactions (mainly CNS-related) may be more frequent or more pronounced (see also Interactions).
Some factors that may raise urine pH may necessitate careful monitoring of the patient. These factors include drastic changes in diet, e.g. from a carnivore to a vegetarian diet, or a massive ingestion of alkalising gastric buffers. Also, urine pH may be elevated by states of renal tubulary acidosis (RTA) or severe infections of the urinary tract with Proteus bacteria.
Patients with recent myocardial infarction, uncompensated congestive heart failure (NYHA III-IV), and uncontrolled hypertension should be closely supervised.
The safety of concomitant administration of Memantine and neuroleptics, benzodiazepines and antidepressant must be considered.
Effects on ability to drive and use machines: Moderate to severe Alzheimer's disease usually causes impairment of driving performance and compromises the ability to use machinery. Furthermore, Memantine has minor to moderate influence on the ability to drive and use machines such that outpatients should be warned to take special care.
Pregnancy: For Memantine, no clinical data on exposed pregnancies are available. Animal studies indicate a potential for reducing intrauterine growth at exposure levels which are identical or slightly higher than at human exposure. The potential risk for human is unknown. Memantine should not be used during pregnancy unless clearly necessary.
Lactation: It is not known whether Memantine is excreted in humans breast milk but, taking into consideration the lipophilicity of the substance, this probably occurs. Women taking Memantine should not breast-feed.
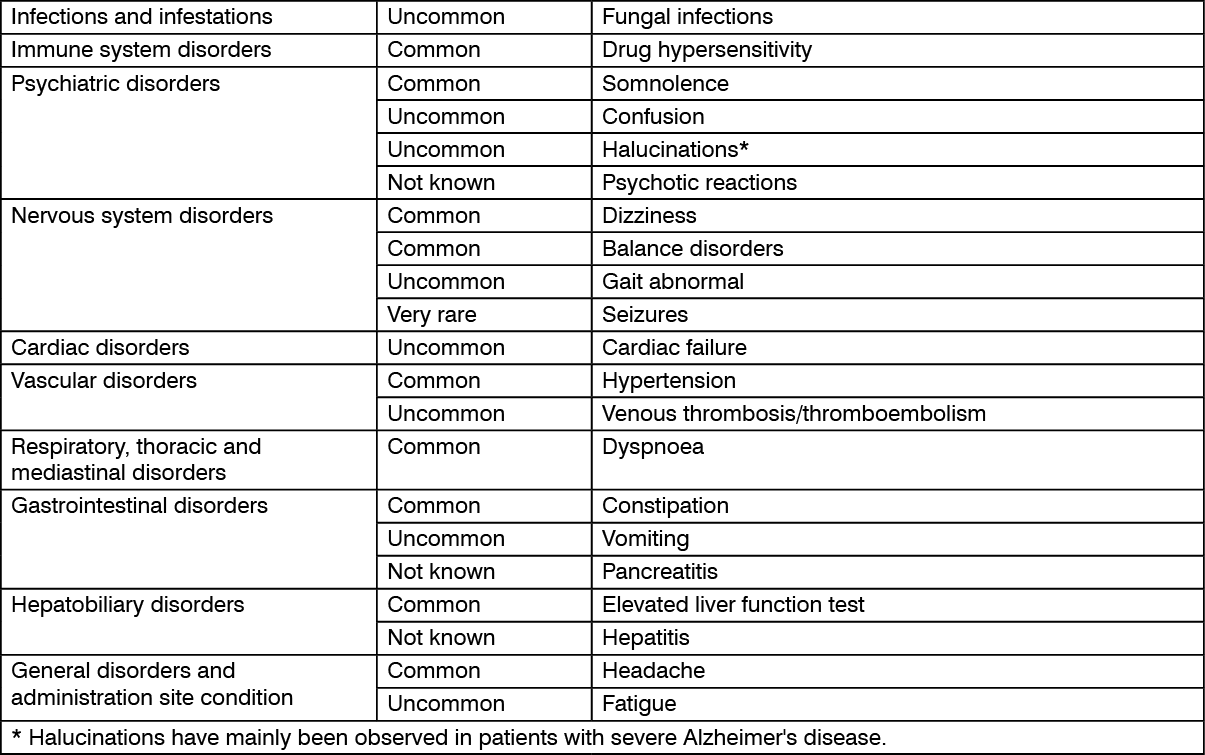
Adverse reactions are ranked according to system organ class, using the following convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Alzheimer's disease has been associated with depression, suicidal ideation and suicide.
Due to the pharmacological effects and the mechanism of action of Memantine the following interactions may occur: The mode of action suggests that the effects of L-dopa, dopaminergic agonist, and anticholinergics may be enhanced by concomitant treatment with NMDA-antagonists such as Memantine. The effects of barbiturates and neuroleptics may be reduced. Concomitant administration of Memantine with the antispasmodic agents, dantrolene or baclofen, can modify their effects and a dosage adjustment may be necessary.
Concomitant use of Memantine and amantadine should be avoided, owing to the risk of pharmacotoxic psychosis. Both compounds are chemically related NMDA-antagonists. The same may be true for ketamine and dextromethorphan (see also Precautions). There is one published case report on a possible risk also for the combination of Memantine and phenytoin.
Other active substances such as cimetidine, ranitidine, procainamide, quinidine, quinine and nicotine that use the same renal cationic transport system as amantadine may also possibly interact with Memantine leading to a potential risk of increased plasma levels.
There may be a possibility of reduced serum level of hydrochlorothiazide (HCT) when Memantine is co-administered with HCT or any combination with HCT.
Isolated cases with international normalized ratio (INR) increases have been reported in patients concomitantly treated with warfarin.
Although no causal relationship has been established, close monitoring of prothrombin time or INR is advisable for patients concomitantly treated with oral anticoagulants.
In single-dose pharmacokinetic (PK) studies in young healthy subjects, no relevant active substance - active substance interaction of Memantine with glyburide/metformin or donepezil was observed.
In a clinical study in young healthy subjects no relevant effect of Memantine on the pharmacokinetics of galantamine was observed.
Memantine did not inhibit CYP 1A2, 2A6, 2C9, 2D6, 2E1, 3A, flavin containing monoxygenase, epoxide hydrolase and sulphation in vitro.
Incompatibilities: Not applicable.
Store below 30°C.
Shelf Life: 2 years.
N06DX01 - memantine ; Belongs to the class of other anti-dementia drugs.
Cimantin FC tab 10 mg
2 × 14's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out