Therapeutic Class: JANUMET: JANUMET (sitagliptin phosphate/metformin HCl) combines two antihyperglycemic agents with complementary mechanisms of action to improve glycemic control in patients with type 2 diabetes: sitagliptin phosphate, a dipeptidyl peptidase 4 (DPP-4) inhibitor, and metformin hydrochloride, a member of the biguanide class.
Sitagliptin phosphate: Sitagliptin phosphate is an orally-active, potent, and highly selective inhibitor of the dipeptidyl peptidase 4 (DPP-4) enzyme for the treatment of type 2 diabetes. The DPP-4 inhibitors are a class of agents that act as incretin enhancers. By inhibiting the DPP-4 enzyme, sitagliptin increases the levels of two known active incretin hormones, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). The incretins are part of an endogenous system involved in the physiologic regulation of glucose homeostasis. When blood glucose concentrations are normal or elevated, GLP-1 and GIP increase insulin synthesis and release from pancreatic beta cells. GLP-1 also lowers glucagon secretion from pancreatic alpha cells, leading to reduced hepatic glucose production. This mechanism is unlike the mechanism seen with sulfonylureas; sulfonylureas cause insulin release even when glucose levels are low, which can lead to sulfonylurea-induced hypoglycemia in patients with type 2 diabetes and in normal subjects. Sitagliptin is a potent and highly selective inhibitor of the enzyme DPP-4 and does not inhibit the closely-related enzymes DPP-8 or DPP-9 at therapeutic concentrations. Sitagliptin differs in chemical structure and pharmacological action from GLP-1 analogues, insulin, sulfonylureas or meglitinides, biguanides, peroxisome proliferator-activated receptor gamma (PPARγ) agonists, alpha-glucosidase inhibitors, and amylin analogues.
Metformin hydrochloride: Metformin is an antihyperglycemic agent which improves glucose tolerance in patients with type 2 diabetes, lowering both basal and postprandial plasma glucose. Its pharmacologic mechanisms of action are different from other classes of oral antihyperglycemic agents. Metformin decreases hepatic glucose production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization. Unlike sulfonylureas, metformin does not produce hypoglycemia in either patients with type 2 diabetes or normal subjects (except in special circumstances, see Metformin hydrochloride under Precautions) and does not cause hyperinsulinemia. With metformin therapy, insulin secretion remains unchanged while fasting insulin levels and day-long plasma insulin response may actually decrease.
Pharmacology: Mechanism of Action: JANUMET: JANUMET combines two antihyperglycemic agents with complementary mechanisms of action to improve glycemic control in patients with type 2 diabetes: sitagliptin phosphate, a dipeptidyl peptidase 4 (DPP-4) inhibitor, and metformin hydrochloride, a member of the biguanide class.
Sitagliptin phosphate: Sitagliptin phosphate is a member of a class of oral antihyperglycemic agents called dipeptidyl peptidase 4 (DPP-4) inhibitors, which improve glycemic control in patients with type 2 diabetes by enhancing the levels of active incretin hormones. Incretin hormones, including glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), are released by the intestine throughout the day, and levels are increased in response to a meal. The incretins are part of an endogenous system involved in the physiologic regulation of glucose homeostasis. When blood glucose concentrations are normal or elevated, GLP-1 and GIP increase insulin synthesis and release from pancreatic beta cells by intracellular signaling pathways involving cyclic AMP. Treatment with GLP-1 or with DPP-4 inhibitors in animal models of type 2 diabetes has been demonstrated to improve beta cell responsiveness to glucose and stimulate insulin biosynthesis and release. With higher insulin levels, tissue glucose uptake is enhanced. In addition, GLP-1 lowers glucagon secretion from pancreatic alpha cells. Decreased glucagon concentrations, along with higher insulin levels, lead to reduced hepatic glucose production, resulting in a decrease in blood glucose levels. The effects of GLP-1 and GIP are glucose-dependent. When blood glucose concentrations are low, stimulation of insulin release and suppression of glucagon secretion by GLP-1 are not observed. For both GLP-1 and GIP, stimulation of insulin secretion is enhanced as glucose rises above normal concentrations. GLP-1 does not impair the normal glucagon response to hypoglycemia. The activity of GLP-1 and GIP is limited by the DPP-4 enzyme, which rapidly hydrolyzes the incretin hormones to produce inactive products. Sitagliptin prevents the hydrolysis of incretin hormones by DPP-4, thereby increasing plasma concentrations of the active forms of GLP-1 and GIP. By enhancing active incretin levels, sitagliptin increases insulin release and decreases glucagon levels in a glucose-dependent manner. This glucose dependent mechanism is unlike the mechanism seen with sulfonylureas where insulin is released even when glucose levels are low, which can lead to hypoglycemia in patients with type 2 diabetes and in normal subjects. In patients with type 2 diabetes with hyperglycemia, these changes in insulin and glucagon levels lead to lower hemoglobin A
1c (HbA
1c) and lower fasting and postprandial glucose concentrations. Sitagliptin is a potent and highly selective inhibitor of the enzyme DPP-4 and does not inhibit the closely-related enzymes DPP-8 or DPP-9 at therapeutic concentrations.
Metformin hydrochloride: Metformin is an antihyperglycemic agent which improves glucose tolerance in patients with type 2 diabetes, lowering both basal and postprandial plasma glucose. Its pharmacologic mechanisms of action are different from other classes of oral antihyperglycemic agents. Metformin decreases hepatic glucose production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization. Unlike sulfonylureas, metformin does not produce hypoglycemia in either patients with type 2 diabetes or normal subjects (except in special circumstances, see Metformin hydrochloride under Precautions) and does not cause hyperinsulinemia. With metformin therapy, insulin secretion remains unchanged while fasting insulin levels and day-long plasma insulin response may actually decrease.
Pharmacodynamics: Sitagliptin phosphate: General: In patients with type 2 diabetes, administration of single oral doses of sitagliptin leads to inhibition of DPP-4 enzyme activity for a 24-hour period, resulting in a 2- to 3-fold increase in circulating levels of active GLP-1 and GIP, increased plasma levels of insulin and C-peptide, decreased glucagon concentrations, reduced fasting glucose, and reduced glucose excursion following an oral glucose load or a meal.
In Phase III clinical studies of 18- and 24-week duration, treatment with sitagliptin 100 mg daily in patients with type 2 diabetes significantly improved beta cell function, as assessed by several markers, including HOMA-β (Homeostasis Model Assessment-β), proinsulin to insulin ratio, and measures of beta cell responsiveness from the frequently-sampled meal tolerance test. In Phase II studies, sitagliptin 50 mg twice daily provided similar glycemic efficacy compared to sitagliptin 100 mg once daily.
In a randomized, placebo-controlled, double-blind, double-dummy, four-period crossover two-day study in healthy adult subjects, the effects on post-meal plasma concentrations of active and total GLP-1 and glucose after coadministration of sitagliptin and metformin were compared with those after administration of sitagliptin alone, metformin alone or placebo, each administered for two days. The incremental 4-hour post-meal weighted mean active GLP-1 concentrations were increased approximately 2-fold after either administration of sitagliptin alone or metformin alone compared with placebo. The effect on active GLP-1 concentrations after coadministration of sitagliptin and metformin were additive, with active GLP-1 concentrations increased by approximately 4-fold compared with placebo. Sitagliptin alone increased only active GLP-1 concentrations, reflecting inhibition of DPP-4, whereas metformin alone increased active and total GLP-1 concentrations to a similar extent. These data are consistent with different mechanisms for the increase in active GLP-1 concentrations. Results from the study also demonstrated that sitagliptin, but not metformin, enhances active GIP concentrations.
In studies with healthy subjects, sitagliptin did not lower blood glucose or cause hypoglycemia, suggesting that the insulinotropic and glucagon suppressive actions of the drug are glucose dependent.
Effects on blood pressure: In a randomized, placebo-controlled crossover study in hypertensive patients on one or more anti-hypertensive drugs (including angiotensin-converting enzyme inhibitors, angiotensin-II antagonists, calcium-channel blockers, beta-blockers and diuretics), coadministration with sitagliptin was generally well tolerated. In these patients, sitagliptin had a modest blood pressure lowering effect; 100 mg per day of sitagliptin reduced 24-hour mean ambulatory systolic blood pressure by approximately 2 mmHg, as compared to placebo. Reductions have not been observed in subjects with normal blood pressure.
Cardiac Electrophysiology: In a randomized, placebo-controlled crossover study, 79 healthy subjects were administered a single oral dose of sitagliptin 100 mg, sitagliptin 800 mg (8 times the recommended dose), and placebo. At the recommended dose of 100 mg, there was no effect on the QTc interval obtained at the peak plasma concentration, or at any other time during the study. Following the 800-mg dose, the maximum increase in the placebo-corrected mean change in QTc from baseline at 3 hours postdose was 8.0 msec. This small increase was not considered to be clinically significant. At the 800-mg dose, peak sitagliptin plasma concentrations were approximately 11 times higher than the peak concentrations following a 100-mg dose.
In patients with type 2 diabetes administered sitagliptin 100 mg (N=81) or sitagliptin 200 mg (N=63) daily, there were no meaningful changes in QTc interval based on ECG data obtained at the time of expected peak plasma concentration.
Clinical Studies: Clinical studies of the coadministration of sitagliptin and metformin demonstrated significant improvements in glycemic control in adult patients with type 2 diabetes. None of the clinical efficacy studies in adults described as follows was conducted with JANUMET tablets; however, bioequivalence of JANUMET tablets with coadministered sitagliptin and metformin hydrochloride tablets was demonstrated.
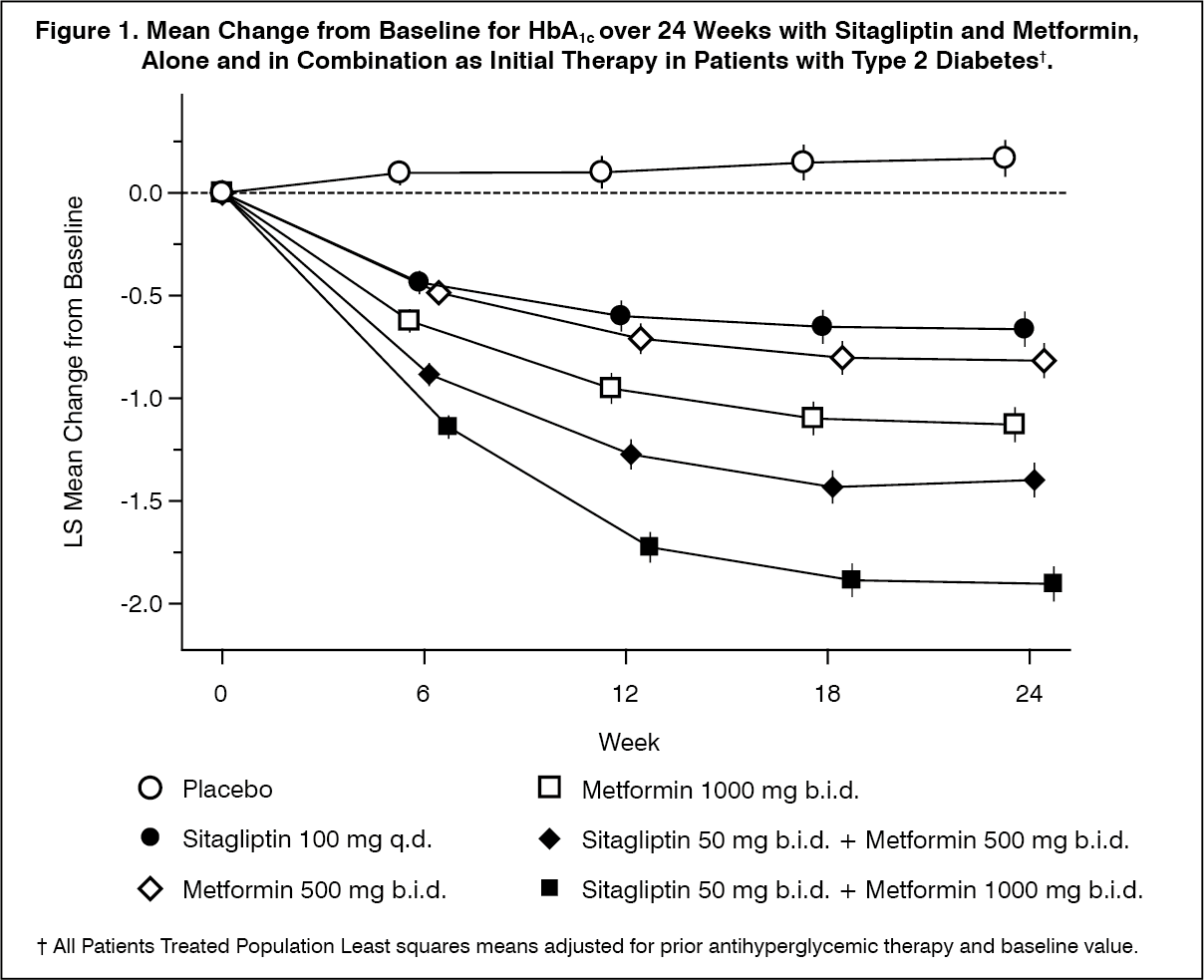
Sitagliptin and Metformin as Initial Therapy in Patients with Type 2 Diabetes: A total of 1091 patients with type 2 diabetes and inadequate glycemic control on diet and exercise participated in a 24-week, randomized, double-blind, placebo-controlled factorial study designed to assess the safety and efficacy of initial therapy with the combination of sitagliptin and metformin. Approximately equal numbers of patients were randomized to receive initial therapy with placebo; 100 mg of sitagliptin once daily; 500 mg or 1000 mg of metformin twice daily; or 50 mg of sitagliptin twice daily in combination with 500 mg or 1000 mg of metformin twice daily.
Initial therapy with the combination of sitagliptin and metformin provided significant improvements in HbA
1c, FPG, and 2-hour PPG compared to placebo, to metformin alone, and to sitagliptin alone (p<0.001; Table 1, Figure 1). An improvement in FPG, with near maximal FPG reduction, was achieved by the 3-week time point (the first time point assessed after initiation of therapy) and sustained throughout the 24-week study. Measures of beta cell function, HOMA-β and the proinsulin to insulin ratio also showed greater improvement with the coadministration of sitagliptin and metformin compared with either monotherapy alone. Lipid effects were generally neutral. The decrease in body weight in the groups given sitagliptin in combination with metformin was similar to that in the groups given metformin alone or placebo. Mean reductions from baseline in HbA
1c compared with placebo were generally greater for patients with higher baseline HbA
1c values. The improvement in HbA
1c was generally consistent across subgroups defined by gender, age, race, or baseline BMI. Mean reductions from baseline in HbA
1c for patients not on an antihyperglycemic agent at study entry were: sitagliptin 100 mg once daily, -1.06%; metformin 500 mg bid, -1.09%; metformin 1000 mg bid, -1.24%; sitagliptin 50 mg bid with metformin 500 mg bid, -1.59%; and sitagliptin 50 mg bid with metformin 1000 mg bid, -1.94%; and for patients receiving placebo, -0.17%. (See Figure 1 and Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In addition, this study included patients (N=117) with more severe hyperglycemia (HbA
1c >11% or blood glucose >280 mg/dL) who were treated with open-label sitagliptin at 50 mg and metformin at 1000 mg twice daily. In this group of patients, the baseline HbA
1c value was 11.15%, FPG was 314.4 mg/dL, and 2-hour PPG was 441.0 mg/dL. After 24 weeks, decreases from baseline of -2.94% for HbA
1c, -126.7 mg/dL for FPG, and -207.9 mg/dL for 2-hour PPG were observed. In this open-label cohort, a modest increase in body weight of 1.3 kg was observed at 24 weeks.
Sitagliptin Add-on Therapy in Patients Inadequately Controlled on Metformin Alone: The combination of sitagliptin and metformin has been evaluated for safety and efficacy in two double-blind, placebo-controlled clinical studies in patients with type 2 diabetes mellitus. In both studies, patients with inadequate glycemic control on stable doses of metformin ≥1500 mg were randomized to receive either sitagliptin 100 mg per day or placebo in addition to ongoing treatment with metformin.
In one study, 701 patients received 100 mg of sitagliptin or placebo once daily for 24 weeks. The addition of sitagliptin to ongoing metformin treatment provided significant improvements compared with the addition of placebo to ongoing metformin treatment in HbA
1c (-0.65%), FPG (-25.4 mg/dL), and 2-hour PPG (-50.6 mg/dL) (see Figure 2 and Table 2). This improvement in HbA
1c compared to placebo was not affected by baseline HbA
1c value, prior antihyperglycemic therapy, gender, age, baseline BMI, length of time since diagnosis of diabetes, presence of metabolic syndrome, or standard indices of insulin resistance (HOMA-IR) or insulin secretion (HOMA-β). Compared to patients taking placebo, patients taking sitagliptin demonstrated slight decreases in total cholesterol, non-HDL cholesterol and triglycerides. A similar decrease in body weight was observed for both treatment groups. (See Figure 2 and Table 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a separate study, 24-hour plasma glucose values were assessed. Twenty-eight patients received either 50 mg sitagliptin or placebo twice daily for 4 weeks in addition to their twice daily metformin regimen. Following 4 weeks of treatment, the difference in glucose lowering efficacy was assessed as a 24-hour weighted mean glucose (WMG) based upon collection of multiple blood samples, including those obtained before and after meals as well as overnight. Sitagliptin 50 mg coadministered twice daily with metformin significantly lowered the 24-hour WMG (-32.8 mg/dL) compared to placebo coadministered with metformin. In addition, sitagliptin administered with metformin, compared with placebo administered with metformin, substantially lowered fasting glucose concentrations and demonstrated smaller glucose excursions after all three meals (see Figure 3). In patient-collected glucose measurements, treatment with sitagliptin administered with metformin also provided significant reductions compared to placebo administered with metformin in mean fasting plasma glucose (-20.3 mg/dL), 7-point glucose average (-28.0 mg/dL), and 2-hour post-glucose concentrations (-36.6 mg/dL). (See Figure 3.)
Click on icon to see table/diagram/image
Sitagliptin Add-on Therapy in Patients Inadequately Controlled on the Combination of Metformin and Glimepiride: A total of 441 patients with type 2 diabetes participated in a 24-week, randomized, double-blind, placebo-controlled study designed to assess the efficacy of sitagliptin 100 mg once daily compared to placebo in combination with glimepiride (alone or in combination with metformin). In this study, 220 patients were on the combination of glimepiride (≥4 mg per day) and metformin (≥1500 mg per day); the results of the glycemic endpoints, including HbA
1c and FPG, are described as follows.
The combination of sitagliptin, glimepiride, and metformin provided significant reduction from baseline in HbA
1c (-0.89%) and FPG (-20.7 mg/dL) compared to placebo (see Table 3). Mean reductions from baseline in HbA
1c compared with placebo were generally greater for patients with higher baseline HbA
1c values. Patients treated with sitagliptin had a modest increase in body weight compared to those given placebo. (See Table 3.)
Click on icon to see table/diagram/image
Sitagliptin Add-on Therapy in Patients Inadequately Controlled on the Combination of Metformin and Rosiglitazone: A total of 262 patients with type 2 diabetes participated in a 54-week, randomized, double-blind, placebo-controlled study designed to assess the efficacy of sitagliptin in combination with metformin and rosiglitazone. Patients with inadequate glycemic control on a stable regimen of metformin (≥1500 mg per day) and rosiglitazone (≥4 mg per day) were randomized to the addition of either 100 mg of sitagliptin or placebo, administered once daily. Glycemic parameters were evaluated at the primary time point of Week 18 and at Week 54.
In combination with metformin and rosiglitazone, sitagliptin provided significant improvements in HbA
1c, FPG, and 2-hour PPG compared to placebo with metformin and rosiglitazone (Table 4, Figure 4) at Week 18, with improvements sustained through the end of the study. Lipid effects were generally neutral. There was no significant difference between sitagliptin and placebo in body weight change. (See Figure 4 and Table 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Sitagliptin Add-on Therapy in Patients Inadequately Controlled on the Combination of Metformin and Insulin: A total of 641 patients with type 2 diabetes participated in a 24-week, randomized, double-blind, placebo-controlled study designed to assess the efficacy of sitagliptin 100 mg once daily in combination with a stable dose of insulin. Approximately 75% of patients were also taking metformin. Patients on pre-mixed, long-acting or intermediate acting insulin (with or without metformin) were randomized to the addition of either 100 mg of sitagliptin or placebo. Glycemic endpoints measured included HbA
1c, FPG and 2-hour PPG.
The combination of sitagliptin, metformin and insulin provided significant improvements in HbA
1c, FPG and 2-hour PPG compared to placebo (Table 5). The improvement in HbA
1c compared to placebo was generally consistent across subgroups defined by gender, age, race, baseline BMI, length of time since diagnosis of diabetes, presence of metabolic syndrome, or standard indices of insulin resistance (HOMA-IR) or insulin secretion (HOMA-β). There was no meaningful change from baseline in body weight in either group. (See Table 5.)
Click on icon to see table/diagram/image
In another 24-week, randomized, double-blind, placebo-controlled study designed to assess the insulin-sparing efficacy of sitagliptin as add-on combination therapy, 660 patients with inadequate glycemic control on insulin glargine with or without metformin (≥1500 mg per day) were randomized to the addition of either 100 mg of sitagliptin (N=330) or placebo (N=330), administered once daily while undergoing intensification of insulin therapy. Among patients taking metformin, baseline HbA
1c was 8.70% and baseline insulin dose was 37 IU/day. Patients were instructed to titrate their insulin glargine dose based on fingerstick fasting glucose values. Glycemic endpoints measured included HbA
1c and FPG.
Among patients taking metformin, at Week 24, the increase in daily insulin dose was 21% smaller in patients treated with sitagliptin (19 IU/day, N=285) than in patients treated with placebo (24 IU/day, N=283). The difference in insulin dose (-5 IU/day) was statistically significant (p=0.007). The reduction in HbA
1c for patients treated with sitagliptin, metformin, and insulin was -1.35% compared to -0.90% for patients treated with placebo, metformin, and insulin, a difference of -0.45% [95% CI: -0.62, -0.29]. The reduction in FPG for patients treated with sitagliptin, metformin, and insulin was -54.8 mg/dL compared to -43.0 mg/dL for patients treated with placebo, metformin, and insulin, a difference of -11.8 mg/dL [95% CI: -18.7, -4.9]. The incidence of hypoglycemia was 24.9% for patients treated with sitagliptin, metformin, and insulin and 37.8% for patients treated with placebo, metformin and insulin. The difference in incidence of hypoglycemia (-12.9%) was statistically significant (p<0.001).
Active (Glipizide)-Controlled Study in Combination with Metformin: Long-term maintenance of effect was evaluated in a 52-week, double-blind, glipizide-controlled trial in patients with type 2 diabetes and inadequate glycemic control on metformin monotherapy at ≥1500 mg/day. In this study, patients were randomized to the addition of either sitagliptin 100 mg daily (N=588) or glipizide (N=584) for 52 weeks. Patients receiving glipizide were given an initial dosage of 5 mg/day and then electively titrated by the investigator to a target FPG of <110 mg/dL, without significant hypoglycemia, over the next 18 weeks. A maximum dosage of 20 mg/day was allowed to optimize glycemic control. Thereafter, the glipizide dose was to have been kept constant. The mean dose of glipizide after the titration period was 10.3 mg.
Both treatments resulted in a statistically significant improvement in glycemic control from baseline. After 52 weeks, the reduction from baseline in HbA
1c was 0.67% for sitagliptin 100 mg daily and 0.67% for glipizide, confirming comparable efficacy of the two agents. The reduction in FPG was 10.0 mg/dL for sitagliptin and 7.5 mg/dL for glipizide. In a post-hoc analysis, patients with higher baseline HbA
1c (≥9%) in both groups had greater reductions from baseline in HbA
1c (sitagliptin, -1.68%; glipizide, -1.76%). In this study, the proinsulin to insulin ratio, a marker of efficiency of insulin synthesis and release, improved with sitagliptin and deteriorated with glipizide treatment. The incidence of hypoglycemia in the sitagliptin group (4.9%) was significantly lower than that in the glipizide group (32.0%). Patients treated with sitagliptin exhibited a significant mean decrease from baseline in body weight compared to a significant weight gain in patients administered glipizide (-1.5 kg vs. +1.1 kg).
Metformin hydrochloride: The prospective randomized (UKPDS) study has established the long-term benefit of intensive blood glucose control in type 2 diabetes. Analysis of the results for overweight patients treated with metformin after failure of diet alone showed: a significant reduction of the absolute risk of any diabetes-related complication in the metformin group (29.8 events/1000 patient-years) versus diet alone (43.3 events/1000 patient-years), p=0.0023, and versus the combined sulphonylurea and insulin monotherapy groups (40.1 events/1000 patient-years), p=0.0034.
A significant reduction of the absolute risk of diabetes-related mortality: metformin 7.5 events/1000 patient-years, diet alone 12.7 events/1000 patient-years, p=0.017.
A significant reduction of the absolute risk of overall mortality: metformin 13.5 events/1000 patient-years versus diet alone 20.6 events/1000 patient-years (p=0.011), and versus the combined sulphonylurea and insulin monotherapy groups 18.9 events/1000 patient-years (p=0.021).
A significant reduction in the absolute risk of myocardial infarction: metformin 11 events/1000 patient-years, diet alone 18 events/1000 patient-years (p=0.01).
TECOS Cardiovascular Safety Study: The Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS) was a randomized study in 14,671 patients in the intention-to-treat population with an HbA
1c of ≥6.5 to 8.0% with established CV disease who received sitagliptin (7,332) 100 mg daily (or 50 mg daily if the baseline eGFR was ≥30 and <50 mL/min/1.73 m
2) or placebo (7,339) added to usual care targeting regional standards for HbA
1c and CV risk factors. Patients with an eGFR <30 mL/min/1.73 m
2 were not to be enrolled in the study. The study population included 2,004 patients ≥75 years of age and 3,324 patients with renal impairment (eGFR <60 mL/min/1.73 m
2).
Over the course of the study, the overall estimated mean (SD) difference in HbA
1c between the sitagliptin and placebo groups was 0.29% (0.01), 95% CI (-0.32, -0.27); p<0.001.
The primary cardiovascular endpoint was a composite of the first occurrence of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for unstable angina. Secondary cardiovascular endpoints included the first occurrence of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke; first occurrence of the individual components of the primary composite; all-cause mortality; and hospital admissions for congestive heart failure.
After a median follow up of 3 years, sitagliptin, when added to usual care, did not increase the risk of major adverse cardiovascular events or the risk of hospitalization for heart failure compared to usual care without sitagliptin in patients with type 2 diabetes (Table 6). (See Table 6.)
Click on icon to see table/diagram/image
Sitagliptin Add-on Therapy in Pediatric Patients Inadequately Controlled on Metformin with or without Insulin: A combined total of 220 pediatric patients aged 10 to 17 years with type 2 diabetes and inadequate glycemic control on metformin with or without insulin participated in two randomized, double-blind, placebo-controlled, parallel-group studies over 54 weeks. The addition of sitagliptin 100 mg (administered as JANUMET or JANUMET XR) was compared to the addition of placebo to metformin or metformin XR.
Superiority of HbA
1c reduction was demonstrated for JANUMET/JANUMET XR over metformin at Week 20 in the pooled analysis of these two studies. The reduction in HbA
1c in patients treated with JANUMET/JANUMET XR (N=107) was -0.6% compared to -0.1% in patients treated with metformin (N=113), a difference of -0.5% (95% CI: -0.9, -0.1). However, results from the individual studies were inconsistent, and efficacy for JANUMET/JANUMET XR over metformin was not observed at Week 54. These results do not support use of JANUMET or JANUMET XR in pediatric subjects (10 to 17 years old) with type 2 diabetes.
Pharmacokinetics: JANUMET: The results of a definitive bioequivalence study in healthy subjects demonstrated that the JANUMET (sitagliptin/metformin hydrochloride) 50 mg/500 mg and 50 mg/1000 mg combination tablets are bioequivalent to coadministration of corresponding doses of sitagliptin phosphate (JANUVIA) and metformin hydrochloride as individual tablets.
Because bioequivalence is demonstrated at the lowest and highest combination tablet dose strengths available, bioequivalence is conferred to the (sitagliptin/metformin) 50 mg/850 mg fixed dose combination (FDC) tablet.
Absorption: Sitagliptin phosphate: The absolute bioavailability of sitagliptin is approximately 87%. Coadministration of a high-fat meal with sitagliptin phosphate had no effect on the pharmacokinetics of sitagliptin.
Metformin hydrochloride: The absolute bioavailability of a metformin hydrochloride 500 mg tablet given under fasting conditions is approximately 50-60%. Studies using single oral doses of metformin hydrochloride tablets 500 mg to 1500 mg, and 850 mg to 2550 mg, indicate that there is a lack of dose proportionality with increasing doses, which is due to decreased absorption rather than an alternation in elimination. Food decreases the extent of and slightly delays the absorption of metformin, as shown by approximately a 40% lower mean peak plasma concentration (C
max), a 25% lower area under the plasma concentration versus time curve (AUC), and a 35-minute prolongation of time to peak plasma concentration (T
max) following administration of a single 850-mg tablet of metformin with food, compared to the same tablet strength administered fasting. The clinical relevance of these decreases is unknown.
Distribution: Sitagliptin phosphate: The mean volume of distribution at steady state following a single 100-mg intravenous dose of sitagliptin to healthy subjects is approximately 198 liters. The fraction of sitagliptin reversibly bound to plasma proteins is low (38%).
Metformin hydrochloride: The apparent volume of distribution (V/F) of metformin following single oral doses of metformin hydrochloride tablets 850 mg averaged 654±358 L. Metformin is negligibly bound to plasma proteins, in contrast to sulfonylureas, which are more than 90% protein bound. Metformin partitions into erythrocytes, most likely as a function of time. At usual clinical doses and dosing schedules of metformin hydrochloride tablets, steady state plasma concentrations of metformin are reached within 24-48 hours and are generally <1 mcg/mL. During controlled clinical trials of metformin, maximum metformin plasma levels did not exceed 5 mcg/mL, even at maximum doses.
Metabolism: Sitagliptin phosphate: Sitagliptin is primarily eliminated unchanged in urine, and metabolism is a minor pathway. Approximately 79% of sitagliptin is excreted unchanged in the urine.
Following a [
14C]sitagliptin oral dose, approximately 16% of the radioactivity was excreted as metabolites of sitagliptin. Six metabolites were detected at trace levels and are not expected to contribute to the plasma DPP-4 inhibitory activity of sitagliptin.
In vitro studies indicated that the primary enzyme responsible for the limited metabolism of sitagliptin was CYP3A4, with contribution from CYP2C8.
Metformin hydrochloride: Intravenous single-dose studies in normal subjects demonstrate that metformin is excreted unchanged in the urine and does not undergo hepatic metabolism (no metabolites have been identified in humans) nor biliary excretion.
Elimination: Sitagliptin phosphate: Following administration of an oral [
14C]sitagliptin dose to healthy subjects, approximately 100% of the administered radioactivity was eliminated in feces (13%) or urine (87%) within one week of dosing. The apparent terminal t
1/2 following a 100-mg oral dose of sitagliptin was approximately 12.4 hours and renal clearance was approximately 350 mL/min.
Elimination of sitagliptin occurs primarily via renal excretion and involves active tubular secretion. Sitagliptin is a substrate for human organic anion transporter-3 (hOAT-3), which may be involved in the renal elimination of sitagliptin. The clinical relevance of hOAT-3 in sitagliptin transport has not been established. Sitagliptin is also a substrate of p-glycoprotein, which may also be involved in mediating the renal elimination of sitagliptin. However, cyclosporine, a p-glycoprotein inhibitor, did not reduce the renal clearance of sitagliptin.
Metformin hydrochloride: Renal clearance is approximately 3.5 times greater than creatinine clearance, which indicates that tubular secretion is the major route of metformin elimination. Following oral administration, approximately 90% of the absorbed drug is eliminated via the renal route within the first 24 hours, with a plasma elimination half-life of approximately 6.2 hours. In blood, the elimination half-life is approximately 17.6 hours, suggesting that the erythrocyte mass may be a compartment of distribution.
Characteristics in Patients: Type 2 Diabetes: Sitagliptin phosphate: The pharmacokinetics of sitagliptin in patients with type 2 diabetes are generally similar to those in healthy subjects.
Metformin hydrochloride: In the presence of normal renal function, there are no differences between single- or multiple-dose pharmacokinetics of metformin between patients with type 2 diabetes and normal subjects, nor is there any accumulation of metformin in either group at usual clinical doses.
Renal Impairment: Sitagliptin phosphate: An approximately 2-fold increase in the plasma AUC of sitagliptin was observed in patients with moderate renal impairment with eGFR of 30 to <45 mL/min/1.73 m
2, and an approximately 4- fold increase was observed in patients with severe renal impairment (eGFR <30 mL/min/1.73 m
2) including patients with end-stage renal disease (ESRD) on hemodialysis, as compared to subjects with normal renal function.
Metformin hydrochloride: In patients with decreased renal function, the plasma and blood half-life of metformin is prolonged and the renal clearance is decreased (see Contraindications and Precautions).
Hepatic Impairment: Sitagliptin phosphate: In patients with moderate hepatic impairment (Child-Pugh score 7 to 9), mean AUC and C
max of sitagliptin increased approximately 21% and 13%, respectively, compared to healthy matched controls following administration of a single 100-mg dose of sitagliptin phosphate. These differences are not considered to be clinically meaningful.
There is no clinical experience in patients with severe hepatic impairment (Child-Pugh score >9). However, because sitagliptin is primarily renally eliminated, severe hepatic impairment is not expected to affect the pharmacokinetics of sitagliptin.
Metformin hydrochloride: No pharmacokinetic studies of metformin have been conducted in patients with hepatic impairment.
Gender: Sitagliptin phosphate: Gender had no clinically meaningful effect on the pharmacokinetics of sitagliptin based on a composite analysis of Phase I pharmacokinetic data and on a population pharmacokinetic analysis of Phase I and Phase II data.
Metformin hydrochloride: Metformin pharmacokinetic parameters did not differ significantly between normal subjects and patients with type 2 diabetes when analyzed according to gender. Similarly, in controlled clinical studies in patients with type 2 diabetes, the antihyperglycemic effect of metformin was comparable in males and females.
Elderly: Sitagliptin phosphate: Age did not have a clinically meaningful impact on the pharmacokinetics of sitagliptin based on a population pharmacokinetic analysis of Phase I and Phase II data. Elderly subjects (65 to 80 years) had approximately 19% higher plasma concentrations of sitagliptin compared to younger subjects.
Metformin hydrochloride: Limited data from controlled pharmacokinetic studies of metformin in healthy elderly subjects suggest that total plasma clearance of metformin is decreased, the half life is prolonged, and C
max is increased, compared to healthy young subjects. From these data, it appears that the change in metformin pharmacokinetics with aging is primarily accounted for by a change in renal function (see GLUCOPHAGE prescribing information).
Pediatric: The pharmacokinetics of sitagliptin (single dose of 50 mg, 100 mg or 200 mg) were investigated in pediatric patients (10 to 17 years of age) with type 2 diabetes. In this population, the dose-adjusted AUC of sitagliptin in plasma was approximately 18% lower compared to adult patients with type 2 diabetes for a 100 mg dose. This is not considered to be a clinically meaningful difference based on the flat PK/PD relationship between the dose of 50 mg and 100 mg in adults.
No studies with sitagliptin have been performed in pediatric patients <10 years of age.
Race: Sitagliptin phosphate: Race had no clinically meaningful effect on the pharmacokinetics of sitagliptin based on a composite analysis of Phase I pharmacokinetic data and on a population pharmacokinetic analysis of Phase I and Phase II data, including subjects of white, Hispanic, black, Asian, and other racial groups.
Metformin hydrochloride: No studies of metformin pharmacokinetic parameters according to race have been performed. In controlled clinical studies of metformin in patients with type 2 diabetes, the antihyperglycemic effect was comparable in whites (n=249), blacks (n=51), and Hispanics (n=24).
Body Mass Index (BMI): Sitagliptin phosphate: Body mass index (BMI) had no clinically meaningful effect on the pharmacokinetics of sitagliptin based on a composite analysis of Phase I pharmacokinetic data and on a population pharmacokinetic analysis of Phase I and Phase II data.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image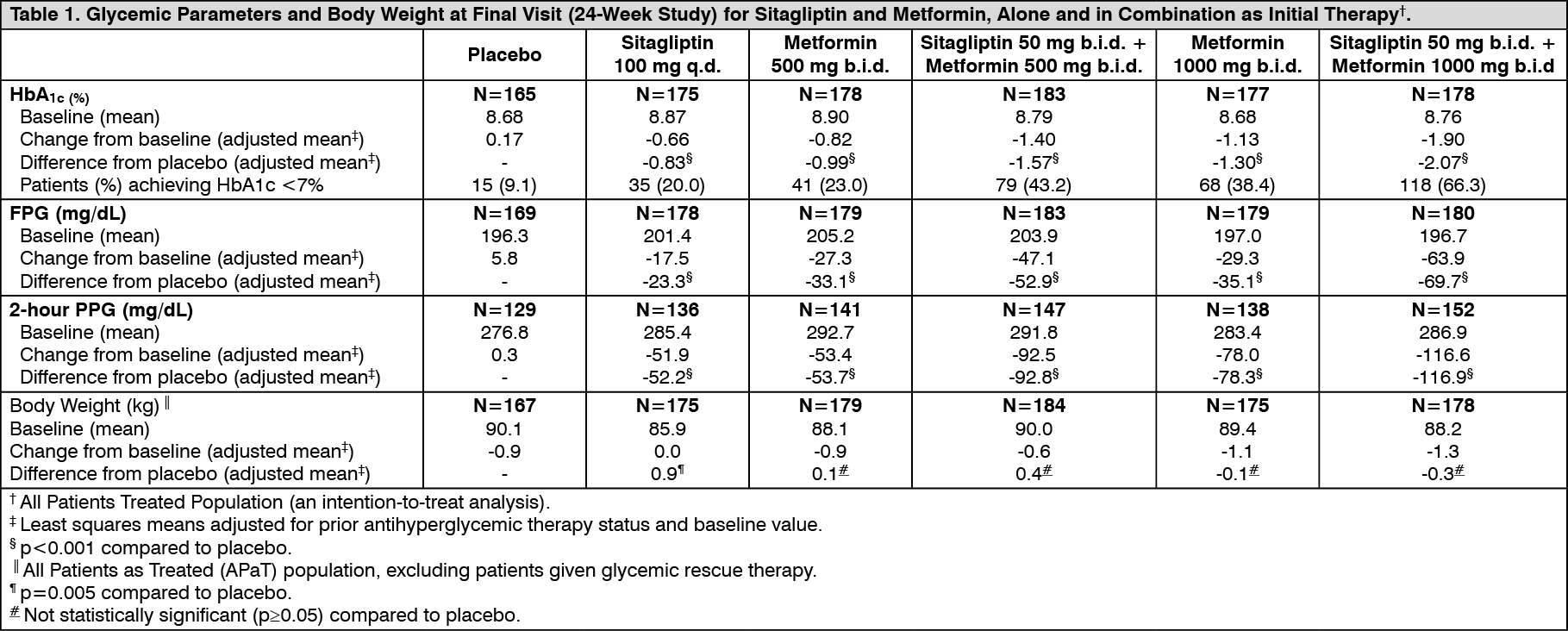 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image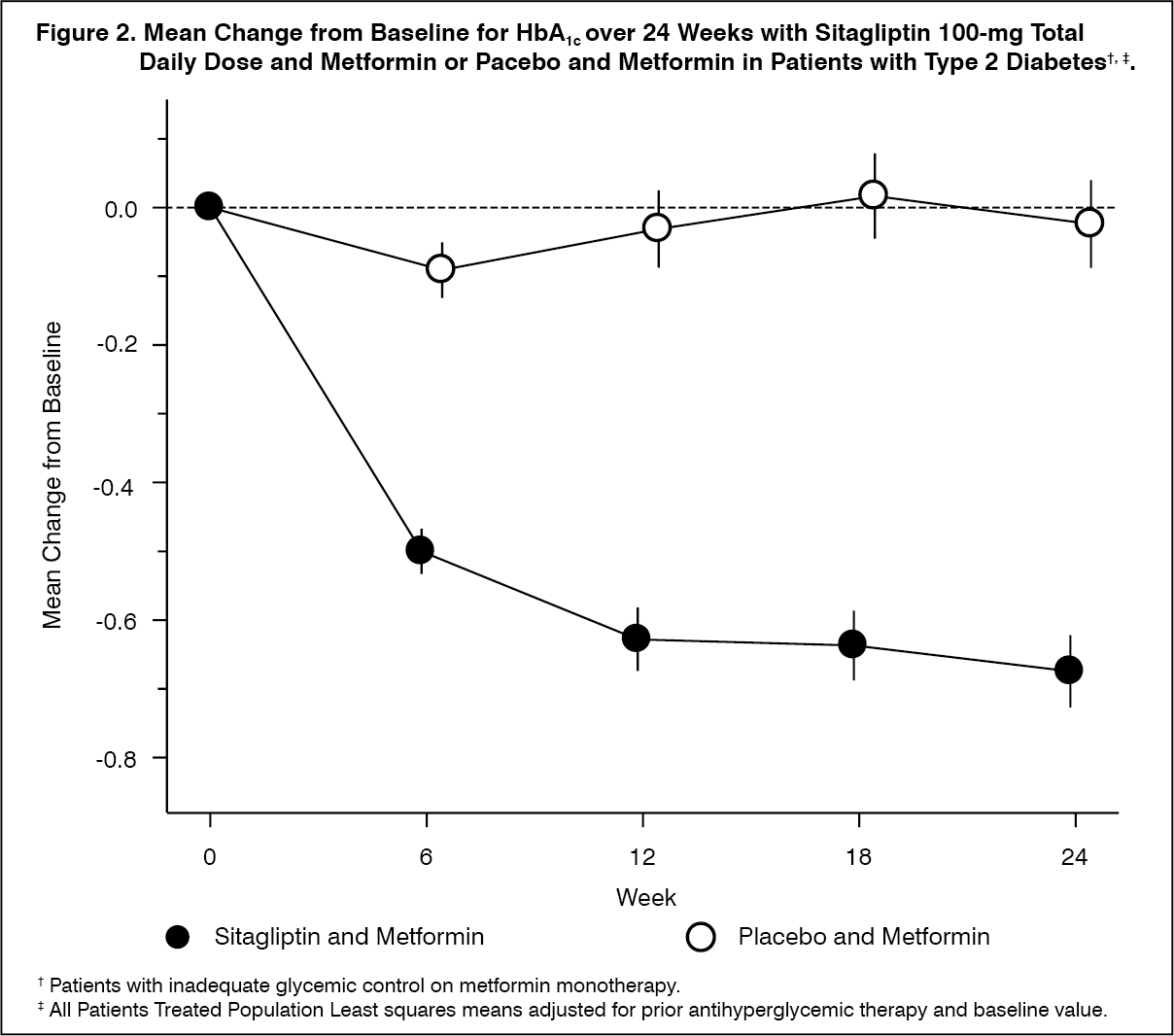 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image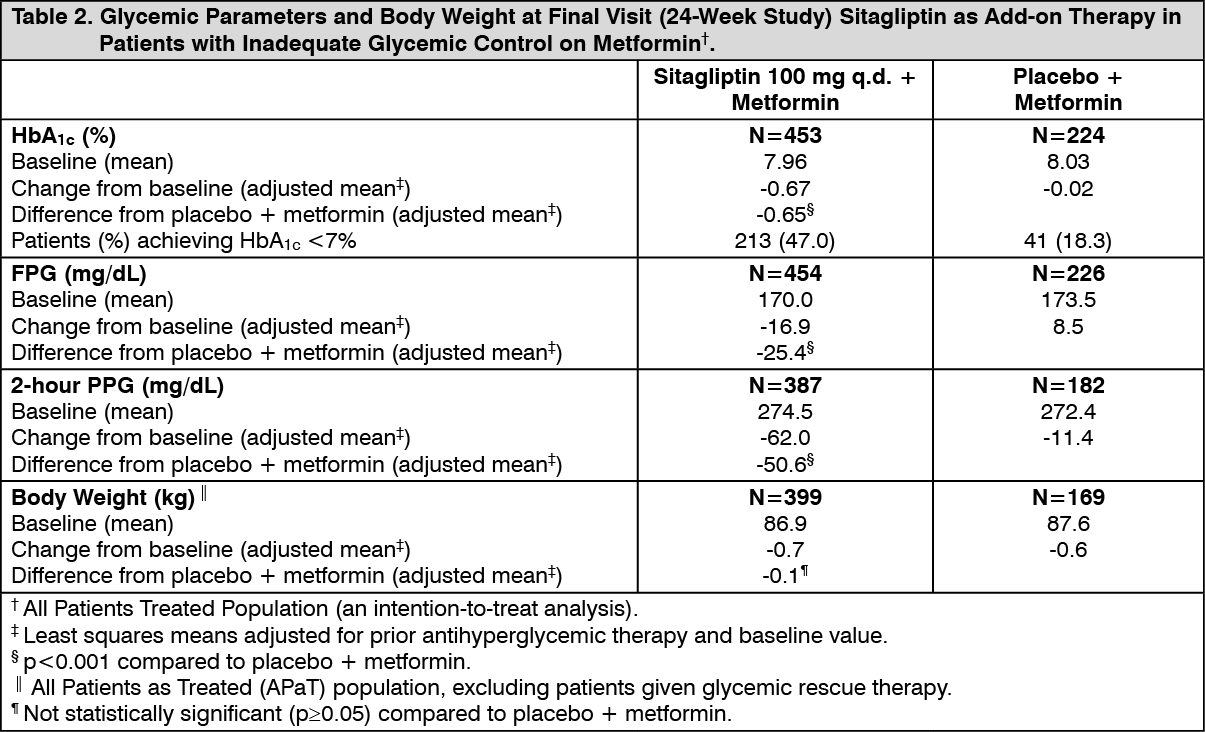 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image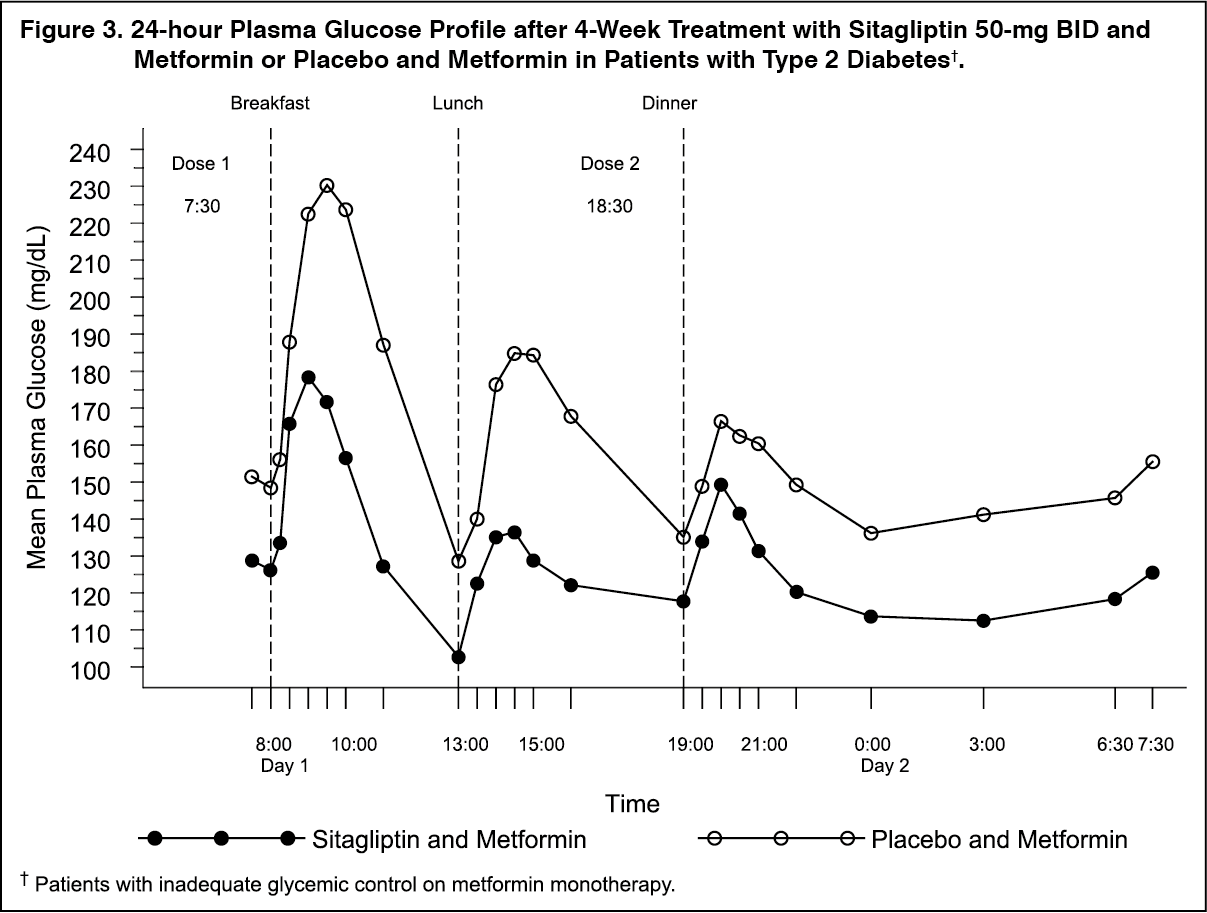 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image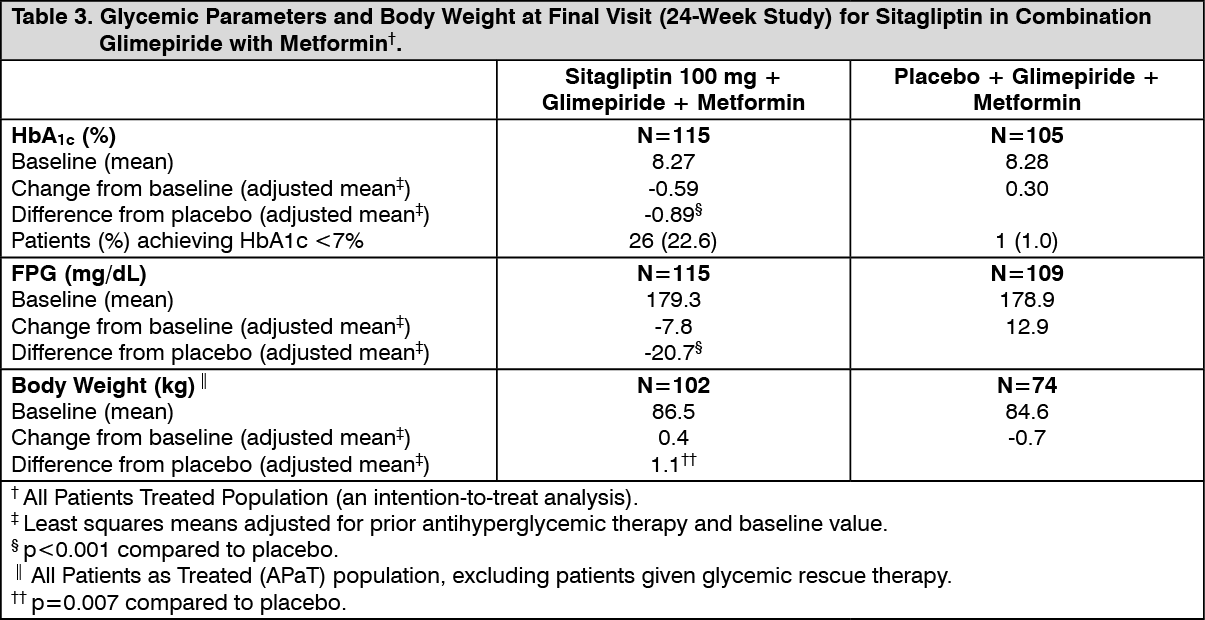 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image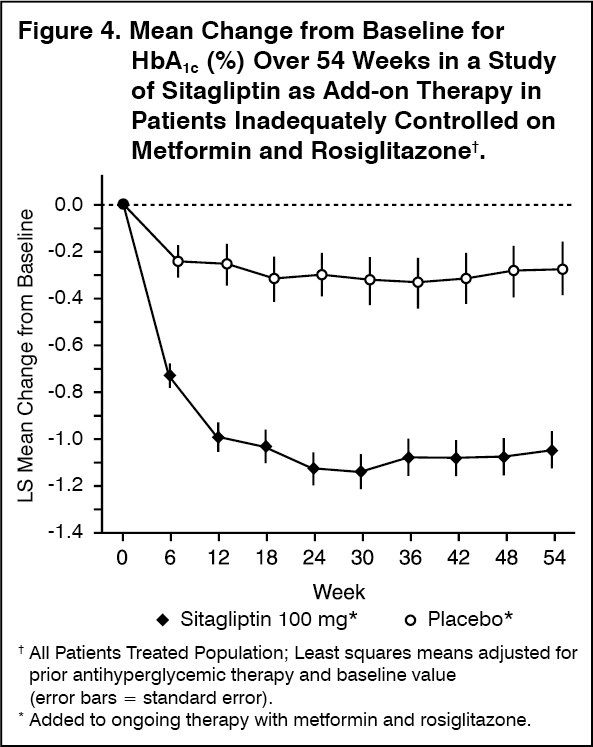 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image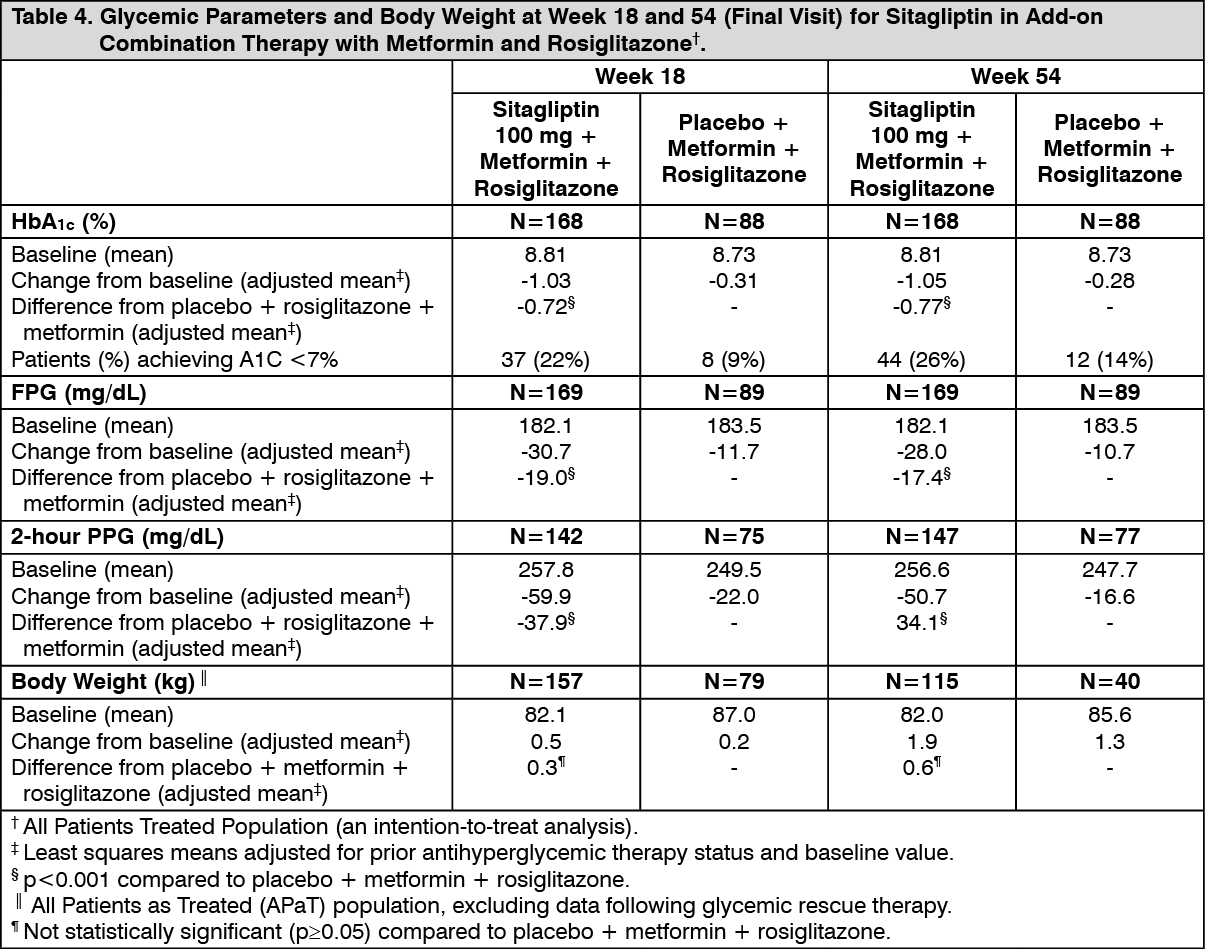 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image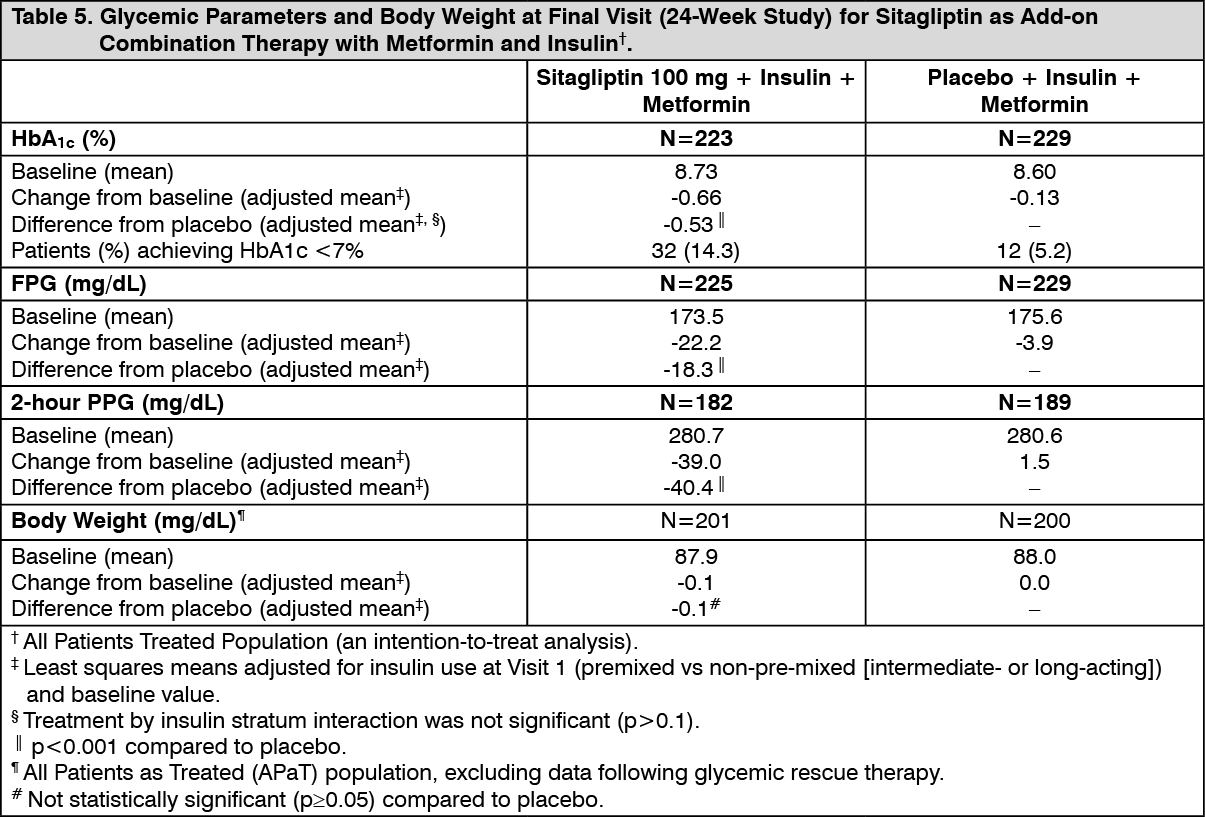 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image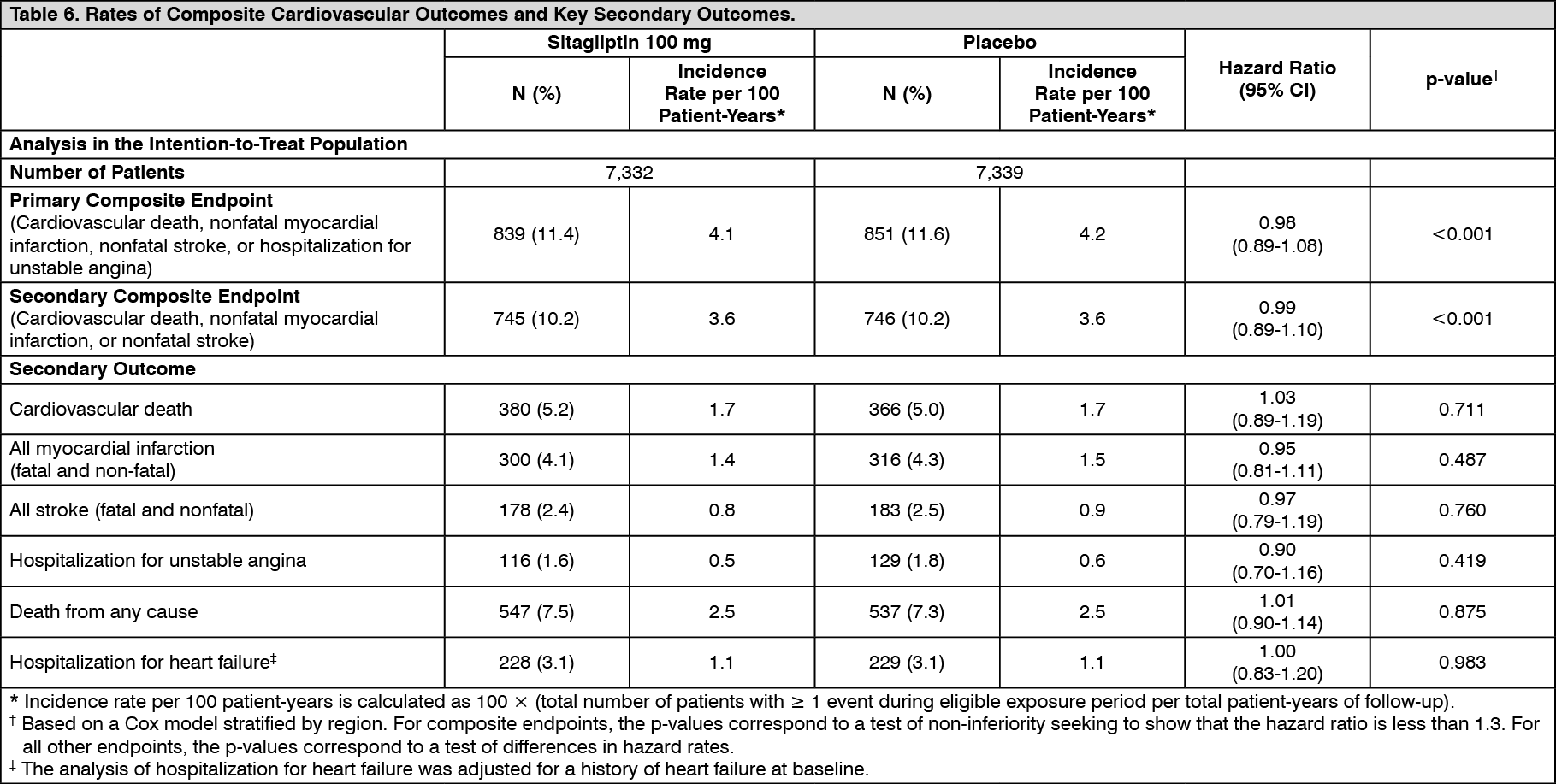 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image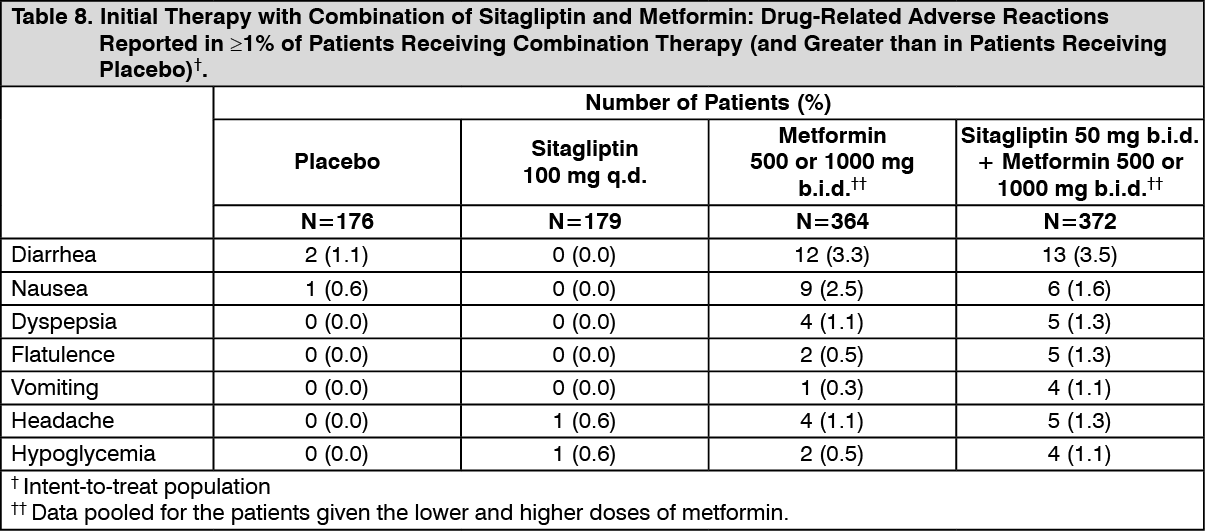 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image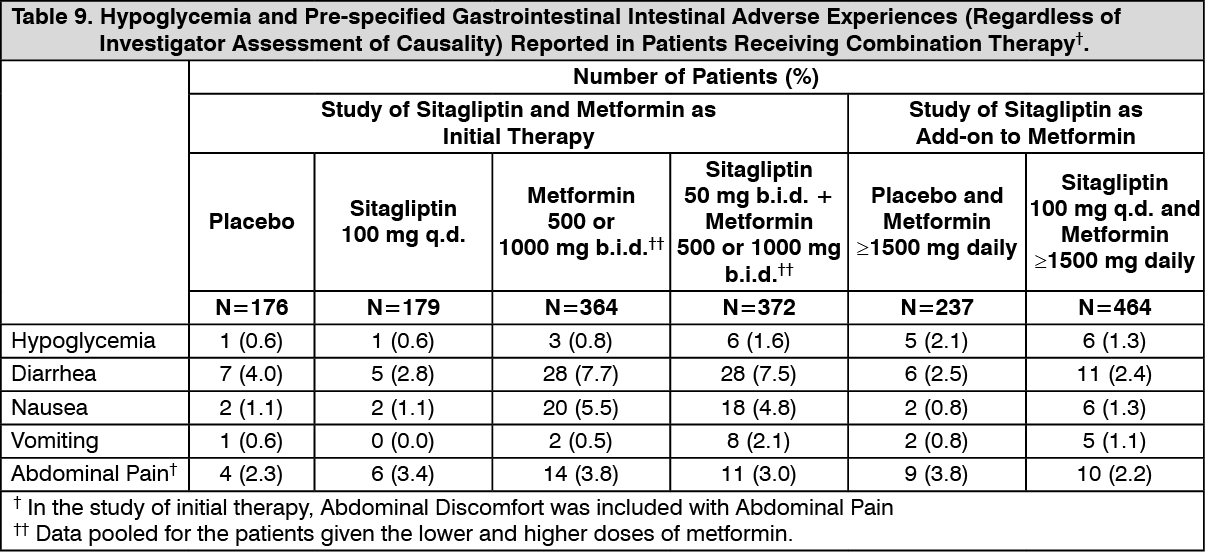 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
