White
to off-white powder filled in white opaque body, red opaque cap, hard gelatin
capsule No. 4 printed with black ink "BC 75".
Source
of Capsule shells: Bovine gelatin.
Each hard capsule contains 75 mg pregabalin.
Pharmacology: Pharmacodynamics: The active substance, pregabalin, is a gamma-aminobutyric acid analogue ((S)-3-(aminomethyl)-5-methylhexanoic acid).
Mechanism of action: Pregabalin binds to an auxiliary subunit (α2-δ protein) of voltage-gated calcium channels in the central nervous system.
Evidence from animal models with nerve damage has shown that pregabalin reduces calcium dependent release of pronociceptive neurotransmitters in the spinal cord possibly by disrupting calcium trafficking and/or reducing calcium currents. Evidence from other animal models of nerve damage suggests the antinociceptive activities of pregabalin may also be mediated through interactions with the descending noradrenergic and serotonergic pathways.
Clinical experience: Neuropathic pain: Efficacy has been shown in studies in diabetic neuropathy and post-herpetic neuralgia. Efficacy has not been studied in other models of neuropathic pain.
Pregabalin has been studied in 9 controlled clinical studies of up to 13 weeks with twice a day dosing and up to 8 weeks with three times a day dosing. Overall, the safety and efficacy profiles for twice a day and three times a day dosing regimens were similar.
In clinical trials up to 13 weeks, a reduction in pain was seen by Week 1 and was maintained throughout the treatment period.
In controlled clinical trials 35% of the pregabalin treated patients and 18% of the patients on placebo had a 50% improvement in pain score. For patients not experiencing somnolence, such an improvement was observed in 33% of patients treated with pregabalin and 18% of patients on placebo. For patients who experienced somnolence the responder rates were 48% on pregabalin and 16% on placebo.
Fibromyalgia: Pregabalin as monotherapy has been studied in 5 placebo-controlled studies, three of 12 weeks fixed-dose duration, one of 7 weeks fixed-dose duration, and a 6-month study demonstrating long-term efficacy. Pregabalin treatment in all fixed-dose studies produced a significant reduction in pain associated with fibromyalgia at doses from 300 to 600 mg/day (BID).
In the three 12-week fixed-dose studies, 40% of pregabalin-treated patients experienced a 30% or more improvement in pain score versus 28% of the patients on placebo; 23% of treated patients experienced a 50% or more improvement in pain score versus 15% of the patients on placebo.
Pregabalin produced significantly superior global assessment scores via the Patient Global Impression of Change (PGIC) in the three 12-week fixed-dose studies as compared to placebo treatment (41% patients feeling very much or much improved on pregabalin versus 29% on placebo). As measured by Fibromyalgia Impact Questionnaire (FIQ), pregabalin produced a statistically significant improvement in function versus placebo treatment in 2 out of the 3 fixed-dose studies in which it was evaluated.
Pregabalin treatment produced significant improvements in patient-reported sleep outcomes in the 4 fixed-dose studies as measured by Medical Outcomes Study Sleep Scale (MOS-SS) Sleep disturbance subscale, MOS-SS overall sleep problem index, and the daily sleep quality diary.
In the 6-month study, improvement in pain, global assessment (PGIC), function (FIQ total score) and sleep (MOS-SS Sleep disturbance subscale) were maintained for pregabalin-treated patients for a significantly longer period compared to placebo.
Pregabalin 600 mg/day showed an additional improvement in patient-reported sleep outcomes as compared to 300 and 450 mg/day; mean effects on pain, global assessment, and FIQ were similar at 450 and 600 mg/day, although the 600 mg per day dose was less well tolerated.
A 15-week, placebo-controlled trial was conducted with 107 pediatric patients with fibromyalgia, ages 12 through 17 years, at pregabalin total daily doses of 75-450 mg per day. The primary efficacy endpoint of change from baseline to Week 15 in mean pain intensity (derived from an 11 point numeric rating scale) showed numerically greater improvement for the pregabalin treated patients compared to placebo treated patients, but did not reach statistical significance. The most frequently observed adverse reactions in the clinical trial included dizziness, nausea, headache, weight increased, and fatigue. The overall safety profile in adolescents was similar to that observed in adults with fibromyalgia.
Epilepsy: Pregabalin has been studied in 3 controlled clinical studies of 12-week duration with either twice a day dosing or three times a day dosing. Overall, the safety and efficacy profiles for twice a day and three times a day dosing regimens were similar.
A reduction in seizure frequency was observed by Week 1.
Generalized anxiety disorder (GAD): Pregabalin has been studied in 6 controlled studies of 4 to 6 weeks duration, an elderly study of 8 weeks duration and a long-term relapse prevention study with a double-blind relapse prevention phase of 6 months duration.
Relief of the symptoms of GAD as reflected by the Hamilton Anxiety Rating Scale (HAM-A) was observed by Week 1.
In controlled clinical trials (4-8 weeks duration) 52% of the pregabalin treated patients and 38% of the patients on placebo had at least a 50% improvement in HAM-A total score from baseline to endpoint.
Pharmacokinetics: Pregabalin steady-state pharmacokinetics are similar in healthy volunteers, patients with epilepsy receiving anti-epileptic drugs, and patients with chronic pain.
Absorption: Pregabalin is rapidly absorbed when administered in the fasted state, with peak plasma concentrations occurring within 1 hour following both single and multiple dose administration. Pregabalin oral bioavailability is estimated to be ≥90% and is independent of dose. Following repeated administration, steady state is achieved within 24 to 48 hours. The rate of pregabalin absorption is decreased when given with food resulting in a decrease in Cmax by approximately 25-30% and a delay in tmax to approximately 2.5 hours. However, administration of pregabalin with food has no clinically significant effect on the extent of pregabalin absorption.
Distribution: In preclinical studies, pregabalin has been shown to cross the blood brain barrier in mice, rats and monkeys. Pregabalin has been shown to cross the placenta in rats and is present in the milk of lactating rats. In humans, the apparent volume of distribution of pregabalin following oral administration is approximately 0.56 L/kg. Pregabalin is not bound to plasma proteins.
Metabolism: Pregabalin undergoes negligible metabolism in humans. Following a dose of radiolabeled pregabalin, approximately 98% of the radioactivity recovered in the urine was unchanged pregabalin. The N-methylated derivative of pregabalin, the major metabolite of pregabalin found in urine, accounted for 0.9% of the dose. In preclinical studies, there was no indication of racemization of pregabalin S-enantiomer to the R-enantiomer.
Elimination: Pregabalin is eliminated from the systemic circulation primarily by renal excretion as unchanged drug.
Pregabalin mean elimination half-life is 6.3 hours. Pregabalin plasma clearance and renal clearance are directly proportional to creatinine clearance (see Pharmacokinetics in special patient groups: Renal impairment as follows).
Dosage adjustment in patients with reduced renal function or undergoing hemodialysis is necessary (see Dosage & Administration).
Linearity/Non-linearity: Pregabalin pharmacokinetics are linear over the recommended daily dose range. Inter-subject pharmacokinetic variability for pregabalin is low (<20%). Multiple dose pharmacokinetics are predictable from single-dose data. Therefore, there is no need for routine monitoring of plasma concentrations of pregabalin.
Pharmacokinetics in special patient groups: Gender: Clinical trials indicate that gender does not have a clinically significant influence on the plasma concentrations of pregabalin.
Renal impairment: Pregabalin clearance is directly proportional to creatinine clearance. In addition, pregabalin is effectively removed from plasma by hemodialysis (following a 4-hour hemodialysis treatment plasma pregabalin concentrations are reduced by approximately 50%).
Since renal elimination is the major elimination pathway, dosage reduction in patients with renal impairment and dosage supplementation following hemodialysis is necessary (see Dosage & Administration).
Hepatic impairment: No specific pharmacokinetic studies were carried out in patients with impaired liver function. Since pregabalin does not undergo significant metabolism and is excreted predominantly as unchanged drug in the urine, impaired liver function would not be expected to significantly alter pregabalin plasma concentrations.
Elderly (over 65 years of age): Pregabalin clearance tends to decrease with increasing age. This decrease in pregabalin oral clearance is consistent with decreases in creatinine clearance associated with increasing age. Reduction of pregabalin dose may be required in patients who have age related compromised renal function (see Table 1 under Dosage & Administration).
Breast-feeding: The pharmacokinetics of 150 mg pregabalin given every 12 hours (300 mg daily dose) was evaluated in 10 lactating women who were at least 12 weeks postpartum. Lactation had little to no influence on pregabalin pharmacokinetics. Pregabalin was excreted into breast milk with average steady-state concentrations approximately 76% of those in maternal plasma. The estimated average daily infant dose of pregabalin from breast milk (assuming mean milk consumption of 150 mL/kg/day) was 0.31 mg/kg/day, which on a mg/kg basis would be approximately 7% of the maternal dose.
Neuropathic pain: Pregabalin is indicated for the treatment of central and peripheral neuropathic pain in adults.
Epilepsy: Pregabalin is indicated as adjunctive therapy in adults with partial seizures with or without secondary generalization.
Generalized Anxiety Disorders (GAD): Pregabalin is indicated for the treatment of Generalized Anxiety Disorders (GAD) in adults.
Fibromyalgia: Pregabalin is indicated for the management of fibromyalgia.
LYBALIN 75 MG is formulated as a capsule for oral administration.
The dose range is 150 to 600 mg per day given in either two or three divided doses.
Pregabalin may be taken with or without food.
Neuropathic Pain: Pregabalin treatment can be started at a dose of 150 mg per day. Based on individual patient response and tolerability, the dosage may be increased to 300 mg per day after an interval of 3 to 7 days, and if needed, to a maximum dose of 600 mg per day after an additional 7-day interval.
Fibromyalgia: The usual dose range for most patients is 300 to 450 mg per day given in two divided doses. Some patients may derive additional benefit at 600 mg per day. Dosing should begin at 75 mg two times a day (150 mg/day) and may be increased to 150 mg two times a day (300 mg/day) within 1 week based on efficacy and tolerability. Patients who do not experience sufficient benefit with 300 mg/day may be further increased to 225 mg two times a day (450 mg/day). If needed, in some patients, based on individual response and tolerability, the dose may be increased to maximum dosage of 600 mg/day after an additional week.
Epilepsy: Pregabalin treatment can be started with a dose of 150 mg per day. Based on individual patient response and tolerability, the dosage may be increased to 300 mg per day after 1 week. The maximum dosage of 600 mg per day may be achieved after an additional week.
Generalized Anxiety Disorder: The dose range is 150 to 600 mg per day given as two or three divided doses. The need for treatment should be reassessed regularly.
Pregabalin treatment can be started with a dose of 150 mg per day. Based on individual patient response and tolerability, the dosage may be increased to 300 mg per day after 1 week. Following an additional week, the dosage may be increased to 450 mg per day. The maximum dosage of 600 mg per day may be achieved after an additional week.
Discontinuation of Pregabalin: If pregabalin has to be discontinued, it is recommended this should be done gradually over a minimum of 1 week.
Patients with renal impairment: Dosage reduction in patients with compromised renal function must be individualized according to creatinine clearance (CL
cr), as indicated in Table 1 determined using the following formula: (See equation.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For patients receiving hemodialysis, the pregabalin daily dose should be adjusted based on renal function. In addition to the daily dose, a supplementary dose should be given immediately following every 4-hour hemodialysis treatment (see Table 1).
Click on icon to see table/diagram/image
Use in patients with hepatic impairment: No dosage adjustment is required for patients with hepatic impairment.
Use in children and adolescents (12 to 17 years of age): The safety and effectiveness of pregabalin in pediatric patients below the age of 12 years and adolescents has not been established.
The use in children is not recommended.
Use in the elderly (over 65 years of age): Elderly patients may require a dose reduction of pregabalin due to decreased renal function.
In overdoses up to 15 g, no unexpected adverse reactions were reported.
In the post-marketing experience, the most commonly reported adverse events observed when pregabalin was taken in overdose included affective disorder, somnolence, confusional state, depression, agitation and restlessness. Seizures were also reported.
Treatment of pregabalin overdose should include general supportive measures and may include hemodialysis if necessary.
Hypersensitivity to pregabalin or any of its components.
Angioedema: Specific symptoms included swelling of the face, mouth (gums, lips, and tongue), and neck (larynx and throat). Discontinue pregabalin immediately in patients with these symptoms. Exercise caution when prescribing pregabalin to patients who have had a previous episode of angioedema. In addition, patients who are taking other drugs associated with angioedema, such as angiotensin converting enzyme inhibitors (ACE-inhibitors), may be at increased risk of developing angioedema.
Hypersensitivity Reactions: Adverse reactions included blisters, dyspnea, hives, rash, skin redness, and wheezing. Discontinue pregabalin immediately in patients with these symptoms.
Increased Risk of Adverse Reactions with Abrupt or Rapid Discontinuation: As with all antiepileptic drugs (AEDs), withdraw pregabalin gradually to minimize the potential of increased seizure frequency in patients with seizure disorders.
Following abrupt or rapid discontinuation of pregabalin, some patients reported symptoms including insomnia, nausea, headache, anxiety, hyperhidrosis, and diarrhea.
If pregabalin is discontinued, taper the drug gradually over a minimum of 1 week rather than discontinue the drug abruptly.
Suicidal Behavior and Ideation: Antiepileptic drugs (AEDs), including pregabalin, increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Monitor patients treated with any AED for any indication for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior.
Anyone considering prescribing pregabalin or any other AED must balance the risk of suicidal thoughts or behavior with the risk of untreated illness. Epilepsy and many other illnesses for which AEDs are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behavior. Should suicidal thoughts and behavior emerge during treatment, the prescriber needs to consider whether the emergence of these symptoms in any given patient may be related to the illness being treated.
Peripheral Edema: Pregabalin may cause peripheral edema.
As the thiazolidinedione class of antidiabetic drugs can cause weight gain and/or fluid retention, possibly exacerbating or leading to heart failure, exercise caution when co-administering pregabalin and these agents.
Dizziness/Somnolence: Pregabalin may cause dizziness and somnolence. Inform patients that pregabalin-related dizziness and somnolence may impair their ability to perform tasks such as driving or operating machinery.
Weight Gain: Pregabalin treatment may cause weight gain. Pregabalin-associated weight gain was related to dose and duration of exposure but did not appear to be associated with baseline body mass index, gender, or age. Weight gain was not limited to patients with edema.
Ophthalmic Effects: Inform patients to notify their healthcare provider if changes in vision occur. If visual disturbance persists, consider further assessment. Consider more frequent assessments for patients who are already routinely monitored for ocular conditions.
Creatine Kinase Elevations: Pregabalin treatment was associated with creatine kinase elevations. Instruct patients to promptly report unexplained symptoms of muscle pain, tenderness, or weakness. Particularly if these muscle symptoms are accompanied by malaise or fever. Discontinue pregabalin treatment if myopathy is diagnosed or suspected or if markedly elevated creatine kinase levels occur.
Decreased Platelet Count: Pregabalin treatment was associated with a decrease in platelet count.
PR Interval Prolongation: Pregabalin treatment was associated with PR interval prolongation.
Effect On Ability To Drive And Use Machines: Pregabalin may cause dizziness and somnolence, and therefore may influence the ability to drive or use machines. Patients are advised not to drive, operate complex machinery or engage in other potentially hazardous activities until it is known whether this medication affects their ability to perform these activities.
Pregnancy: There is a limited amount of data on the use of pregabalin in pregnant women.
Birth and postnatal neurodevelopmental outcomes: There were no statistically significant findings for stillbirth, low birth weight, preterm birth, small for gestational age, low Apgar score, and microcephaly.
In pediatric population, no evidence of an increased risk for attention deficit hyperactivity disorder (ADHD), autism spectrum disorders (ASD), and intellectual disabilities.
Pregabalin should not be used during pregnancy unless the benefit to the mother clearly outweighs the potential risk to the fetus. Effective contraception must be used in women of childbearing potential.
Lactation: Pregabalin is excreted in the milk of lactating women. As the safety of pregabalin in infants is not known, breast-feeding is not recommended during treatment with pregabalin. A decision must be made whether to discontinue breast-feeding or to discontinue from pregabalin therapy taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman.
The most commonly reported adverse reactions were dizziness and somnolence. Adverse reactions were usually mild to moderate in intensity.
Selected adverse drug reactions are listed in the table as follows by System Organ Class (SOC). The adverse reactions listed may also be associated with the underlying disease and/or concomitant medications. (See Table 2.)
Click on icon to see table/diagram/image
The following adverse drug reactions were reported during Post-Marketing Surveillance:
Immune system disorders: Uncommon: Hypersensitivity; Rare: Angioedema, allergic reaction.
Nervous system disorders: Very Common: Headache; Uncommon: Loss of consciousness, mental impairment.
Eye disorders: Rare: Keratitis.
Cardiac disorders: Rare: Congestive heart failure.
Respiratory, thoracic and mediastinal disorders: Rare: Pulmonary oedema.
Gastrointestinal disorders: Common: Nausea, diarrhoea; Rare: Swollen tongue.
Skin and subcutaneous tissue disorders: Uncommon: Face swelling, pruritus.
Renal and urinary disorders: Rare: Urinary retention.
Reproductive system and breast disorders: Rare: Gynaecomastia.
General disorders and administration site conditions: Uncommon: Malaise.
Since pregabalin is predominantly excreted unchanged in the urine, undergoes negligible metabolism in humans, does not inhibit drug metabolism in vitro, and is not bound to plasma proteins, it is unlikely to produce, or be subject to, pharmacokinetic interactions.
Co-administration of pregabalin with the oral contraceptives norethisterone and/or ethinyl estradiol does not influence the steady-state pharmacokinetics of either substance. Pregabalin may potentiate the effects of ethanol and lorazepam. Pregabalin appears to be additive in the impairment of cognitive and gross motor function caused by oxycodone.
In the post-marketing experience, there are reports of respiratory failure, coma and deaths in patients taking pregabalin and other CNS depressant medications including in patients who are substance abusers. There are post-marketing reports of events related to reduced lower gastrointestinal tract function (e.g., intestinal obstruction, paralytic ileus, constipation) when pregabalin was co-administered with medications that have the potential to produce constipation, such as opioid analgesics.
N02BF02 - pregabalin ; Belongs to the class of gabapentinoids. Used to relieve pain and other conditions.
Lybalin hard cap 75 mg
8 × 7's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image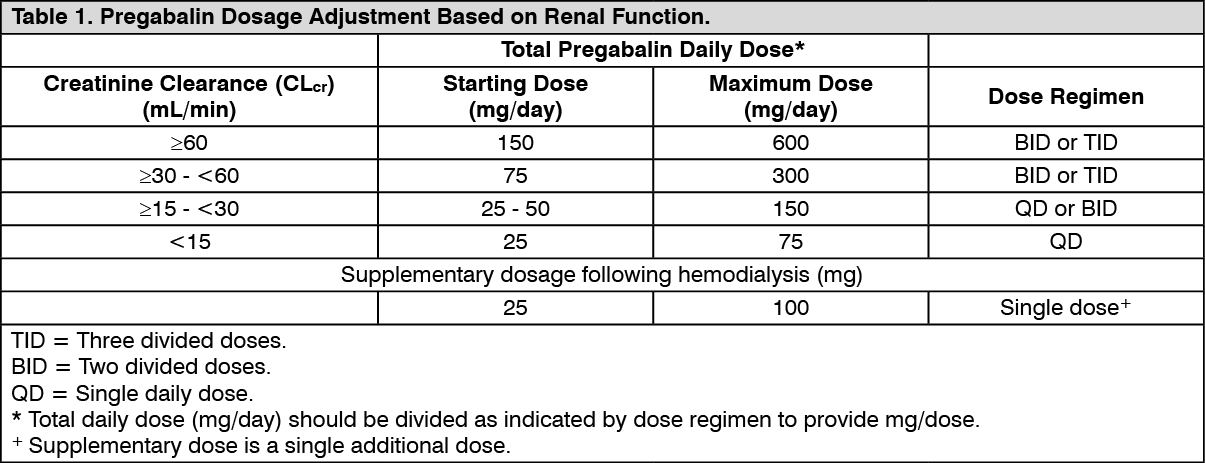 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image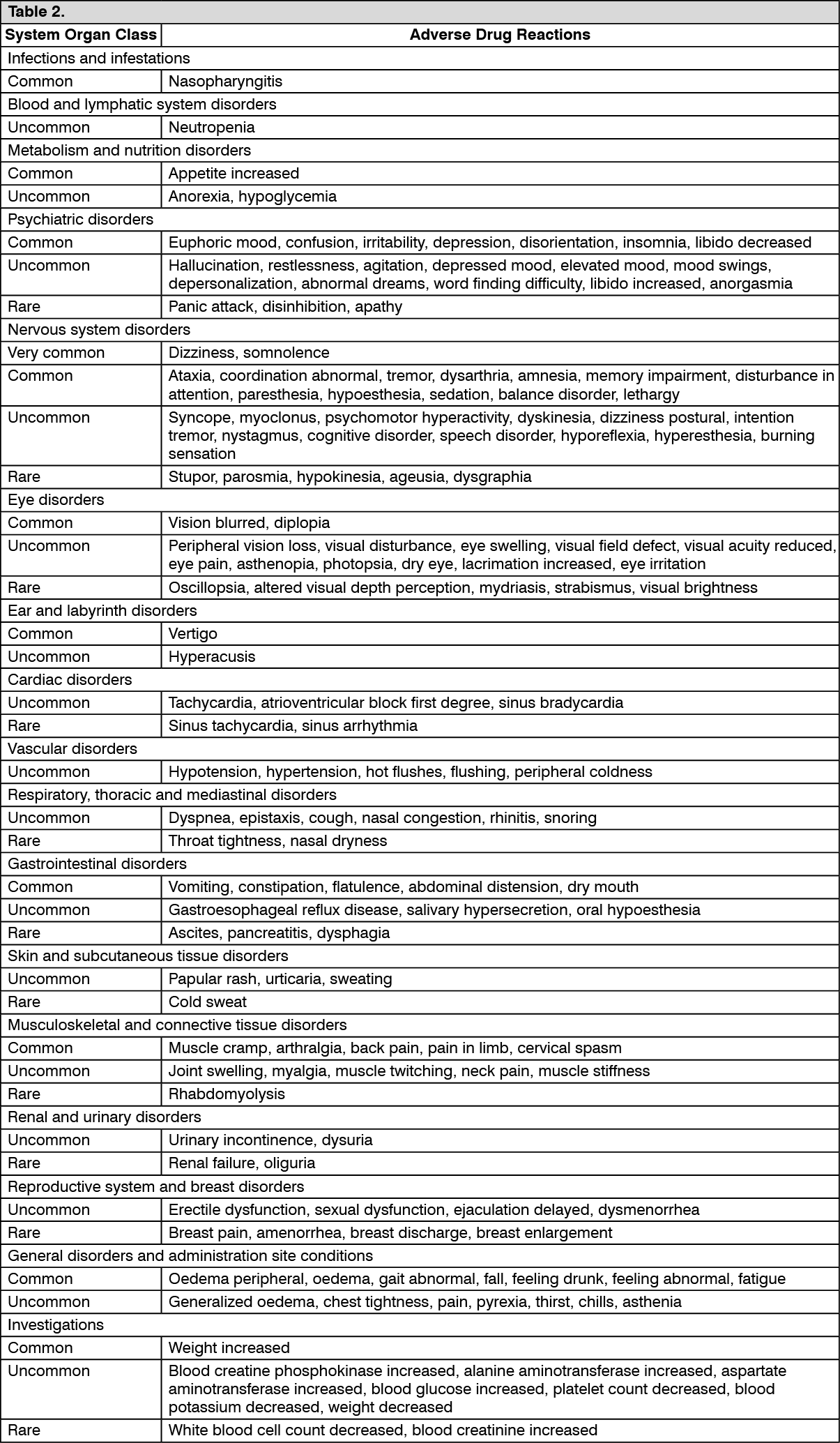 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out