Levocetirizine Dihydrochloride.
Each film coated tablet contains: Levocetirizine Dihydrochloride 5 mg.
Pharmacology: Pharmacodynamics: Levocetirizine the (R) enantiomer of cetirizine, is a potent and selective antagonist of peripheral H1-receptors. Binding studies revealed that Levocetirizine has high affinity for human H1-receptors (Ki=3.2 nmol L). Levocetirizine dissociates from H1-receptors with half-life of 115±38 min. Pharmacodynamic studies in healthy volunteers demonstrate that, at half the dose, Levocetirizine has comparable activity to cetirizine, both in skin and in the nose. In vitro studies (Boyden chambers and cell layers techniques) show that Levocetirizine inhibits eotaxin-induced eosinophil transendothelial migration through both dermal and lung cells. A pharmacodynamic experimental study in vivo (skin chamber technique) showed three main inhibitory effects of Levocetirizine 5 mg in the first 6 hour of pollen-induced reaction, compared with placebo in 14 adult patients: inhibition of VCAM-1 release, modulation of vascular permeability and a decrease in eosinophil recruitment. Pharmacokinetic/pharmacodynamic relationship: 5 mg Levocetirizine provide a similar pattern of inhibition of histamin-induced wheal and flare than 10 mg cetirizine. As for cetirizine, the action on histamin-induced skin reaction was out of phase with the plasma concentrations. ECGs did not show relevant effects of Levocetirizine on QT interval.
Pharmacokinetics: The pharmacokinetics of Levocetirizine are linear with dose- and time-independent with low inter-subject variability. The pharmacokinetic profile is the same when given as the single enantiomer or when given as cetirizine. No chiral inversion occurs during the process of absorption and elimination.
Absorption: Levocetirizine is rapidly and extensively absorbed following oral administration. Peak plasma concentrations are achieved 0.9 hour after dosing. Steady state achieved after two days. Peak concentrations are typically 270 ng/mL and 308 ng/mL following a single and a repeated 5 mg once daily dose, respectively. The extent of absorption is dose-independent and is not altered-by food, but the peak concentration is reduced and delayed.
Distribution: No tissue distribution data are available in humans. Levocetirizine is 90% bound to plasma proteins. The distribution of Levocetirizine is restrictive, as the volume of distribution is 0.4 l/kg.
Biotransformation: The extent of metabolism of Levocetirizine in humans is less than 14% of the dose and therefore differences resulting from genetic polymorphism or concomitant intake of enzyme inhibitors are expected to be negligible. Metabolic pathways include aromatic oxidation, N- and O-dealkylation, and taurine conjugation. Dealkylation pathways are primarily mediated by CYP 3A4 while aromatic oxidation involved multiple and/or unidentified CYP isoforms. Levocetirizine had no effect on the activities of CYP isoenzymes 1A2, 2C9, 2C19, 2D6, 2E1 and 3A4 at concentrations well above peak concentrations achieved following a 5 mg oral dose. Due to its low metabolism and absence of metabolic inhibition potential, the interaction of levocetirizine with other substances, or vice-versa, is unlikely.
Elimination: The plasma half-life in adults is 7.9±1.9 hours. The mean apparent total body clearance is 0.63 mL/min/kg. The major route of excretion of levocetirizine and metabolites is via urine, accounting for a mean of 85.4% of the dose. Excretion via feces accounts for only 12.9% of the dose. Levocetirizine is excreted both by glomerular filtration and active tubular secretion.
Renal Impairment: The apparent body clearance of Levocetirizine is correlated to the creatinine clearance. It is therefore recommended to adjust the dosing intervals of Levocetirizine, based on creatinine clearance in patients with moderate and severe renal impairment. In anuric end stage renal disease subjects, the total body clearance is decreased by approximately 80% when compared to normal subjects. The amount of Levocetirizine removed during a standard 4-hour hemodialysis procedure was <10%.
Symptomatic treatment of allergic rhinitis and chronic idiopathic urticaria.
The film-coated tablet must be taken orally, swallowed whole with liquid and be taken with or without food. It is recommended to take the daily dose in one single intake.
Adults and Children 6 Years and above: The daily recommended dose of is 5 mg (1 film coated tablet). For children aged less than 6 years no adjusted dosage is yet possible.
Elderly: Adjustment of the dose is recommended in elderly patients with moderated to severe renal impairment (see Patients with renal impairment as follows).
Patients with renal impairment: The dosing intervals must be individualised according to renal function. Refer to the table and adjust the dose as indicated. To use this dosing table, an estimate of the patient's creatinine clearance (Cl
cr) in mL/min is needed.
The Cl
cr (mL/min) may be estimated from serum creatinin (mg/dL) determination using the following formula:
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Dosing Adjustment for patients with Impaired Renal Function: (See table.)
Click on icon to see table/diagram/image
Patients with hepatic impairment: No dose adjustment is needed in patients with solely hepatic impairment. In patients with hepatic impairment and renal impairment, adjustment of the dose is recommended (see Patients with renal impairment as previously mentioned).
Duration of use: The duration of use depends on the type, duration and course of the complaints. For hay fever 3-6 weeks, and in case of short-term pollen exposure as little as one week, is generally sufficient. Clinical experience with 5 mg Levocetirizine as a film-coated tablet formulation is currently available for a 6-month treatment period. For chronic urticaria and chronic allergic rhinitis, up to one year's clinical experience is available for the racemate, and up to 18 months in patients with pruritus associated with atopic dermatitis.
Symptoms: Symptoms of overdose may include drowsiness in adults and initially agitation and restlessness, followed by drowsiness in children.
Management of overdose: There is no known specific antidote to Levocetirizine. Should overdose occur, symptomatic or supportive treatment is recommended. Gastric lavage should be considered following short-term ingestion. Levocetirizine is not effectively removed by haemodialysis.
History of hypersensitivity to Levocetirizine or any of the other constituents of the formulation or to any piperazine derivatives. Patients with severe renal impairment at less than 10 mL/min creatinine clearance.
The use of Levocetirizine Dihydrochloride is not recommended in children aged less than 6 years since the currently available film-coated tablets do not yet allow dose adaption.
Precaution is recommended with intake of alcohol (see Interactions). Patients with rare hereditary problems of galactose intolerance, the lapp lactase deficiency or glucose-galactose malabsorption should not take this medicines.
Effects on Ability to Drive and Use Machines: Comparative clinical trials have revealed no evidence that Levocetirizine at the recommended dose impairs mental alertness, reactivity or the ability to drive. Nevertheless, some patients could experience somnolence, fatigue and asthenia under therapy with Levocetirizine Dihydrochloride. Therefore, patients intending to drive, engage in potentially hazardous activities or operate machinery should take their response to the medicinal product into account.
For Levocetirizine no clinical data on exposed pregnancies are available. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/fetal development, parturition or postnatal development. Caution should be exercised when prescribing to pregnant or lactating woman.
No interaction studies have been performed with Levocetirizine (including no studies with CYP3A4 inducers). Studies with the racemate compound cetirizine demonstrated that there were no clinically relevant adverse interactions (with pseudoephedrine, cimetidine, ketoconazole, erythromycin, azithromycin, glipizide and diazepam). A small decrease in the clearance of cetirizine (16%) was observed in a multiple dose study with theophylline (400 mg once a day); while the disposition of theophylline was not altered by concomitant cetirizine administration. The extent of absorption of Levocetirizine is not reduced with food, although the rate of absorption is decreased. In sensitive patients the simultaneous administration of cetirizine or Levocetirizine and alcohol or other CNS depressants may have effects on the central nervous system, although it has been shown that the racemate cetirizine does not potentiate the effect of alcohol.
R06AE09 - levocetirizine ; Belongs to the class of piperazine derivatives used as systemic antihistamines.
L-Falergi FC tab 5 mg
1 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image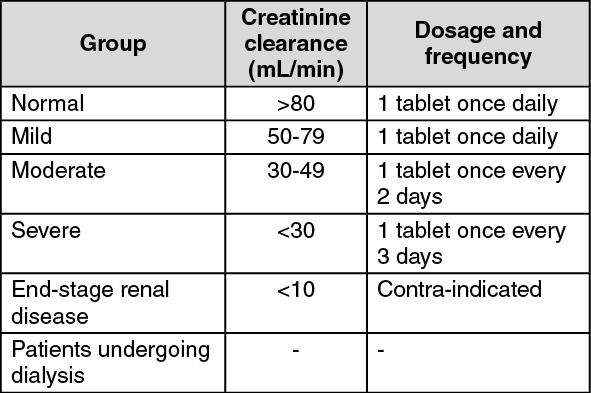 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out