


 Sign Out
Sign Out
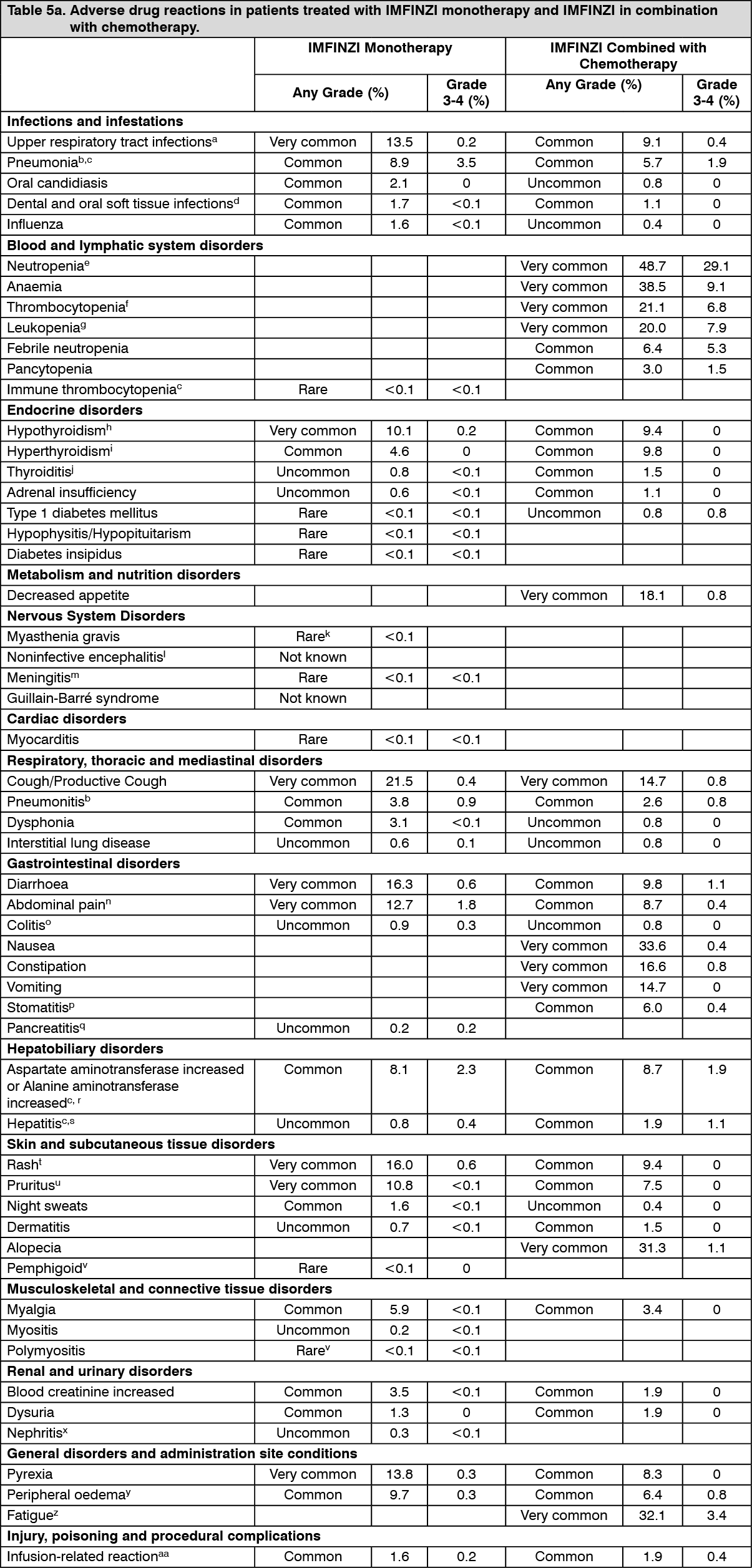
The safety of IMFINZI given in combination with chemotherapy is based on data in 265 patients with SCLC. IMFINZI was administered at a dose of 1500 mg every 3 weeks in combination with chemotherapy followed by monotherapy every 4 weeks. The most frequent (>20%) adverse reactions were neutropenia (48.7%), anaemia (38.5%), nausea (33.6%), fatigue (32.1%), alopecia (31.3%), thrombocytopenia (21.1%), and leukopenia (20.0%).
Tabulated list of adverse reactions: Table 5 lists the incidence of adverse reactions in the monotherapy safety dataset and in patients treated with IMFINZI in combination with chemotherapy in the CASPIAN study. Adverse drug reactions are listed according to system organ class in MedDRA. Within each system organ class, the adverse drug reactions are presented in decreasing frequency. The corresponding frequency category for each ADR is defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1000); very rare (<1/10,000); not known (cannot be estimated from available data). Within each frequency grouping, adverse drug reactions are presented in order of decreasing seriousness. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image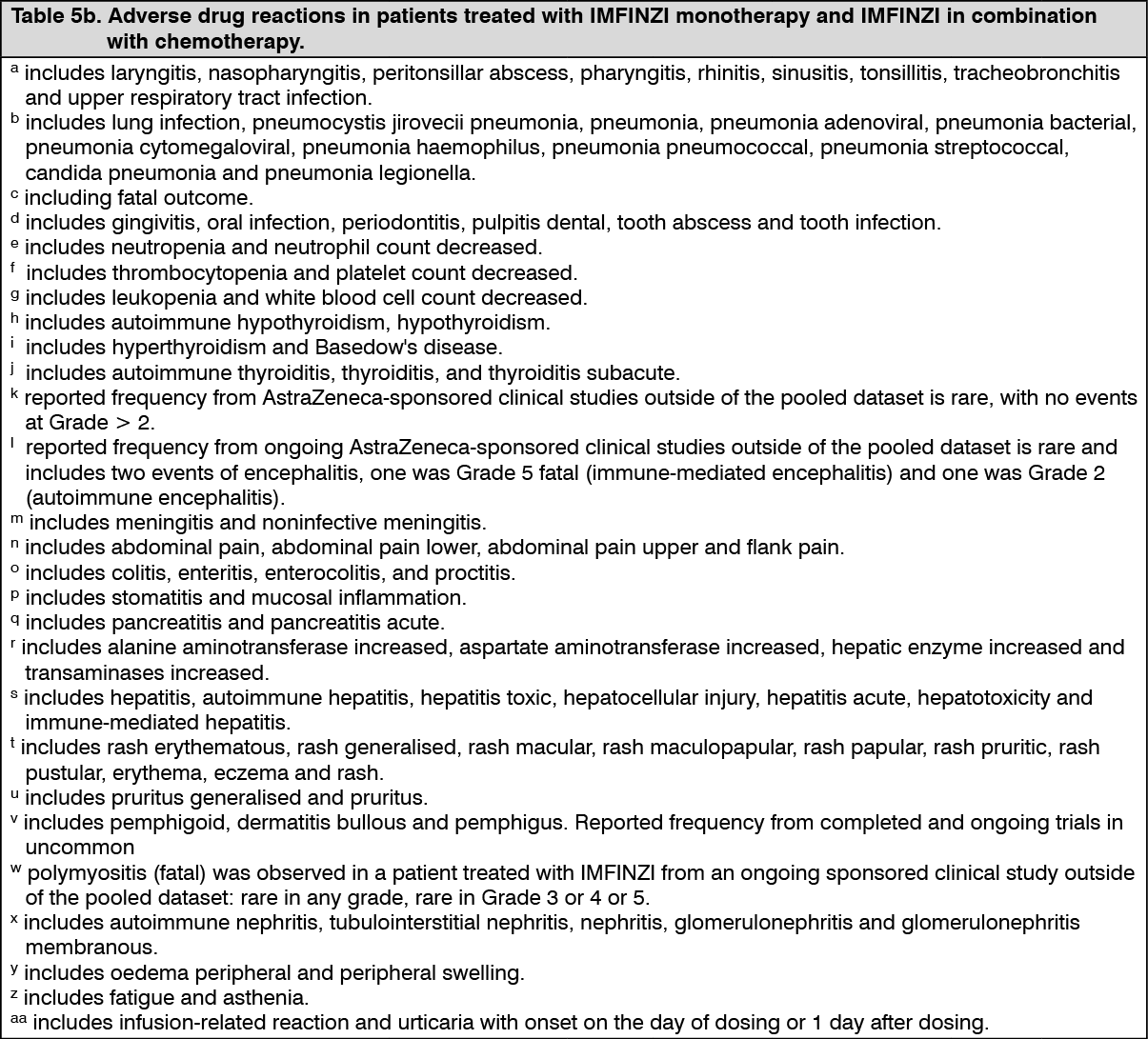 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: IMFINZI is most commonly associated with immune-mediated adverse reactions. Most of these, including severe reactions, resolved following initiation of appropriate medical therapy or withdrawal and/or treatment modifications. The data for the following immune-mediated adverse reactions reflect the combined safety database of 3006 patients which includes the PACIFIC Study and additional studies in patients with various solid tumours, in indications for which durvalumab is not approved. Across all studies, IMFINZI was administered at a dose of 10 mg/kg every 2 weeks, 20 mg/kg every 4 weeks, or 1500 mg every 3 or 4 weeks. Details for the significant adverse reactions for IMFINZI when given in combination with chemotherapy are presented if clinically relevant differences were noted in comparison to IMFINZI monotherapy. The management guidelines for these adverse reactions are described in Dosage & Administration and Precautions.
Immune-mediated pneumonitis: In the combined safety database with IMFINZI monotherapy, (n=3006 multiple tumour types), immune-mediated pneumonitis occurred in 92 (3.1%) patients, including Grade 3 in 25 (0.8%) patients, Grade 4 in 2 (<0.1%) patient, and Grade 5 in 6 (0.2%) patients. The median time to onset was 55 days (range: 2-785 days). Sixty-nine of the 92 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day), and 2 patients also received infliximab and 1 patient also received cyclosporine. IMFINZI was discontinued in 38 patients. Resolution occurred in 53 patients.
Immune-mediated pneumonitis occurred more frequently in the PACIFIC study who had completed treatment with concurrent chemoradiation within 1 to 42 days prior to initiation of the study (9.9%), than in the other patients in the combined safety database (1.8%).
In the PACIFIC Study, (n=475 in the IMFINZI arm, and n=234 in the placebo arm) immune-mediated pneumonitis occurred in 47 (9.9%) patients in the IMFINZI-treated group and 14 (6.0%) patients in the placebo group, including Grade 3 in 9 (1.9%) patients on IMFINZI vs. 6 (2.6%) patients on placebo and Grade 5 (fatal) in 4 (0.8%) patients on IMFINZI vs. 3 (1.3%) patients on placebo. The median time to onset in the IMFINZI-treated group was 46 days (range: 2-342 days) vs. 57 days (range: 26-253 days) in the placebo group. In the IMFINZI-treated group, all patients received systemic corticosteroids, including 30 patients who received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day), and 2 patients also received infliximab. In the placebo group, all patients received systemic corticosteroids, including 12 patients who received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day) and 1 patient also received cyclophosphamide and tacrolimus. Resolution occurred for 29 patients in the IMFINZI treated group vs. 6 in placebo.
Immune-mediated hepatitis: In the combined safety database with IMFINZI monotherapy, immune-mediated hepatitis occurred in 68 (2.3%) patients, including Grade 3 in 35 (1.2%) patient, Grade 4 in 6 (<0.2%) and Grade 5 (fatal) in 4 (<0.1%) patient. The median time to onset was 33 days (range: 3-333 days). Forty-five of the 68 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Three patient also received mycophenolate treatment. IMFINZI was discontinued in 9 patients. Resolution occurred in 31 patients.
Immune-mediated colitis: In the combined safety database with IMFINZI monotherapy, immune-mediated colitis or diarrhoea occurred in 58 (1.9%) patients, including Grade 3 in 9 (0.3%) patients and Grade 4 in 2 (<0.1%) patient. The median time to onset was 70 days (range: 1-394 days). Thirty-eight of the 58 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). One patient also received infliximab treatment and 1 patient also received mycophenolate. IMFINZI was discontinued in 9 patients. Resolution occurred in 43 patients.
Immune-mediated endocrinopathies: Immune-mediated hypothyroidism: In the combined safety database with IMFINZI monotherapy, immune-mediated hypothyroidism occurred in 245 (8.2%) patients, including Grade 3 in 4 (0.1%) patients. The median time to onset was 85 days (range: 1-562 days). Of the 245 patients, 240 patients received hormone replacement therapy and 6 patients received high-dose corticosteroids (at least 40 mg prednisone or equivalent per day) for immune-mediated hypothyroidism. No patients discontinued IMFINZI due to immune-mediated hypothyroidism.
Immune-mediated hyperthyroidism: In the combined safety database with IMFINZI monotherapy, immune-mediated hyperthyroidism occurred in 50 (1.7%) patients, there were no Grade 3 or 4 cases. The median time to onset was 43 days (range: 1-196 days). Forty-six of the 50 patients received medical therapy (thiamazole, carbimazole, propylthiouracil, perchlorate, calcium channel blocker, or beta-blocker), 11 patients received systemic corticosteroids and 4 of the 11 patients received high-dose systemic corticosteroid treatment (at least 40 mg prednisone or equivalent per day). One patient discontinued IMFINZI due to immune-mediated hyperthyroidism. Resolution occurred in 39 patients. Twenty patients experienced hypothyroidism following hyperthyroidism.
Immune-mediated thyroiditis: In the combined safety database with IMFINZI monotherapy, immune-mediated thyroiditis occurred in 12 (0.4%) patients, including Grade 3 in 2 (<0.1%) patients. The median time to onset was 49 days (range: 14-106 days). Of the 12 patients, 10 patients received hormone replacement therapy and 1 patient received high-dose corticosteroids (at least 40 mg prednisone or equivalent per day). One patient discontinued IMFINZI due to immune-mediated thyroiditis. Three patients experienced hypothyroidism following thyroiditis.
Immune-mediated adrenal insufficiency: In the combined safety database with IMFINZI monotherapy, immune-mediated adrenal insufficiency occurred in 14 (0.5%) patients, including Grade 3 in 3 (<0.1%) patients. The median time to onset was 146 days (range: 20-547 days). All 14 patients received systemic corticosteroids; 4 of the 14 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). No patients discontinued IMFINZI due to immune-mediated adrenal insufficiency. Resolution occurred in 3 patients.
Immune-mediated type 1 diabetes mellitus: In one study with 475 locally advance, unresectable NSCLC patients, Grade-3 immune-mediated type 1 diabetes mellitus occurred in 1 (<0.1%) patient. The time to onset was 43 days. This patient recovered with sequelae, required long-term insulin therapy and IMFINZI was permanently discontinued due to immune-mediated type 1 diabetes mellitus.
Immune-mediated hypophysitis/hypopituitarism: In the combined safety database with IMFINZI monotherapy, immune-mediated hypophysitis/hypopituitarism occurred in 2 (<0.1%) patients, both Grade 3. The time to onset for the events was 44 days and 50 days. Both patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day) and one patient discontinued IMFINZI due to immune-mediated hypophysitis/hypopituitarism.
Immune-mediated nephritis: In the combined safety database with IMFINZI monotherapy, immune-mediated nephritis occurred in 14 (0.5%) patients, including Grade 3 in 2 (<0.1%) patients. The median time to onset was 71 days (range: 4-393 days). Nine patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day) and 1 patient also received mycophenolate. IMFINZI was discontinued in 5 patients. Resolution occurred in 8 patients.
Immune-mediated rash: In the combined safety database with IMFINZI monotherapy, immune-mediated rash or dermatitis occurred in 50 (1.7%) patients, including Grade 3 in 12 (0.4%) patients. The median time to onset was 43 days (range: 4-333 days). Twenty-three of the 50 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). IMFINZI was discontinued in 3 patients. Resolution occurred in 32 patients.
Infusion-related reactions: In the combined safety database with IMFINZI monotherapy, infusion-related reactions occurred in 49 (1.6%) patients, including Grade 3 in 5 (0.2%) patients. There were no Grade 4 or 5 events.
Laboratory abnormalities: In patients treated with durvalumab monotherapy, the proportion of patients who experienced a shift from baseline to a Grade 3 or 4 laboratory abnormality was as follows: 2.4% for alanine aminotransferase increased, 3.6% for aspartate aminotransferase increased, 0.5% for blood creatinine increased, 5.7% for amylase increased and 5.6% for lipase increased. The proportion of patients who experienced a TSH shift from baseline that was ≤ULN to any grade >ULN was 18.8% and a TSH shift from baseline was ≥LLN to any grade <LLN was 18.1%.
In patients treated with durvalumab in combination with chemotherapy, the proportion of patients who experienced a shift from baseline to a Grade 3 or 4 laboratory abnormality was as follows: 4.9% for alanine aminotransferase increased, 4.6% for aspartate aminotransferase increased, 3.4% for blood creatinine increased, 4.8% for amylase increased and 8.1% for lipase increased. The proportion of patients who experienced a TSH shift from baseline that was ≤ULN to any grade >ULN was 17.7% and a TSH shift from baseline that was ≥LLN to any grade <LLN was 31.3%.
Immunogenicity: Immunogenicity of IMFINZI as monotherapy is based on pooled data in 2280 patients who were treated with IMFINZI 10 mg/kg every 2 weeks, or 20 mg/kg every 4 weeks as a single-agent and evaluable for the presence of anti-drug antibodies (ADA). Sixty nine patients (3.0%) tested positive for treatment emergent ADA. Neutralising antibodies (nAb) against durvalumab were detected in 0.5% (12/2280) of patients. The presence of ADA did not have a clinically relevant effect on safety. There are insufficient number of patients to determine ADA impact on efficacy. Based on population PK analysis, slightly lower exposure are expected in ADA-positive patients however, the reduction of PK exposure is less than 30% compared to a typical patient and is not considered clinically relevant.
In the CASPIAN study, of 201 patients who were treated with IMFINZI 1500 mg every 3 weeks in combination with chemotherapy and evaluable for the presence of ADAs, 0 (0%) patients tested positive for treatment-emergent ADAs. The impact of treatment-emergent ADA on PK, clinical safety and efficacy of durvalumab was not evaluable as no patient samples tested positive for treatment-emergent durvalumab ADA.
Elderly: No overall differences in safety were reported between elderly (≥65 years) and younger patients. Data from NSCLC and ES-SCLC patients 75 years of age or older are limited.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after registration of the medicinal product is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions at e-meso.pom.go.id.
View ADR Monitoring Form