The information highlighted (if any) are the most recent updates for this brand.
Inactivated hepatitis A and rDNA hepatitis B vaccine (adsorbed).
One dose (1.0 mL) contains: Hepatitis A virus (inactivated)1,2 720 ELISA Units; Hepatitis B surface antigen3,4 20 micrograms.
1Produced on human diploid (MRC-5) cells.
2Adsorbed on aluminium hydroxide, hydrated 0.05 milligrams Al3+.
3Produced in yeast cells (Saccharomyces cerevisiae) by recombinant DNA technology.
4Adsorbed on aluminium phosphate 0.4 milligrams Al3+.
Excipients/Inactive Ingredients: Sodium chloride and water for injections. Aminoacids for injection, formaldehyde, neomycin sulphate and polysorbate 20 are present as residual from the manufacturing process.
Pharmaco-therapeutic group: Hepatitis vaccines. ATC code: J07BC20.
Pharmacology: Pharmacodynamics: Twinrix confers immunity against HAV and HBV infection by inducing specific anti-HAV and anti-HBs antibodies.
Children of 1 to 15 years of age: In clinical studies involving subjects from 1 to 15 years old, seropositivity rates for anti-HAV antibodies were 99.1% one month after the first dose and 100% after the second dose given at month 6 (i.e. month 7). Seropositivity rates for anti-HBs antibodies were 74.2% one month after the first dose and 100% after the second dose given at month 6 (i.e. month 7). The anti-HBs seroprotection rates (titres ≥10 mIU/mL) at these time points were 37.4% and 98.2% respectively.
In a clinical study conducted among 12 years up to and including 15 years old subjects who received the second dose at month 12, seropositivity rates for anti-HAV were 99.0% and seropositivity rates for anti-HBs were 99.0% at month 13 with seroprotection rates of 97.0%.
In a comparative study conducted in adolescents (from 12 years up to and including 15 years of age) vs an alternative schedule of 3 doses with the combined vaccine containing 360 ELISA Units inactivated HA virus and 10 µg HBsAg in a dose volume of 0.5 mL, seroprotection rates for anti-HBs at intermediate time points before the 2nd dose of Twinrix were lower compared to those obtained with the alternative schedule comprising 3 doses, but non-inferiority was shown after completion of the schedule (month 7).
Anti-HAV and anti-HBs antibodies have been shown to persist for at least 10 years following the initiation of a 0, 6 month schedule of Twinrix. After 10 years, anti-HAV seropositivity rates were 100% in both subjects aged 1-11 years and in subjects aged 12-15 years at primary vaccination. The anti-HBs seroprotection rates at this time point were 77.3% and 85.9%, respectively. In the study conducted in subjects aged 12-15 years at primary vaccination, the immune response for both antigen components was comparable to that seen after a 3-dose regimen of the combined vaccine containing 360 ELISA Units of inactivated hepatitis A virus and 10 μg of recombinant hepatitis B surface antigen in a dose volume of 0.5 mL.
In a 6 year long term follow-up study involving subjects aged 12-15 years at primary vaccination, anti-HAV seropositivity rates were 100% following a 0, 6 month or a 0, 12 month schedule. The anti-HBs seroprotection rates were 84.8% and 92.9%, respectively.
Adults and adolescents of 16 years of age and above: In adults aged 16 years and above administered a 3-dose schedule of Twinrix, protection against hepatitis A and hepatitis B develops within 2-4 weeks. In the clinical studies, specific humoral antibodies against hepatitis A were observed in approximately 94% of the adults one month after the first dose and in 100% one month after the third dose (i.e. month 7). Specific humoral antibodies against hepatitis B were observed in 70% of the adults after the first dose and approximately 99% after the third dose.
For use in exceptional circumstances in adults, the 0, 7 and 21 days primary schedule plus a fourth dose at month 12 results in 82% and 85% of vaccinees having seroprotective levels of anti-HBV antibodies at 1 and 5 weeks respectively following the third dose. One month after the fourth dose, all vaccinees demonstrated seroprotective levels of antibody. Seropositivity rates for anti-HAV antibodies were 100% and 99.5% at 1 and 5 weeks respectively following the third dose, and reached 100% one month after the fourth dose.
In a clinical study conducted in subjects over 40 years of age, the seropositivity rate for anti-HAV antibodies and seroprotection rate against hepatitis B following Twinrix on a 0, 1, 6 month schedule were compared with the seropositivity and seroprotection rates of monovalent hepatitis A and B vaccines when administered separately.
The seroprotection rates against hepatitis B after the administration of Twinrix were 92% and 57% at 7 and 48 months following the first dose respectively, versus 80% and 40% after the GlaxoSmithKline Biologicals monovalent 20 µg hepatitis B vaccine, and 71% and 27% after another licensed monovalent 10 µg hepatitis B vaccine. In all groups, anti-HBs antibody concentrations decreased as age and body mass index increased; concentrations were also lower in males compared with females.
The seropositivity rates for anti-HAV antibodies after Twinrix were 97% at both 7 and 48 months following the first dose versus 99% and 94% after the GlaxoSmithKline Biologicals monovalent hepatitis A vaccine and 99% and 96% after another licensed monovalent hepatitis A vaccine.
Subjects received an additional dose of Twinrix to assess the immune memory 48 months after the first dose of the primary vaccination course with the same vaccine. One month after this dose, 95% of subjects elicited anti-HBV antibody concentration ≥10 mIU/mL and Geometric Mean Concentrations (GMC) increased by 179-fold (GMC of 7233.7 mIU/mL) indicative of an immune memory response.
In two long-term clinical studies conducted in adults, 15 years after the primary vaccination with Twinrix the anti-HAV seropositivity rates were 100% in both studies and the anti-HBs seroprotection rates were 89.3% and 92.9%, respectively (n=56). The kinetics of decline of anti-HAV and anti-HBs antibodies were shown to be similar to those of the monovalent vaccines.
Toxicology: Pre-clinical Safety Data: Pre-clinical data reveal no special hazards for humans based on general safety studies (see Use in Pregnancy & Lactation).
Twinrix is indicated for use in non immune adults, adolescents and children aged from 2-15 years, who are at risk of both hepatitis A and hepatitis B infection and never been vaccinated or incomplete vaccinated course of hepatitis B.
Dosage: A dose of 1.0 mL Twinrix is recommended for adults, adolescents and children aged from 2-15 years.
Primary vaccination schedules: Adults and adolescents of 16 years of age and above: The standard primary course of vaccination with Twinrix consists of three doses, the first administered at the elected date, the second one month later and the third six months after the first dose.
In exceptional circumstances in adults, when travel is anticipated within one month or more after initiating the vaccination course, but where insufficient time is available to allow the standard 0, 1, 6 month schedule to be completed, a schedule of three intramuscular injections given at 0, 7 and 21 days may be used. When this schedule is applied, a fourth dose is recommended 12 months after the first dose.
Children of 2 to 15 years of age: The standard primary course of vaccination with Twinrix consists of two doses, the first is administered at the elected date and the second between six and twelve months after the first dose. As protection against hepatitis B infection will not be obtained in all vaccinees until after the second dose, it is important that the second dose be administered to assure protection against hepatitis B infection.
The recommended schedule should be adhered to. Once initiated, the primary course of vaccination should be completed with the same vaccine.
Booster dose: Long-term antibody persistence data following vaccination with Twinrix in adults with a 0, 1, 6 month schedule are available for up to 15 years after vaccination.
The anti-HBs and anti-HAV antibody titres observed following a primary vaccination course with the combined vaccine are in the range of what is seen following vaccination with the monovalent vaccines. Following vaccination with Twinrix in adults, the kinetics of antibody decline are similar to what has been observed after vaccination with the monovalent vaccines.
General guidelines for booster vaccination can therefore be drawn from experience with the monovalent vaccines.
Hepatitis B: The need for a booster dose of hepatitis B vaccine in healthy individuals who have received a full primary vaccination course has not been established; however some official vaccination programmes currently include a recommendation for a booster dose of hepatitis B vaccine and these should be respected.
For some categories of subjects or patients exposed to HBV (e.g. haemodialysis or immunocompromised patients) a precautionary attitude should be considered to ensure a protective antibody level ≥10 IU/L.
Hepatitis A: It is not yet fully established whether immunocompetent individuals who have responded to hepatitis A vaccination will require booster doses, as protection in the absence of detectable antibodies may be ensured by immunological memory. Guidelines for boosting are based on the assumption that antibodies are required for protection; anti-HAV antibodies have been shown to persist for at least 10 years.
In situations where a booster dose of both hepatitis A and hepatitis B are desired, Twinrix can be given. Alternatively, subjects primed with Twinrix may be administered a booster dose of either of the monovalent vaccines. The safety and immunogenicity of Twinrix administered as a booster dose following a two dose primary vaccination course have not been evaluated.
Method of administration: Twinrix should be injected intramuscularly into the deltoid region of the upper arm in adults, adolescents and children. The anterolateral thigh may be used in infants.
Since intradermal injection or intramuscular administration into the gluteal muscle could lead to a suboptimal response to the vaccine, these routes should be avoided. Exceptionally, Twinrix can be administered subcutaneously to subjects with thrombocytopenia or bleeding disorders since bleeding may occur following an intramuscular administration to these subjects. However, this route of administration may result in suboptimal immune response to the vaccine.
Cases of overdose have been reported during post-marketing surveillance after administration of Twinrix according to a three doses schedule. Adverse reactions reported following overdosage were similar to those reported with normal vaccine administration.
Twinrix should not be administered to subjects with known hypersensitivity to any constituent of the vaccine, or to subjects having shown signs of hypersensitivity after previous administration of Twinrix or the monovalent hepatitis A or hepatitis B vaccines.
As with other vaccines, the administration of Twinrix should be postponed in subjects suffering from acute severe febrile illness.
Syncope (fainting) can occur following, or even before, any vaccination as a psychogenic response to the needle injection. It is important that procedures are in place to avoid injury from faints.
It is possible that subjects may be in the incubation period of a hepatitis A or hepatitis B infection at the time of vaccination. It is not known whether Twinrix will prevent hepatitis A and hepatitis B in such cases.
The vaccine will not prevent infection caused by other agents such as hepatitis C and hepatitis E and other pathogens known to infect the liver.
Twinrix is not recommended for postexposure prophylaxis (e.g. needle stick injury).
The vaccine has not been tested in patients with impaired immunity. In haemodialysis patients and persons with an impaired immune system, adequate anti-HAV and anti-HBs antibody titres may not be obtained after the primary immunisation course and such patients may therefore require administration of additional doses of vaccine.
As with all injectable vaccines, appropriate medical treatment and supervision should always be readily available in case of a rare anaphylactic event following the administration of the vaccine.
Twinrix should under no circumstances be administered intravascularly.
Effects on Ability to Drive and Use Machines: The vaccine is unlikely to produce an effect on the ability to drive and use machines.
Pregnancy: Twinrix should be used during pregnancy only when clearly needed and when the possible advantages outweigh the possible risks for the foetus.
The effect of Twinrix on embryo-foetal, peri-natal and post-natal survival and development has not been prospectively evaluated in clinical trials.
The effect of Twinrix on embryo-foetal, peri-natal and post-natal survival and development has been assessed in rats. Such animal studies do not indicate direct or indirect harmful effects with respect to fertility, pregnancy, embryonal/foetal development, parturition or post-natal development.
Lactation: Adequate human data on use during lactation and adequate animal reproduction studies are not available. Twinrix should therefore be used with caution in breastfeeding women.
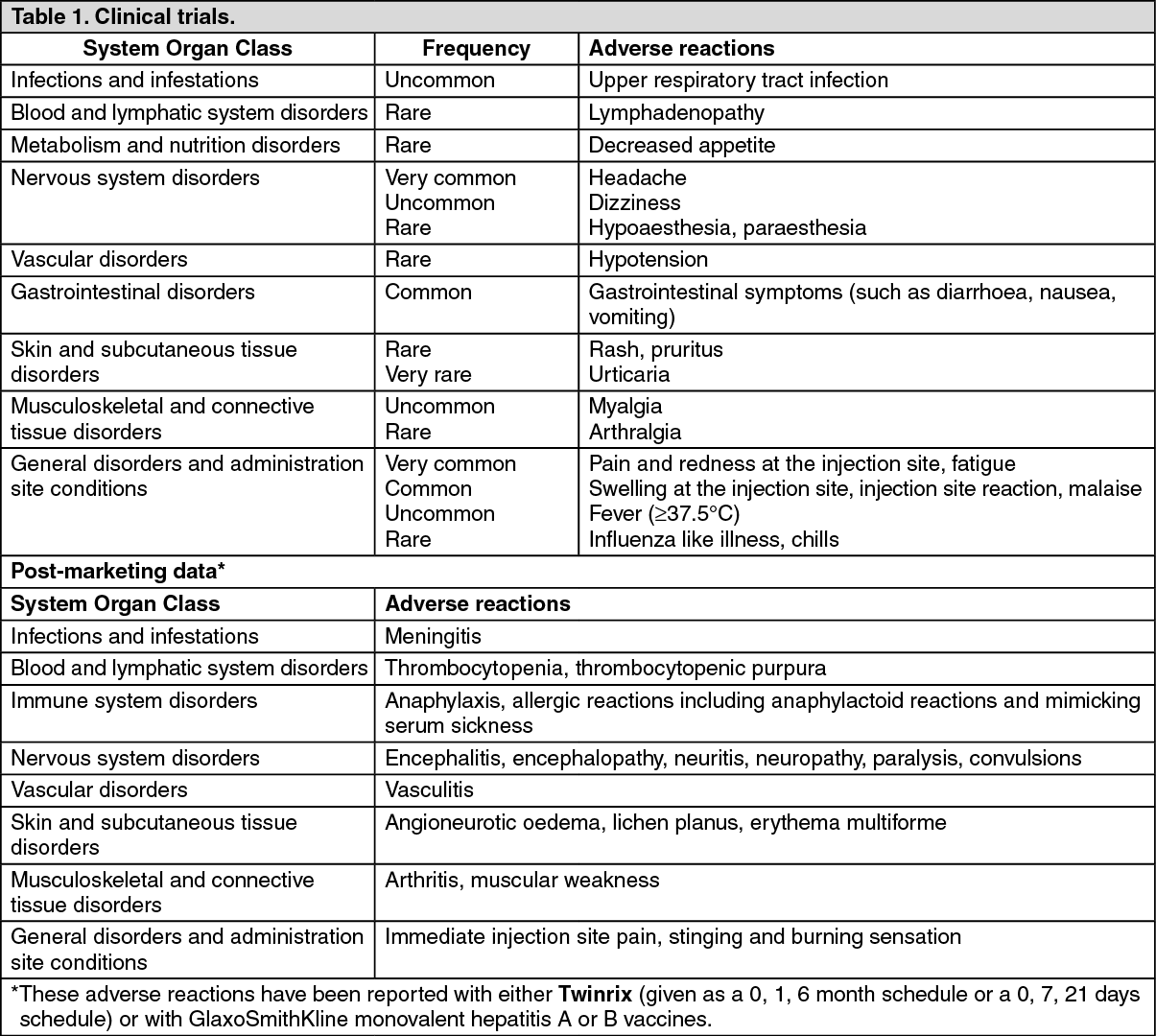
Local and general adverse events reported following primary vaccination with Twinrix were categorised by frequency.
Adverse reactions reported are listed according to the following frequency: Very common: ≥1/10; Common: ≥1/100 and <1/10; Uncommon: ≥1/1,000 and <1/100; Rare: ≥1/10,000 and <1/1,000; Very rare: <1/10,000.
Adults and adolescents of 16 years of age and above: The safety profile presented as follows is based on data from more than 6,000 subjects who received either the standard 0, 1, 6 month schedule or the accelerated 0, 7, 21 days schedule. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a comparative study it was noted that the frequency of solicited adverse events following the administration of Twinrix is not different from the frequency of solicited adverse events following the administration of the monovalent vaccines.
In a clinical trial where Twinrix was administered at 0, 7, 21 days, solicited general symptoms were reported with the same categories of frequency as defined previously. After a fourth dose given at month 12, the incidence of systemic adverse reactions was comparable to that seen after vaccination at 0, 7, 21 days.
Children of 1 to 15 years of age inclusive: Clinical trials involved the administration of 1,537 doses of Twinrix as a two dose schedule to 778 subjects from 1 year up to and including 15 years of age. (See Table 2.)
Click on icon to see table/diagram/image
No data on concomitant administration of Twinrix with specific hepatitis A immunoglobulin or hepatitis B immunoglobulin have been generated. However, when the monovalent hepatitis A and hepatitis B vaccines were administered concomitantly with specific immunoglobulins, no influence on seroconversion was observed although it may result in lower antibody titres.
Clinical studies have demonstrated that Twinrix can be administered concomitantly with diphtheria, tetanus, acellular pertussis, inactivated poliomyelitis, Haemophilus influenzae type b (DTPa-IPV/Hib) or Measles-Mumps-Rubella vaccines in the second year of life. In these trials, the injectable vaccines were given at different injection sites.
Although the concomitant administration of Twinrix and other vaccines has not specifically been studied, it is anticipated that, if different syringes and other injection sites are used, no interaction will be observed.
It may be expected that in patients receiving immunosuppressive treatment or patients with immunodeficiency, an adequate response may not be achieved.
Instructions for Use/Handling: The vaccine should be re-suspended before use. When re-suspended, the vaccine will have a uniform hazy white appearance.
Upon storage, a fine white deposit with a clear colourless layer above may be observed.
Re-suspension of the vaccine to obtain a uniform hazy white suspension: The vaccine can be re-suspended following these steps: 1. Hold the syringe upright in a closed hand.
2. Shake the syringe by tipping it upside down and back again.
3. Repeat this action vigorously for at least 15 seconds.
4. Inspect the vaccine again: If the vaccine appears as a uniform hazy white suspension, it is ready to use - the appearance should not be clear.
If the vaccine still does not appear as a uniform hazy white suspension - tip upside down and back again for at least another 15 seconds - then inspect again.
The vaccine should be inspected visually for any foreign particulate matter and/or abnormal physical appearance prior to administration. In the event of either being observed, do not administer the vaccine.
Any unused product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: Twinrix should not be mixed with other vaccines in the same syringe.
Twinrix should be stored at +2°C to +8°C.
Do not freeze; discard if the vaccine has been frozen.
Shelf-Life: 36 months.
J07BC20 - combinations ; Belongs to the class of hepatitis viral vaccines.
Twinrix vaccine (inj)
(pre-filled syringe) 1 mL x 1's





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image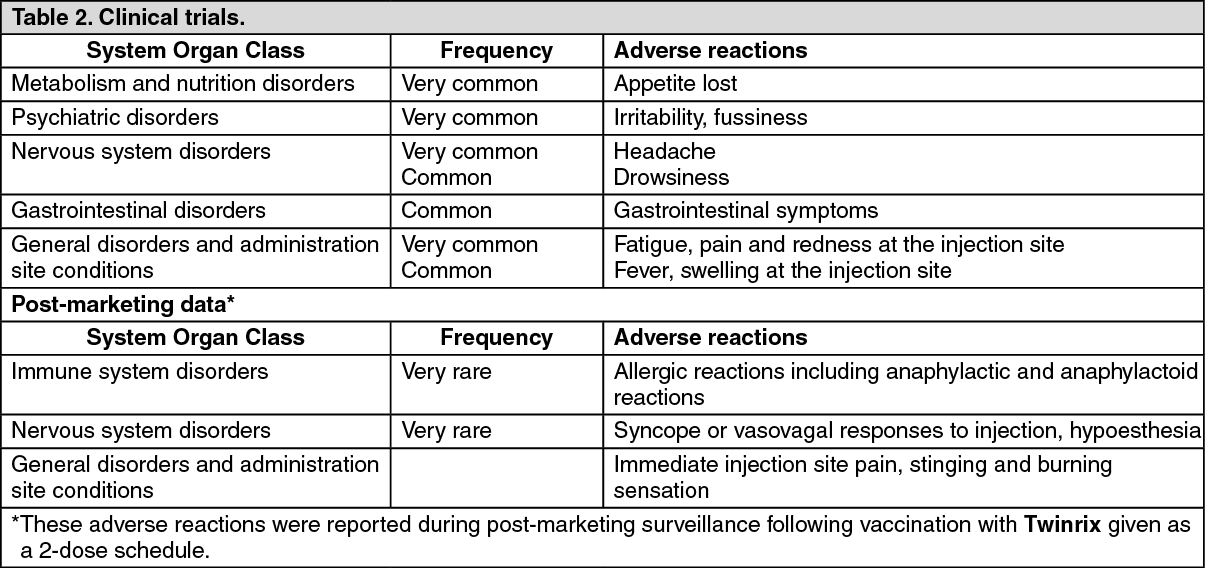 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageda679f96-6e67-4043-a84c-9fab018815af.GIF)

 Sign Out
Sign Out