


 Sign Out
Sign Out



Exercise caution when prescribing pregabalin to patients who have had a previous episode of angioedema. In addition, patients who are taking other drugs associated with angioedema (e.g., angiotensin converting enzyme inhibitors [ACE-inhibitors]) may be at increased risk of developing angioedema.
Hypersensitivity: There have been post-marketing reports of hypersensitivity in patients shortly after initiation of treatment with pregabalin. Adverse reactions included skin redness, blisters, hives, rash, dyspnea, and wheezing. Discontinue pregabalin immediately in patients with these symptoms.
Suicidal Behavior and Ideation: Antiepileptic drugs (AEDs), including pregabalin, increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Monitor patients treated with any AED for any indication for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior.
Pooled analyses of 199 placebo-controlled clinical trials (mono- and adjunctive therapy) of 11 different AEDs showed that patients randomized to one of the AEDs had approximately twice the risk (adjusted Relative Risk 1.8, 95% CI:1.2, 2.7) of suicidal thinking or behavior compared to patients randomized to placebo. In these trials, which had a median treatment duration of 12 weeks, the estimated incidence rate of suicidal behavior or ideation among 27,863 AED-treated patients was 0.43%, compared to 0.24% among 16,029 placebo-treated patients, representing an increase of approximately one case of suicidal thinking or behavior for every 530 patients treated. There were four suicides in drug-treated patients in the trials and none in placebo-treated patients, but the number is too small to allow any conclusion about drug effect on suicide.
The increased risk of suicidal thoughts or behavior with AEDs was observed as early as one week after starting drug treatment with AEDs and persisted for the duration of treatment assessed. Because most trials included in the analysis did not extend beyond 24 weeks, the risk of suicidal thoughts or behavior beyond 24 weeks could not be assessed.
The risk of suicidal thoughts or behavior was generally consistent among drugs in the data analyzed. The finding of increased risk with AEDs of varying mechanisms of action and across a range of indications suggests that the risk applies to all AEDs used for any indication. The risk did not vary substantially by age (5-100 years) in the clinical trials analyzed.
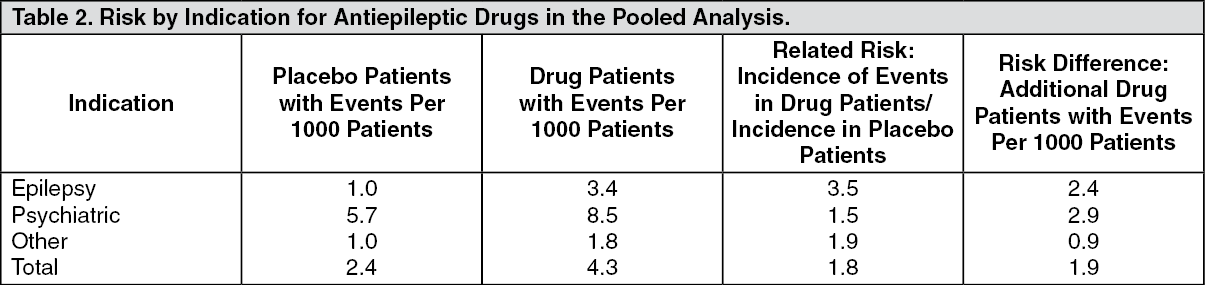
Table 2 shows absolute and relative risk by indication for all evaluated AEDs. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe relative risk for suicidal thoughts or behavior was higher in clinical trials for epilepsy than in clinical trials for psychiatric or other conditions, but the absolute risk differences were similar for the epilepsy and psychiatric indications.
Anyone considering prescribing pregabalin or any other AED must balance the risk of suicidal thoughts or behavior with the risk of untreated illness. Epilepsy and many other illnesses for which AEDs are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behavior. Should suicidal thoughts and behavior emerge during treatment, the prescriber needs to consider whether the emergence of these symptoms in any given patient may be related to the illness being treated.
Respiratory Depression: There is evidence from case reports, human studies, and animal studies associating pregabalin with serious, life-threatening, or fatal respiratory depression when co-administered with central nervous system (CNS) depressants, including opioids, or in the setting of underlying respiratory impairment. When the decision is made to co-prescribe pregabalin with another CNS depressant, particularly an opioid, or to prescribe pregabalin to patients with underlying respiratory impairment, monitor patients for symptoms of respiratory depression and sedation, and consider initiating pregabalin at a low dose. The management of respiratory depression may include close observation, supportive measures, and reduction or withdrawal of CNS depressants (including pregabalin).
There is more limited evidence from case reports, animal studies, and human studies associating pregabalin with serious respiratory depression, without co-administered CNS depressants or without underlying respiratory impairment.
Dizziness and Somnolence: Pregabalin may cause dizziness and somnolence. Inform patients that pregabalin-related dizziness and somnolence may impair their ability to perform tasks such as driving or operating machinery and could increase the occurrence of accidental injury (fall) in the elderly population.
In the pregabalin controlled trials in adult patients, dizziness was experienced by 30% of pregabalin-treated patients compared to 8% of placebo-treated patients; somnolence was experienced by 23% of pregabalin-treated patients compared to 8% of placebo-treated patients. Dizziness and somnolence generally began shortly after the initiation of pregabalin therapy and occurred more frequently at higher doses. Dizziness and somnolence were the adverse reactions most frequently leading to withdrawal (4% each) from controlled studies. In pregabalin-treated patients reporting these adverse reactions in short-term, controlled studies, dizziness persisted until the last dose in 30% and somnolence persisted until the last dose in 42% of patients (see Interactions).
There have also been post-marketing reports of loss of consciousness, confusion and mental impairment. Therefore, patients should be advised to exercise caution until they are familiar with the potential effects of the medication.
Pregabalin is not known to be active at receptor sites associated with drugs of abuse. Cases of misuse, abuse and dependence have been reported in the post-marketing database. As with any CNS active drug, carefully evaluate patients for history of drug abuse and/or psychiatric disorders. Patients should be observed for signs of pregabalin misuse, abuse or dependence (e.g. development of tolerance, dose escalation, drug-seeking behavior).
Increased Risk of Adverse Reactions with Abrupt or Rapid Discontinuation: As with all antiepileptic drugs (AEDs), withdraw pregabalin gradually to minimize the potential of increased seizure frequency in patients with seizure disorders.
Following abrupt or rapid discontinuation of LYRICA, some patients reported symptoms including insomnia, nausea, headache, anxiety, hyperhidrosis, and diarrhea.
If LYRICA is discontinued, taper the drug gradually over a minimum of 1 week rather than discontinue the drug abruptly.
Peripheral Edema: Pregabalin treatment may cause peripheral edema. In short-term trials of patients without clinically significant heart or peripheral vascular disease, there was no apparent association between peripheral edema and cardiovascular complications such as hypertension or congestive heart failure. Peripheral edema was not associated with laboratory changes suggestive of deterioration in renal or hepatic function.
In controlled clinical trials in adult patients, the incidence of peripheral edema was 6% in the pregabalin group compared with 2% in the placebo group. In controlled clinical trials, 0.5% of pregabalin patients and 0.2% placebo patients withdrew due to peripheral edema.
Higher frequencies of weight gain and peripheral edema were observed in patients taking both pregabalin and a thiazolidinedione antidiabetic agent compared to patients taking either drug alone. The majority of patients using thiazolidinedione antidiabetic agents in the overall safety database were participants in studies of pain associated with diabetic peripheral neuropathy. In this population, peripheral edema was reported in 3% (2/60) of patients who were using thiazolidinedione antidiabetic agents only, 8% (69/859) of patients who were treated with pregabalin only, and 19% (23/120) of patients who were on both pregabalin and thiazolidinedione antidiabetic agents. Similarly, weight gain was reported in 0% (0/60) of patients on thiazolidinediones only; 4% (35/859) of patients on pregabalin only; and 7.5% (9/120) of patients on both drugs.
As the thiazolidinedione class of antidiabetic drugs can cause weight gain and/or fluid retention, possibly exacerbating or leading to heart failure, exercise caution when co-administering pregabalin and these agents.
Although there has been no causal relationship identified between exposure to pregabalin and congestive heart failure, there has been post-marketing reports of congestive heart failure in some patients receiving pregabalin. In short-term trials of patients without clinically significant heart or peripheral vascular disease, there was no apparent association between peripheral edema and cardiovascular complications such as hypertension or congestive heart failure.
Because there are limited data on congestive heart failure patients with New York Heart Association (NYHA) Class III or IV cardiac status, exercise caution when using pregabalin in these patients.
Weight Gain: Pregabalin treatment may cause weight gain. In pregabalin controlled clinical trials in adult patients of up to 14 weeks, a gain of 7% or more over baseline weight was observed in 9% of pregabalin-treated patients and 2% of placebo-treated patients. Few patients treated with pregabalin (0.3%) withdrew from controlled trials due to weight gain. Pregabalin-associated weight gain was related to dose and duration of exposure but did not appear to be associated with baseline BMI, gender, or age. Weight gain was not limited to patients with edema.
Although weight gain was not associated with clinically important changes in blood pressure in short-term controlled studies, the long-term cardiovascular effects of pregabalin-associated weight gain are unknown.
Among diabetic patients, pregabalin-treated patients gained an average of 1.6 kg (range: -16 to 16 kg), compared to an average 0.3 kg (range: -10 to 9 kg) weight gain in placebo patients. In a cohort of 333 diabetic patients who received pregabalin for at least 2 years, the average weight gain was 5.2 kg.
While the effects of pregabalin-associated weight gain on glycemic control have not been systematically assessed, in controlled and longer-term open label clinical trials with diabetic patients, pregabalin treatment did not appear to be associated with loss of glycemic control (as measured by HbA1C).
Some diabetic patients who gain weight on pregabalin treatment may need to adjust hypoglycemic medications.
Abrupt or Rapid Discontinuation: Following abrupt or rapid discontinuation of short-term and long-term treatment with pregabalin, withdrawal symptoms have been observed in some patients. The following events have been mentioned: insomnia, headache, nausea, anxiety, diarrhoea, flu syndrome, nervousness, depression, pain, convulsion, hyperhidrosis and dizziness suggestive of physical dependence. The patient should be informed about this at the start of the treatment.
Convulsions, including status epilepticus and grand mal convulsions, may occur during pregabalin use or shortly after discontinuing pregabalin.
Concerning discontinuation of long-term treatment of pregabalin, data suggest that the incidence and severity of withdrawal symptoms may be dose-related.
There are insufficient data for the withdrawal of concomitant antiepileptic medicinal products, once seizure control with pregabalin in the add-on situation has been reached, in order to reach monotherapy on pregabalin.
Tumorigenic Potential: In standard preclinical in vivo lifetime carcinogenicity studies of pregabalin, an unexpectedly high incidence of hemangiosarcoma was identified in two different strains of mice. The clinical significance of this finding is unknown. Clinical experience during pregabalin's pre-marketing development provides no direct means to assess its potential for inducing tumors in humans.
In clinical studies across various patient populations, comprising 6396 patient-years of exposure in patients greater than 12 years of age, new- or worsening pre-existing tumors were reported in 57 patients. Without knowledge of the background incidence and recurrence in similar populations not treated with pregabalin, it is impossible to know whether the incidence seen in these cohorts is or is not affected by treatment.
Ophthalmological Effects: In controlled studies in adult patients, a higher proportion of patients treated with pregabalin reported blurred vision (7%) than did patients treated with placebo (2%), which resolved in a majority of cases with continued dosing. Less than 1% of patients discontinued pregabalin treatment due to vision-related events (primarily blurred vision).
Prospectively planned ophthalmologic testing, including visual acuity testing, formal visual field testing and dilated funduscopic examination, was performed in over 3600 patients. In these patients, visual acuity was reduced in 7% of patients treated with pregabalin, and 5% of placebo-treated patients. Visual field changes were detected in 13% of pregabalin-treated, and 12% of placebo-treated patients. Funduscopic changes were observed in 2% of pregabalin-treated and 2% of placebo-treated patients.
Although the clinical significance of the ophthalmologic findings is unknown, inform patients to notify their physician if changes in vision occur. If visual disturbance persists, consider further assessment. Consider more frequent assessments for patients who are already routinely monitored for ocular conditions.
In the post-marketing experience, visual adverse reactions have also been reported, including loss of vision, visual blurring or other changes of visual acuity, many of which were transient. Discontinuation of pregabalin may result in resolution or improvement of these visual symptoms.
Creatine Kinase Elevations: Pregabalin treatment was associated with creatine kinase elevations. Mean changes in creatine kinase from baseline to the maximum value were 60 U/L for pregabalin-treated patients and 28 U/L for the placebo patients. In all controlled trials in adult patients across multiple patient populations, 1.5% of patients on pregabalin and 0.7% of placebo patients had a value of creatine kinase at least three times the upper limit of normal. Three pregabalin-treated subjects had events reported as rhabdomyolysis in premarketing clinical trials. The relationship between these myopathy events and pregabalin is not completely understood because the cases had documented factors that may have caused or contributed to these events. Instruct patients to promptly report unexplained muscle pain, tenderness, or weakness, particularly if these muscle symptoms are accompanied by malaise or fever. Discontinue treatment with pregabalin if myopathy is diagnosed or suspected or if markedly elevated creatine kinase levels occur.
Decreased Platelet Count: Pregabalin treatment was associated with a decrease in platelet count. Pregabalin-treated subjects experienced a mean maximal decrease in platelet count of 20 x 103/μL, compared to 11 x 103/μL in placebo patients. In the overall database of controlled trials in adult patients, 2% of placebo patients and 3% of pregabalin patients experienced a potentially clinically significant decrease in platelets, defined as 20% below baseline value and less than 150 x 103/µL. A single pregabalin-treated subject developed severe thrombocytopenia with a platelet count less than 20 x 103/μL. In randomized controlled trials, pregabalin was not associated with an increase in bleeding-related adverse reactions.
PR Interval Prolongation: Pregabalin treatment was associated with PR interval prolongation. In analyses of clinical trial ECG data in adult patients, the mean PR interval increase was 3-6 msec at pregabalin doses greater than or equal to 300 mg/day. This mean change difference was not associated with an increased risk of PR increase greater than or equal to 25% from baseline, an increased percentage of subjects with on-treatment PR greater than 200 msec, or an increased risk of adverse reactions of second- or third-degree AV block.
Subgroup analyses did not identify an increased risk of PR prolongation in patients with baseline PR prolongation or in patients taking other PR prolonging medications. However, these analyses cannot be considered definitive because of the limited number of patients in these categories.
Women of childbearing potential/Contraception: Pregabalin use in the first trimester of pregnancy may cause major birth defects in the unborn child. Pregabalin should not be used during pregnancy unless the benefit to the mother clearly outweighs the potential risk to the fetus. Women of childbearing potential must use effective contraception during treatment (see Use in Pregnancy & Lactation).
Others: Although the effects of discontinuation on the reversibility of renal failure have not been systematically studied, improved renal failure following discontinuation or dose reduction of pregabalin has been reported.
Misuse, abuse potential or dependence: Cases of misuse, abuse and dependence have been reported. Caution should be exercised in patients with a history of substance abuse and the patient should be monitored for symptoms of pregabalin misuse, abuse or dependence (development of tolerance, dose escalation, drug seeking behaviour have been reported).
Encephalopathy: Cases of encephalopathy have been reported, mostly in patients with underlying conditions that may precipitate encephalopathy.
Lactose intolerance: Pregabalin contains lactose monohydrate. Patients with rare hereditary problems of galactose intolerance, the Lapp-lactase deficiency or glucose-galactose malabsorption should not take this medicinal product.
Treatment of central neuropathic pain due to spinal cord injury: In the treatment of central neuropathic pain due to spinal cord injury the incidence of adverse reactions in general, central nervous system adverse reactions and especially somnolence was increased. This may be attributed to an additive effect due to concomitant medicinal products (e.g., anti-spasticity agents) needed for this condition. This should be considered when prescribing pregabalin in this condition.
Effects on ability to drive and use machines: Pregabalin may cause dizziness and somnolence and therefore may influence the ability to drive or use machines. Patients are advised not to drive, operate complex machinery or engage in other potentially hazardous activities until it is known whether this medication affects their ability to perform these activities.