Pharmacology: Pharmacodynamics: Asthma: Salmeterol Multi-center Asthma Research Trial (SMART): The Salmeterol Multi-center Asthma Research Trial (SMART) was a 28-week US study that evaluated the safety of salmeterol compared to placebo added to usual therapy in adult and adolescent subjects. Although there were no significant differences in the primary endpoint of the combined number of respiratory-related deaths and respiratory-related life-threatening experiences, the study showed a significant increase in asthma-related deaths in patients receiving salmeterol (13 deaths out of 13,176 patients treated with salmeterol versus 3 deaths out of 13,179 patients on placebo). The study was not designed to assess the impact of concurrent inhaled corticosteroid use.
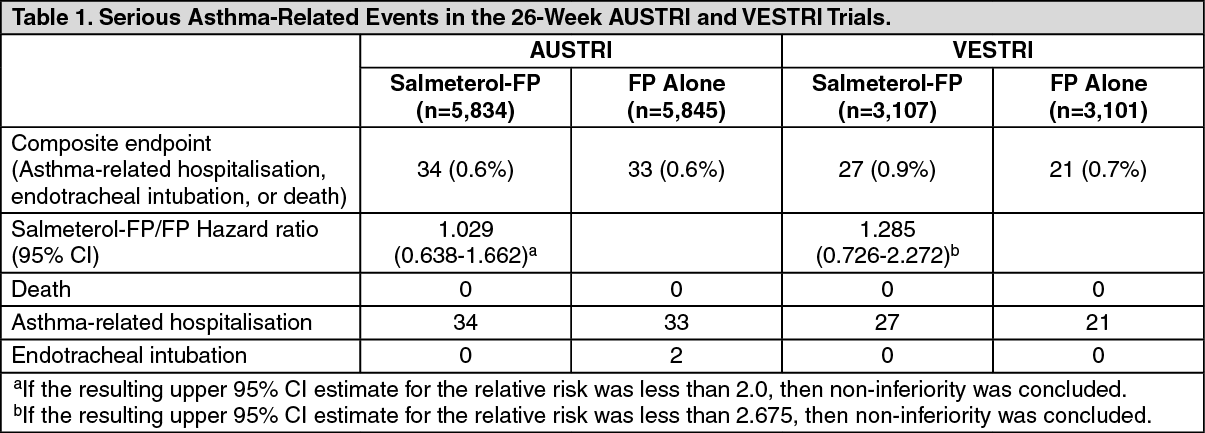
Safety and efficacy of salmeterol-FP versus FP alone in asthma: Two multi-center 26-week studies were conducted to compare the safety and efficacy of salmeterol-FP versus FP alone, one in adult and adolescent subjects (AUSTRI trial), and the other in paediatric subjects 4-11 years of age (VESTRI trial). For both studies, enrolled subjects had moderate to severe persistent asthma with history of asthma-related hospitalisation or asthma exacerbation in the previous year. The primary objective of each study was to determine whether the addition of LABA to ICS therapy (salmeterol-FP) was non-inferior to ICS (FP) alone in terms of the risk of serious asthma-related events (asthma-related hospitalisation, endotracheal intubation, and death). A secondary efficacy objective of these studies was to evaluate whether ICS/LABA (salmeterol-FP) was superior to ICS therapy alone (FP) in terms of severe asthma exacerbation (defined as deterioration of asthma requiring the use of systemic corticosteroids for at least 3 days or an in-patient hospitalisation or emergency department visit due to asthma that required systemic corticosteroids).
A total of 11,679 and 6,208 subjects were randomized and received treatment in the AUSTRI and VESTRI trials, respectively. For the primary safety endpoint, non-inferiority was achieved for both trials (see Table 1 as follows).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For the secondary efficacy endpoint, reduction in time to first asthma exacerbation for salmeterol-FP relative to FP was seen in both studies, however only AUSTRI met statistical significance: See Table 2.
Click on icon to see table/diagram/image
Twelve-month study: A large twelve-month study (Gaining Optimal Asthma ControL, GOAL) in 3,416 asthma patients compared the efficacy and safety of SERETIDE versus inhaled corticosteroid alone in achieving pre-defined levels of asthma control. Treatment was stepped-up every 12 weeks until
##‘Total control’ was achieved or the highest dose of study drug was reached. Control needed to be sustained for at least 7 out of the last 8 weeks of treatment. The study showed that: 71% of patients treated with SERETIDE achieved
#‘Well-controlled’ asthma compared with 59% of patients treated with inhaled corticosteroid alone.
41% of patients treated with SERETIDE achieved
##‘Total control’ of asthma compared with 28% of patients treated with inhaled corticosteroid alone.
These effects were observed earlier with SERETIDE compared with inhaled corticosteroid alone and at a lower inhaled corticosteroid dose.
The GOAL study also showed that: The rate of exacerbations was 29% lower with SERETIDE compared to inhaled corticosteroid treatment alone.
Attaining ‘Well-controlled’ and ‘Totally controlled’ asthma improved Quality of Life (QoL). 61% of patients reported minimal or no impairment on QoL, as measured by an asthma specific quality of life questionnaire, after treatment with SERETIDE compared to 8% at baseline.
#Well-controlled asthma; less than or equal to 2 days with symptom score greater than 1 (symptom score 1 defined as ‘symptoms for one short period during the day’), SABA use on less than or equal to 2 days and less than or equal to 4 occasions/week, greater than or equal to 80% predicted morning peak expiratory flow, no night-time awakenings, no exacerbations and no side effects enforcing a change in therapy.
##Total control of asthma; no symptoms, no SABA use, greater than or equal to 80% predicted morning peak expiratory flow, no night-time awakenings, no exacerbations and no side effects enforcing a change in therapy.
Two further studies have shown improvements in lung function, percentage of symptom free days and reduction in rescue medication use, at 60% lower inhaled corticosteroid dose with SERETIDE compared to treatment with inhaled corticosteroid alone, whilst the control of the underlying airway inflammation, measured by bronchial biopsy and bronchoalveolar lavage, was maintained.
Additional studies have shown that treatment with SERETIDE significantly improves asthma symptoms, lung function and reduces the use of rescue medication compared to treatment with the individual components alone and placebo. Results from GOAL show that the improvements seen with SERETIDE, in these endpoints, are maintained over at least 12 months.
COPD: Symptomatic COPD patients without restriction to 10% reversibility to a short-acting beta
2-agonist: Placebo-controlled clinical trials, over 6 months, have shown that regular use of both SERETIDE 50/250 and 50/500 micrograms rapidly and significantly improves lung function, significantly reduced breathlessness and the use of relief medication. There were also significant improvements in health status.
Symptomatic COPD patients who demonstrated less than 10% reversibility to a short-acting beta
2-agonist: Placebo-controlled clinical trials, over 6 and 12 months, have shown that regular use of SERETIDE 50/500 micrograms rapidly and significantly improves lung function, significantly reduced breathlessness and the use of relief medication. Over a 12-month period the risk of COPD exacerbations and the need for additional courses of oral corticosteroids was significantly reduced from 1.42 per year to 0.99 per year compared with placebo and the risk of exacerbations requiring oral corticosteroids was significantly reduced from 0.81 to 0.47 per year compared with placebo. There were also significant improvements in health status.
Fluticasone propionate containing medications in asthma during pregnancy: An observational retrospective epidemiological cohort study utilising electronic health records from the United Kingdom was conducted to evaluate the risk of MCMs following first trimester exposure to inhaled FP alone and SERETIDE relative to non-FP containing ICS. No placebo comparator was included in this study.
Within the asthma cohort of 5,362 first trimester ICS-exposed pregnancies, 131 diagnosed MCMs were identified; 1,612 (30%) were exposed to FP or SERETIDE of which 42 diagnosed MCMs were identified. The adjusted odds ratio for MCMs diagnosed by 1 year was 1.1 (95% CI: 0.5 – 2.3) for FP exposed vs non-FP ICS exposed women with moderate asthma and 1.2 (95% CI: 0.7 – 2.0) for women with considerable to severe asthma. No difference in the risk of MCMs was identified following first trimester exposure to FP alone versus SERETIDE. Absolute risks of MCM across the asthma severity strata ranged from 2.0 to 2.9 per 100 FP-exposed pregnancies which is comparable to results from a study of 15,840 pregnancies unexposed to asthma therapies in the General Practice Research Database (2.8 MCM events per 100 pregnancies).
Mechanism of action: SERETIDE contains salmeterol and fluticasone propionate which have differing modes of action. Salmeterol protects against symptoms, fluticasone propionate improves lung function and prevents exacerbations of the condition. SERETIDE can offer a more convenient regime for patients on concurrent beta-agonist and inhaled corticosteroid therapy. The respective mechanisms of action of both drugs are discussed as follows: Salmeterol: Salmeterol is a selective long-acting (12 hours) beta
2-adrenoceptor agonist with a long side chain which binds to the exo-site of the receptor.
These pharmacological properties of salmeterol offer more effective protection against histamine-induced bronchoconstriction and produce a longer duration of bronchodilation, lasting for at least 12 hours, than recommended doses of conventional short-acting beta
2-agonists.
In vitro tests have shown salmeterol is a potent and long-lasting inhibitor of the release, from human lung, of mast cell mediators such as histamine, leukotrienes and prostaglandin D
2.
In man, salmeterol inhibits the early and late phase response to inhaled allergen; the latter persisting for over 30 hours after a single dose when the bronchodilator effect is no longer evident.
Fluticasone propionate: Fluticasone propionate given by inhalation at recommended doses has a potent glucocorticoid antiinflammatory action within the lungs, resulting in reduced symptoms and exacerbations of asthma, without the adverse effects observed when corticosteroids are administered systemically.
Daily output of adrenocortical hormones usually remains within the normal range during chronic treatment with inhaled fluticasone propionate, even at the highest recommended doses in children and adults. After transfer from other inhaled steroids, the daily output gradually improves despite past and present intermittent use of oral steroids, thus demonstrating return of normal adrenal function on inhaled fluticasone propionate. The adrenal reserve also remains normal during chronic treatment, as measured by a normal increment on a stimulation test. However, any residual impairment of adrenal reserve from previous treatment may persist for a considerable time and should be borne in mind (see Precautions).
Pharmacokinetics: There is no evidence in animal or human subjects that the administration of salmeterol and fluticasone propionate together by the inhaled route affects the pharmacokinetics of either component.
For pharmacokinetic purposes therefore, each component can be considered separately.
In a placebo-controlled, crossover drug interaction study in 15 healthy subjects, co-administration of salmeterol (50 mcg twice daily inhaled) and the CYP3A4 inhibitor ketoconazole (400 mg once daily orally) for 7 days resulted in a significant increase in plasma salmeterol exposure (1.4-fold C
max and 15-fold AUC). There was no increase in salmeterol accumulation with repeat dosing. Three subjects were withdrawn from salmeterol and ketoconazole co-administration due to QTc prolongation or palpitations with sinus tachycardia. In the remaining 12 subjects, co-administration of salmeterol and ketoconazole did not result in a clinically significant effect on heart rate, blood potassium or QTc duration (see Precautions, and Interactions).
Salmeterol: Salmeterol acts locally in the lung therefore plasma levels are not an indication of therapeutic effects. In addition, there are only limited data available on the pharmacokinetics of salmeterol because of the technical difficulty of assaying the drug in plasma due to the low plasma concentrations at therapeutic doses (approximately 200 picograms/mL or less) achieved after inhaled dosing. After regular dosing with salmeterol xinafoate, hydroxynaphthoic acid can be detected in the systemic circulation, reaching steady state concentrations of approximately 100 nanograms/mL. These concentrations are up to 1,000-fold lower than steady state levels observed in toxicity studies. No detrimental effects have been seen following long-term regular dosing (more than 12 months) in patients with airway obstruction.
An
in vitro study showed that salmeterol is extensively metabolised to α-hydroxysalmeterol (aliphatic oxidation) by cytochrome P450 3A4 (CYP3A4). A repeat dose study with salmeterol and erythromycin in healthy volunteers showed no clinically significant changes in pharmacodynamic effects at 500 mg three times daily doses of erythromycin. However, a salmeterol-ketoconazole interaction study resulted in a significant increase in plasma salmeterol exposure (see Precautions, and Interactions).
Fluticasone propionate: The absolute bioavailability of fluticasone propionate for each of the available inhaler devices has been estimated from within and between study comparisons of inhaled and intravenous pharmacokinetic data. In healthy adult subjects the absolute bioavailability has been estimated for fluticasone propionate Diskus (7.8%), fluticasone propionate Diskhaler (9.0%), fluticasone propionate Inhaler (10.9%), salmeterol-fluticasone propionate Inhaler (5.3%) and salmeterol-fluticasone propionate Diskus (5.5%) respectively. In patients with asthma or COPD a lesser degree of systemic exposure to inhaled fluticasone propionate has been observed. Systemic absorption occurs mainly through the lungs and is initially rapid then prolonged. The remainder of the inhaled dose may be swallowed but contributes minimally to systemic exposure due to the low aqueous solubility and pre-systemic metabolism, resulting in oral availability of less than 1%. There is a linear increase in systemic exposure with increasing inhaled dose. The disposition of fluticasone propionate is characterised by high plasma clearance (1,150 mL/min), a large volume of distribution at steady-state (approximately 300 L) and a terminal half-life of approximately 8 hours. Plasma protein binding is moderately high (91%). Fluticasone propionate is cleared very rapidly from the systemic circulation, principally by metabolism to an inactive carboxylic acid metabolite, by the cytochrome P450 enzyme CYP3A4.
The renal clearance of fluticasone propionate is negligible (<0.2%) and less than 5% as the metabolite. The main part of the dose is excreted in faeces as metabolites and unchanged drug. Other unidentified metabolites are also found in faeces. Care should be taken when co-administering known CYP3A4 inhibitors, as there is potential for increased systemic exposure to fluticasone propionate.
Special Patient Populations: SERETIDE Diskus: Population pharmacokinetic analysis was performed utilising data for asthmatic subjects (nine clinical studies for FP and five studies for salmeterol) and showed the following:
Higher FP exposure seen following administration of SERETIDE (50/100 micrograms) compared to FP alone (100 micrograms) in adolescents and adults (ratio 1.52 [90% CI 1.08, 2.13]) and children (ratio 1.20 [90% CI 1.06, 1.37]).
Higher FP exposure observed in children taking SERETIDE (50/100 micrograms) compared to adolescents and adults (ratio 1.63 [90% CI 1.35, 1.96]).
The clinical relevance of these findings are not known, however, no differences in HPA axis effects were observed in clinical studies of up to 12 weeks duration comparing SERETIDE (50/100 micrograms) and FP (100 micrograms) in both adolescents and adults and in children.
FP exposure was similar at the higher SERETIDE 50/500 microgram dose compared to the equivalent FP dose alone.
Higher salmeterol exposure was observed in children taking SERETIDE (50/100 micrograms) compared to adolescents and adults (ratio 1.23 [90% CI 1.10, 1.38]).
The clinical relevance of these findings are not known, however there were no differences observed in cardiovascular effects or reports of tremor between adults, adolescents and children in clinical studies of up to 12 weeks duration.
Toxicology: Non-Clinical Information: Salmeterol xinafoate and fluticasone propionate have been extensively evaluated in animal toxicity tests. Significant toxicities occurred only at doses in excess of those recommended for human use and were those expected for a potent beta
2-adrenoreceptor agonist and glucocorticosteroid. Neither salmeterol xinafoate nor fluticasone propionate have shown any potential for genetic toxicity.
In long term studies, salmeterol xinafoate induced benign tumours of smooth muscle in the mesovarium of rats and the uterus of mice.
Rodents are sensitive to the formation of these pharmacologically-induced tumours. Salmeterol is not considered to represent a significant oncogenic hazard to man.
Co-administration of salmeterol and fluticasone propionate resulted in some cardiovascular interactions at high doses. In rats, mild atrial myocarditis and focal coronary arteritis were transient effects that resolved with regular dosing. In dogs, heart rate increases were greater after co-administration than after salmeterol alone. No clinically relevant serious adverse cardiac effects have been observed in studies in man.
Co-administration did not modify other class-related toxicities in animals.
Inhaler: The non-CFC propellant, HFA134a, has been shown to have no toxic effect at very high vapour concentrations, far in excess of those likely to be experienced by patients, in a wide range of animal species exposed daily for periods of two years.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
