Zoledronic Acid Injection must only be prescribed and administered to patients by healthcare professionals experienced in the administration of intravenous bisphosphonates.
Posology: Prevention of skeletal related events in patients with advanced malignancies involving bone: Adults and elderly: The recommended dose in the prevention of skeletal related events in patients with advanced malignancies involving bone is 4 mg zoledronic acid every 3 to 4 weeks.
Patients should also be administered an oral calcium supplement of 500 mg and 400 IU vitamin D daily.
The decision to treat patients with bone metastases for the prevention of skeletal related events should consider that the onset of treatment effect is 2-3 months.
Treatment of Tumour-Induced Hypercalcaemia (TIH): Adults and elderly: The recommended dose in hypercalcaemia (albumin-corrected serum calcium ≥ 12.0 mg/dL or 3.0 mmol/L) is a single dose of 4 mg zoledronic acid.
Renal impairment: Tumour-Induced Hypercalcaemia (TIH): Zoledronic acid treatment in patients with Tumour-Induced Hypercalcaemia (TIH) and who have severe renal impairment should be considered only after evaluating the risks and benefit of treatment. No dose adjustment is necessary in TIH patients with serum creatinine < 400 micromol/L or <4.5 mg/dL.
Prevention of skeletal related events in patients with advanced malignancies involving bone: When initiating treatment with OLEDRON in patients with multiple myeloma or metastatic bone lesions from solid tumours, serum creatinine and creatinine clearance (Cl
Cr) should be determined. Cl
Cr is calculated from serum creatinine levels using the Cockcroft-Gault formula. OLEDRON is not recommended for patients presenting with severe renal impairment prior to initiation of therapy, which is defined for this population as Cl
Cr < 30 mL/min.
For patients with normal renal function (defined as Cl
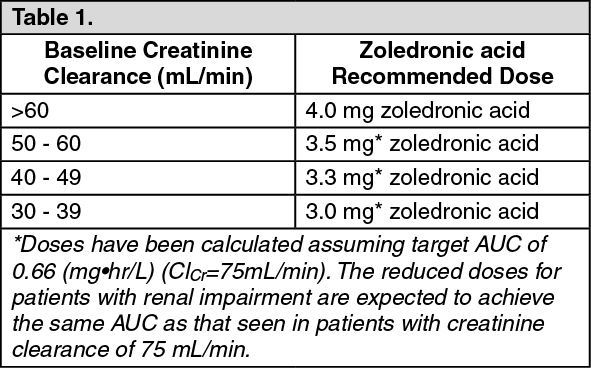
Cr > 60 ml/min), zoledronic acid 4 mg/100 ml solution for infusion may be administered directly without any further preparation. In patients with bone metastases presenting with mild to moderate renal impairment prior to initiation of therapy, which is defined for this population as Cl
Cr 30 to 60 mL/min, the following OLEDRON dose is recommended: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Following initiation of therapy, serum creatinine should be measured prior to each dose of OLEDRON and treatment should be withheld if renal function has deteriorated. Renal deterioration was defined as follows: For patients with normal baseline serum creatinine (<1.4 mg/dl or <124 μmol/l), an increase of 0.5mg/dl or 44 μmol/l; For patients with abnormal baseline creatinine (> 1.4 mg/dl or >124 μmol/l), an increase of 1.0 mg/dl or 88 μmol/l.
Zoledronic acid should be resumed at the same dose as that prior to treatment interruption.
Pediatric population: The safety and efficacy of zoledronic acid in children aged 1 year to 17 years have not been established.
Method of Administration: OLEDRON 4 mg/5 mL concentrate for solution for infusion is for intravenous use only. Oledron 4mg concentrate for solution for infusion, further diluted in 100ml (see Instruction for Use and Handling under Cautions for Usage), should be given as a single intravenous infusion in no less than 15 minutes.
In patients with mild to moderate renal impairment, reduced OLEDRON doses are recommended.
Instructions for preparing reduced doses of OLEDRON: Withdraw an appropriate volume of the concentrate needed, as follows: See Table 2.
Click on icon to see table/diagram/image
For instructions on the dilution of the medicinal product before administration, see Instruction for Use and Handling under Cautions for Usage.
Route of Administration: Intravenous Infusion.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image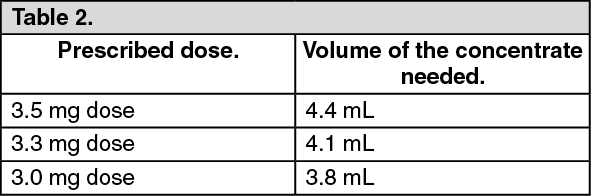 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out