Tablet: VENTOLIN Tablets 2 mg each contain 2 mg salbutamol, as sulphate, respectively.
Syrup: Each 5 ml contains 2 mg Salbutamol (as Salbutamol Sulphate).
Excipient with known effect: Sodium.
Evohaler: VENTOLIN EVOHALER is a pressurised metered-dose inhaler which delivers 100 micrograms salbutamol (as sulphate) per actuation, into the mouthpiece of a specially designed actuator. The inhaler also contains the CFC-free propellant HFA 134a. Each canister contains at least 200 actuations.
Respirator Solution: VENTOLIN Respirator Solution contains 5 mg salbutamol, as sulphate, per ml of solution and is supplied in 10 ml bottles.
Nebule: Each nebule contains 2.5 ml of solution equivalent to 2.5 mg salbutamol.
VENTOLIN nebules are plastic ampoules containing a solution of salbutamol sulphate in normal saline.
Infusion: VENTOLIN Solution for Intravenous Infusion 5 mg salbutamol, as sulphate, in 5 ml (1 mg/ml).
Excipients/Inactive Ingredients: Tablet: Lactose monohydrate, maize starch, pregelatinised starch, magnesium stearate.
Syrup: Sodium citrate dihydrate, Citric acid monohydrate, Hydroxypropyl methylcellulose, Sodium benzoate, Saccharin sodium, Orange flavour, Sodium chloride, Purified water.
Evohaler: 1,1,1,2-tetrafluoroethane (also known as HFA 134a or norflurane).
Respirator Solution: Purified water, Benzalkonium chloride, Dilute sulphuric acid.
Nebule: Sodium chloride, Sulphuric acid, Purified water.
Infusion: Dilute sulphuric acid or sodium hydroxide for pH adjustment, Nitrogen, Sodium Chloride, Water for Injections.
Pharmacotherapeutic group: Selective beta2-adrenoceptor agonists. ATC Code: R03CC02.
Pharmacology: Pharmacodynamics: Salbutamol is a selective beta2-adrenoreceptor agonist. At therapeutic doses, it acts on the beta2-adrenoreceptors of bronchial muscle providing short-acting (4 to 6 hours) bronchodilation in reversible airways obstruction.
Clinical Studies: Evohaler: Special Patient Populations: Children <4 years of age: Paediatric clinical studies conducted at the recommended dose (SB020001, SB030001, SB030002), in patients <4 years with bronchospasm associated with reversible obstructive airways disease, show that the Evohaler has a safety profile comparable to that in children ≥4 years, adolescents and adults.
Pharmacokinetics: Tablet/Syrup/Infusion: Salbutamol administered intravenously has a half-life of 4 to 6 hours and is cleared partly renally and partly by metabolism to the inactive 4'-O-sulphate (phenolic sulphate) which is also excreted primarily in the urine. The faeces are a minor route of excretion. The majority of a dose of salbutamol given intravenously, orally or by inhalation is excreted within 72 hours. Salbutamol is bound to plasma proteins to the extent of 10%.
Tablet/Syrup: After oral administration, salbutamol is absorbed from the gastrointestinal tract and undergoes considerable first-pass metabolism to the phenolic sulphate. Both unchanged drug and conjugate are excreted primarily in the urine. The bioavailability of orally administered salbutamol is about 50%.
Evohaler/Respirator Solution/Nebule: Absorption: After administration by the inhaled route, between 10 and 20% of the dose reaches the lower airways. The remainder is retained in the delivery system or is deposited in the oropharynx from where it is swallowed. The fraction deposited in the airways is absorbed into the pulmonary tissues and circulation but is not metabolised by the lung.
Distribution: Salbutamol is bound to plasma proteins to the extent of 10%.
Metabolism: On reaching the systemic circulation, salbutamol becomes accessible to hepatic metabolism and is excreted, primarily in the urine, as unchanged drug and as the phenolic sulphate.
The swallowed portion of an inhaled dose is absorbed from the gastrointestinal tract and undergoes considerable first-pass metabolism to the phenolic sulphate. Both unchanged drug and conjugate are excreted primarily in the urine.
Elimination: Salbutamol administered intravenously has a half-life of 4 to 6 hours and is cleared partly renally and partly by metabolism to the inactive 4'-O-sulphate (phenolic sulphate) which is also excreted primarily in the urine. The faeces are a minor route of excretion. The majority of a dose of salbutamol given intravenously, orally or by inhalation is excreted within 72 hours.
Toxicology: Preclinical Safety Data: In common with other potent selective beta2-receptor agonists, salbutamol has been shown to be teratogenic in mice when given subcutaneously. In a reproductive study, 9.3% of the foetuses were found to have cleft palate, at 2.5 mg/kg, 4 times the maximum human oral dose. In rats, treatment at the levels of 0.5, 2.32, 10.75 and 50 mg/kg/day orally throughout pregnancy resulted in no significant foetal abnormalities. The only toxic effect was an increase in neonatal mortality at the highest dose level as the result of lack of maternal care. A reproductive study in rabbits revealed cranial malformations in 37% of foetuses at 50 mg/kg/day, 78 times the maximum human oral dose.
In an oral fertility and general reproductive performance study in rats at doses of 2 and 50 mg/kg/day, with the exception of a reduction in number of weanlings surviving to day 21 postpartum at 50 mg/kg/day, there were no adverse reactions on fertility, embryofetal development, litter size, birth weight or growth rate.
Syrup: Reproductive studies in the rabbit at doses of 50 mg/kg/day orally (i.e much higher than the normal human dose) have shown foetuses with treatment related changes; these included open eyelids (ablepharia), secondary palate clefts (palatoschisis), changes in ossification of the frontal bones of the cranium (cranioschisis) and limb flexure.
Evohaler: HFA 134a has been shown to be nontoxic at very high vapour concentrations, far in excess of those likely to be experienced by patients, in a wide range of animal species exposed daily for periods of two years.
Tablet: Relief of bronchial asthma of all types, chronic bronchitis and emphysema.
Syrup: Relief of bronchospasm in bronchial asthma of all types, chronic bronchitis and emphysema.
Ventolin syrup is suitable oral therapy for children and adults who are unable to use an inhaler device.
Evohaler: VENTOLIN Evohaler provides short-acting (4 to 6 hours) bronchodilation with fast onset (within 5 minutes) in reversible airway obstruction.
It is particularly suitable for the relief and prevention of asthma symptoms. VENTOLIN Evohaler should be used to relieve symptoms when they occur, and to prevent them in those circumstances, recognised by the patient to precipitate an asthma attack (e.g. before exercise or unavoidable allergen exposure).
VENTOLIN Evohaler is particularly valuable as relief medication in mild, moderate or severe asthma, provided that reliance on it does not delay the introduction and use of regular inhaled corticosteroid therapy.
Respirator Solution: VENTOLIN Respirator Solution is indicated for the treatment of of acute severe asthma (status asthmaticus) and for routine management of chronic bronchospasm-unresponsive to conventional therapy.
Nebule: Salbutamol is a selective beta2-adrenoceptor agonist. At therapeutic doses, it acts on the beta2-adrenoceptors of bronchial muscle, with little or no action on the heart. With its fast onset of action, it is particularly suitable for the management and prevention of attack in asthma.
Routine management of chronic bronchospasm - unresponsive to conventional therapy.
Treatment of acute severe asthma (status asthmaticus).
Nebule/Infusion: Bronchodilators should not be the only or the main treatment in patients with severe or unstable asthma. Severe asthma requires regular medical assessment as death may occur. Patients with severe asthma have constant symptoms and frequent exacerbations, with limited physical capacity, and PEF values below 60% predicted at baseline with greater than 30% variability, usually not returning entirely to normal after a bronchodilator. These patients will require high dose inhaled (e.g. >1 mg/day beclomethasone dipropionate) or oral corticosteroid therapy. Sudden worsening of symptoms may require increased corticosteroid dosage which should be administered under urgent medical supervision.
Infusion: VENTOLIN is a selective β2-adrenoceptor agonist. At therapeutic doses it acts on the β2-adrenoceptors in the bronchi and uterus, with little or no actions on the β1-adrenoceptors of the heart. It is suitable for the management of an asthmatic attack, and for uncomplicated premature labour, under the direction of a physician.
Relief of severe bronchospasm associated with asthma or bronchitis and for the treatment of status asthmaticus.
Management of uncomplicated premature labour in the last trimester of pregnancy.
Tablet/Evohaler/Respirator Solution/Nebule/Infusion: VENTOLIN has a duration of action of 4 to 6 hours in most patients.
Increasing use of beta2-agonists may be a sign of worsening asthma. Under these conditions, a reassessment of the patient's therapy plan may be required and concomitant glucocorticosteroid therapy should be considered.
Tablet/Evohaler/Respirator Solution/Nebule: As there may be adverse effects associated with excessive dosing, the dosage or frequency of administration should only be increased on medical advice.
Tablet: Adults: The usual effective dose is 4 milligrams 3 or 4 times per day.
If adequate bronchodilation is not obtained each single dose may be gradually increased to as much as 8 milligrams.
Some patients obtain adequate relief with 2 milligrams 3 or 4 times daily.
Children: 2 - 6 years: 1 to 2 mg 3 or 4 times daily. If a dose of 1 mg is required, the use of salbutamol syrup should be considered.
6 - 12 years: 2 mg (1 tablet of 2 milligrams) 3 or 4 times daily.
Over 12 years: 2 to 4 milligrams (1 tablet of 2 milligrams or 1 tablet of 4 milligrams) 3 or 4 times daily.
Special patient groups: In elderly patients or in those known to be unusually sensitive to beta-adrenergic stimulant drugs, it is advisable to initiate treatment with 2 milligrams salbutamol 3 or 4 times per day.
Syrup: Route of administration: oral.
Adults: The minimum starting dose is: 2 mg three times a day given as 5 ml syrup. The usual effective dose is 4 mg (10 ml syrup) three or four times a day, which may be increased to a maximum of 8 mg (20 ml syrup) three or four times a day if adequate bronchodilation is not obtained.
Elderly: In elderly patients or in those known to be unusually sensitive to beta-adrenergic stimulant drugs, it is advisable to initiate treatment with the minimum starting dose.
Paediatric Population: 2 - 6 years: the minimum starting dose is 1 mg as 2.5 ml of syrup three times daily. This may be increased to 2 mg as 5 ml of syrup three or four times daily.
6 - 12 years: the minimum starting dose is 2 mg as 5 ml syrup three times daily. This may be increased to four times daily.
Over 12 years: the minimum starting dose is 2 mg three times daily given as 5 ml syrup. This may be increased to 4 mg as 10 ml syrup three or four times daily.
Ventolin is well tolerated by children so that, if necessary, these doses may be cautiously increased to the maximum dose.
For lower doses the syrup may be diluted with freshly prepared purified water.
Evohaler: VENTOLIN is administered by the oral inhaled route only.
In patients who find co-ordination of a pressurised metered-dose inhaler difficult a spacer may be used with VENTOLIN Evohaler.
Babies and young children using the VENTOLIN Evohaler may benefit from use of a paediatric spacer device with a face mask.
Relief of Acute Bronchospasm: Adults: 100 or 200 micrograms.
Children: 100 micrograms. The dose may be increased to 200 micrograms if required.
Prevention of Allergen or Exercise-Induced Bronchospasm: Adults: 200 micrograms before challenge or exertion.
Children: 100 micrograms before challenge or exertion. The dose may be increased to 200 micrograms if required.
Chronic Therapy: Adults: Up to 200 micrograms 4 times daily.
Children: Up to 200 micrograms 4 times daily.
On demand use of VENTOLIN should not exceed four times daily. Reliance on such supplementary use or a sudden increase in dose indicates deteriorating asthma (see Precautions).
Respirator Solution: VENTOLIN Respirator Solution is to be used with a respirator or nebuliser, only under the direction of a physician.
The solution must not be injected, or swallowed.
Delivery of the aerosol may be by facemask, 'T' piece or via an endotracheal tube. Intermittent positive pressure ventilation may be used but is rarely necessary. When there is a risk of anoxia through hypoventilation, oxygen should be added to the inspired air.
As many nebulisers operate on a continuous flow basis, it is likely that nebulised drug will be released in the local environment. Ventolin Respirator Solution should therefore be administered in a well-ventilated room, particularly in hospitals when several patients may be using nebulisers at the same time.
By intermittent administration: Intermittent treatment may be repeated 4 times daily.
Adults: VENTOLIN Respirator Solution 0.5 to 1.0 ml (2.5 to 5.0 milligrams of salbutamol) should be diluted to a final volume of 2.0 or 2.5 ml using sterile normal saline as a diluent. The resulting solution is inhaled from a suitably driven nebuliser until aerosol generation ceases. Using a correctly matched nebuliser and driving source this should take about 10 minutes.
VENTOLIN Respirator Solution may be used undiluted for intermittent administration. For this, 2.0 ml of VENTOLIN Respirator Solution (10.0 milligrams salbutamol) is placed in the nebuliser and the patient allowed to inhale the nebulised solution until bronchodilatation is achieved.
This usually takes 3 to 5 minutes.
Some adult patients may require higher doses of salbutamol, up to 10 milligrams, in which case nebulisation of the undiluted solution may continue until aerosol generation ceases.
Children: The same mode of administration for intermittent administration is also applicable to children. The usual dosage for children under the age of 12 years is 0.5 ml (2.5 milligrams salbutamol) diluted to 2.0 or 2.5 ml using sterile normal saline as a diluent. Some children may however require higher doses of salbutamol up to 5.0 milligrams.
Clinical efficacy of nebulised VENTOLIN in infants under 18 months is uncertain. As transient hypoxaemia may occur, supplemental oxygen therapy should be considered.
By continuous administration: VENTOLIN Respirator Solution is diluted using sterile normal saline to contain salbutamol 50-100 μg of salbutamol per ml, (1 to 2 ml solution made up to 100 ml with diluent). The diluted solution is administered as an aerosol by a suitably driven nebuliser. The usual rate of administration is 1 to 2 milligrams per hour.
Nebule: VENTOLIN Nebules are to be used undiluted. However, if prolonged delivery time is desirable (more than 10 minutes) dilution using sterile normal saline as a diluent may be required.
VENTOLIN Nebules are to be used with a nebuliser, under the direction of a physician.
The solution must not be injected or swallowed.
Delivery of the aerosol may be by facemask, 'T' piece or via an endotracheal tube. Intermittent positive pressure ventilation may be used but it is rarely necessary. When there is a risk of anoxia through hypoventilation, oxygen should be added to the inspired air.
As many nebulisers operate on a continuous flow basis, it is likely that nebulised drug will be released in the local environment. VENTOLIN nebules should therefore be administered in a well ventilated room, particularly in hospitals when several patients may be using nebulisers at the same time.
Adults and Children: A suitable starting dose of salbutamol by wet inhalation is 2.5 milligrams.
This may be increased to 5 milligrams. Treatment may be repeated four times daily. In adults higher dosing, up to 40 milligrams per day, can be given under strict medical supervision in hospital for the treatment of severe airways obstruction.
Clinical efficacy of nebulised VENTOLIN in infants under 18 months is uncertain. As transient hypoxaemia may occur, supplemental oxygen therapy should be considered.
Infusion: VENTOLIN parenteral preparations are to be used under the direction of a physician.
Note: The contents of the ampoules of VENTOLIN Solution For Intravenous Infusion must not be injected undiluted. The concentration should be reduced by 50% before administration.
VENTOLIN parenteral preparations should not be administered in the same syringe or infusion as any other medication.
In severe bronchospasm and status asthmaticus: Adults: Infusion: In status asthmaticus, infusion rates of 3 to 20 micrograms per minute are generally adequate but in patients with respiratory failure, higher dosage has been used with success. A starting dose of 5 micrograms per minute is recommended with appropriate adjustments in dosage according to patient response.
A suitable solution for infusion may be repeated by diluting 5 ml of VENTOLIN Solution For Intravenous Infusion in 500 ml of an infusion solution such as sodium chloride and dextrose injection BP to provide a salbutamol dose of 10 micrograms/ml of solution.
Children: At present there is insufficient evidence to recommend a dosage regimen for routine use in children.
In the management of premature labour: Treatment with VENTOLIN Solution For Intravenous Infusion should only be initiated by obstetricians/physicians experienced in the use of tocolytic agents. Ideally, it should be carried out in facilities adequately equipped to perform continuous monitoring of maternal and foetal health status.
Duration of treatment should not exceed 48 hours as data show that the main effect of tocolytic therapy is a delay in delivery of up to 48 hours. No statistically significant effect on perinatal mortality or morbidity has been observed in randomised, controlled trials. This delay may be used to administer glucocorticoids or to implement other measures known to improve perinatal health.
VENTOLIN Solution for infusion should be administered as early as possible after the diagnosis of premature labour, and after evaluation of the patient to eliminate any contraindications to the use of VENTOLIN (see Contraindications). This should include an adequate assessment of the patient's cardiovascular status with continuous ECG monitoring throughout treatment (see Precautions).
For this indication, VENTOLIN Solution for Intravenous Infusion is recommended using a solution prepared as previously mentioned. Infusion rates of 10 to 45 micrograms per minute are generally adequate to control uterine contractions but greater or lesser infusion rates may be required according to the strength and frequency of contractions. A starting rate of 10 micrograms per minute is recommended, increasing the rate at 10-minute intervals until there is evidence of patient response shown by diminution in strength, frequency or duration of contractions. Thereafter the infusion rate may be increased slowly until contractions cease. Careful attention should be given to cardio-respiratory function, including increases in pulse rate and changes in blood pressure, electrolytes, glucose and lactate levels and fluid balance monitoring. A maximum sustained maternal heart rate of 120 beats/min should not be exceeded. Treatment should be discontinued should signs of pulmonary oedema or myocardial ischaemia develop (see Precautions and Adverse Reactions).
Once uterine contractions have ceased the infusion rate should be maintained at the same level for 1 hour and then reduced by 50% decrements at 6-hourly intervals.
The most common signs and symptoms of overdose with VENTOLIN are transient beta-agonist pharmacologically mediated events (see Precautions and Adverse Reactions).
Hypokalaemia may occur following overdose with VENTOLIN. Serum potassium levels should be monitored.
Lactic acidosis has been reported in association with high therapeutic doses as well as overdoses of short-acting beta-agonist therapy, therefore monitoring for elevated serum lactate and consequent metabolic acidosis (particularly if there is persistence or worsening of tachypnea despite resolution of other signs of bronchospasm such as wheezing) may be indicated in the setting of overdose.
Syrup: The most common signs and symptoms of overdose with salbutamol are transient beta-agonist pharmacologically mediated events, including tachycardia, tremor, hyperactivity and metabolic effects including hypokalaemia (see Precautions and Adverse Reactions).
Respirator Solution: During continuous administration of VENTOLIN Respirator Solution, any signs of overdosage can usually be countered by withdrawal of the drug.
Syrup/Infusion: Nausea, vomiting and hyperglycaemia have been reported, predominantly in children and when salbutamol overdose has been taken via the oral route.
Treatment: Tablet/Syrup/Infusion: Further management should be as clinically indicated or as recommended by the national poisons centre, where available.
VENTOLIN are contraindicated in patients with a history of hypersensitivity to any of their components.
Non-i.v. formulations of VENTOLIN must not be used to arrest uncomplicated premature labour or threatened abortion.
Infusion: Obstetric: VENTOLIN solution for infusion, when used in the management of premature labour, is contraindicated in the following conditions: at a gestational age <22 weeks; intrauterine foetal death, known lethal congenital or lethal chromosomal malformation; any condition of the mother or foetus in which prolongation of the pregnancy is hazardous; in patients with pulmonary hypertension, pre-existing ischaemic heart disease or those patients with significant risk factors for ischaemic heart disease; threatened abortion during the 1st and 2nd trimester.
VENTOLIN should be administered cautiously to patients with thyrotoxicosis.
Tablet/Evohaler/Respirator Solution/Nebule/Infusion: The management of asthma should normally follow a stepwise programme, and patient response should be monitored clinically and by lung function tests.
Increasing use of short-acting inhaled beta2-agonists to control symptoms indicates deterioration of asthma control. Under these conditions, the patient's therapy plan should be reassessed. Sudden and progressive deterioration in asthma control is potentially life-threatening and consideration should be given to starting or increasing corticosteroid therapy. In patients considered at risk, daily peak flow monitoring may be instituted.
Tablet/Syrup/Evohaler/Respirator Solution/Nebule: Potentially serious hypokalaemia may result from beta2-agonist therapy mainly from parenteral and nebulised administration. Particular caution is advised in acute severe asthma as this effect may be potentiated by concomitant treatment with xanthine derivatives, steroids, diuretics and by hypoxia. It is recommended that serum potassium levels are monitored in such situations.
Tablet/Syrup/Respirator Solution/Nebule/Infusion: In common with other beta-adrenoceptor agonists, VENTOLIN can induce reversible metabolic changes, for example increased blood glucose levels. The diabetic patient may be unable to compensate for this and the development of ketoacidosis has been reported. Concurrent administration of corticosteroids can exaggerate this effect.
Tablet/Syrup/Respirator Solution/Nebule: Patients should be warned that if either the usual relief is diminished or the usual duration of action reduced, they should not increase the dose or its frequency of administration, but should seek medical advice.
Cardiovascular effects may be seen with sympathomimetic drugs, including salbutamol. There is some evidence from post-marketing data and published literature of rare occurrences of myocardial ischaemia associated with salbutamol. Patients with underlying severe heart disease (e.g. ischaemic heart disease, arrhythmia or severe heart failure) who are receiving salbutamol should be warned to seek medical advice if they experience chest pain or other symptoms of worsening heart disease. Attention should be paid to assessment of symptoms such as dyspnoea and chest pain, as they may be of either respiratory or cardiac origin.
Respirator Solution/Nebule: VENTOLIN must only be used by inhalation, to be breathed in through the mouth, and must not be injected or swallowed.
VENTOLIN should be used with caution in patients known to have received large doses of other sympathomimetic drugs.
A small number of cases of acute angle closure glaucoma have been reported in patients treated with a combination of nebulised VENTOLIN and ipratropium bromide. A combination of nebulised VENTOLIN with nebulised anticholinergics should therefore be used cautiously. Patients should receive adequate instruction in correct administration and be warned not to let the solution or mist enter the eye.
Respirator Solution/Nebule/Infusion: Lactic acidosis has been reported very rarely in association with high therapeutic doses of intravenous and nebulised short-acting beta-agonist therapy, mainly in patients being Lactic acidosis has been reported very rarely in association with high therapeutic doses of intravenous and nebulised short-acting beta-agonist therapy, mainly in patients being treated for an acute asthma exacerbation (see Adverse Reaction). Increase in lactate levels may lead to dyspnoea and compensatory hyperventilation, which could be misinterpreted as a sign of asthma treatment failure and lead to inappropriate intensification of short-acting beta-agonist treatment. It is therefore recommended that patients are monitored for the development of elevated serum lactate and consequent metabolic acidosis in this setting.
Evohaler/Respirator Solution/Nebule: As with other inhalation therapy, paradoxical bronchospasm may occur, resulting in an immediate increase in wheezing after dosing. This should be treated immediately with an alternative presentation or a different fast-acting inhaled bronchodilator, if immediately available. VENTOLIN should be discontinued, and if necessary a different fast-acting bronchodilator instituted for ongoing use.
Syrup: Bronchodilators should not be the only or main treatment in patients with severe or unstable asthma. Severe asthma requires regular medical assessment including lung function testing as patients are at risk of severe attacks and even death. Physicians should consider using oral corticosteroid therapy and/or the maximum recommended dose of inhaled corticosteroid in those patients.
Patients should seek medical advice if treatment with Ventolin syrup becomes less effective.
The dosage or frequency of administration should only be increased on medical advice.
Patients taking Ventolin syrup may also be receiving short-acting inhaled bronchodilators to relieve symptoms.
Increasing use of bronchodilators in particular short-acting inhaled beta2-agonists to relieve symptoms indicates deterioration of asthma control. The patient should be instructed to seek medical advice if short-acting relief bronchodilator treatment becomes less effective or they need more inhalations than usual.
In this situation patients should be reassessed and consideration given to the need for increased anti-inflammatory therapy (eg. Higher doses of inhaled corticosteroids or a course of oral corticosteroid). Severe exacerbations of asthma must be treated in the normal way.
Ventolin Syrup contains 5.6 mg sodium in each 5 ml of syrup. This should be taken into consideration by patients on a controlled sodium diet. Ventolin syrup is sugar free.
Evohaler: In the event of a previously effective dose of inhaled salbutamol failing to give relief for at least 3 hrs, the patient should be advised to seek medical advice in order that any necessary additional steps may be taken.
The patient's inhaler technique should be checked to make sure that the aerosol actuation is synchronised with inspiration of breath for optimum delivery of the drug to the lungs.
Infusion: The use of VENTOLIN parenteral preparations in the treatment of severe bronchospasm or status asthmaticus does not obviate the requirement for glucocorticoid steroid therapy as appropriate.
When practicable, administration of oxygen concurrently with parenteral VENTOLIN is recommended, particularly when it is given by intravenous infusion to hypoxic patients.
Diabetic patients and those concurrently receiving corticosteroids should be monitored frequently during intravenous infusion of VENTOLIN so that remedial steps (e.g. an increase in insulin dosage) can be taken to counter any metabolic change occurring. For these patients, VENTOLIN Solution for Intravenous Infusion should be diluted with Sodium Chloride Injection BP, rather than Sodium Chloride and Dextrose Injection BP.
Obstetric use only: In the treatment of premature labour, before VENTOLIN parenteral preparations are given to any patient with known or suspected heart disease, an adequate assessment of the patient's cardiovascular status should be made by a physician experienced in cardiology.
Tocolysis with VENTOLIN parenteral preparations is not recommended when membranes have ruptured or the cervix has dilated beyond 4 cm.
Tocolysis: Serious adverse reactions including death have been reported after administration of terbutaline/salbutamol to women in labor. In the mother, these include increased heart rate, transient hyperglycaemia, hypokalaemia, cardiac arrhythmias, pulmonary oedema and myocardial ischemia. Increased fetal heart rate and neonatal hypoglycaemia may occur as a result of maternal administration.
As maternal pulmonary oedema and myocardial ischaemia have been reported during or following treatment of premature labour with beta2-agonists, careful attention should be given to fluid balance and cardio-respiratory function, including ECG should be monitored. If signs of pulmonary oedema or myocardial ischaemia develop, discontinuation of treatment should be considered (see Dosage & Administration and Adverse Reactions).
In the treatment of premature labour by intravenous infusion of VENTOLIN increases in maternal heart rate of the order 20 to 50 beats per minute usually accompany the infusion. The maternal pulse rate should be monitored and not normally allowed to exceed a sustained rate of 120 beats per minute. The effect of infusion on foetal rate is less marked but increases of up to 20 beats per minute may occur.
Cautious use of salbutamol injections is required in pregnant patients when it is given for relief of bronchospasm so as to avoid interference with uterine contractibility.
Maternal blood pressure may fall slightly during the infusion; the effect being greater on diastolic than on systolic pressure. Falls in diastolic pressure are usually within the range of 10 to 20 mmHg.
Effects on the Ability to Drive and Use Machines: None known/reported.
Fertility: There is no information on the effects of salbutamol on human fertility. There were no adverse effects on fertility in animals (see Pharmacology: Toxicology: Preclinical Safety Data under Actions).
Pregnancy: Administration of drugs during pregnancy should only be considered if the expected benefit to the mother is greater than any possible risk to the foetus.
During worldwide marketing experience, rare cases of various congenital anomalies, including cleft palate and limb defects have been reported in the offspring of patients being treated with salbutamol. Some of the mothers were taking multiple medications during their pregnancies.
As no consistent pattern of defects can be discerned, and baseline rate for congenital anomalies is 2 to 3%, a relationship with salbutamol use cannot be established.
Syrup: As with the majority of drugs, there is little published evidence of its safety in the early stages of human pregnancy, but in animal studies there was evidence of some harmful effects on the foetus at very high dose levels.
Lactation: As salbutamol is probably secreted in breast milk its use in nursing mothers is not recommended unless the expected benefits outweigh any potential risk. It is not known whether salbutamol in breast milk has a harmful effect on the neonate.
Syrup: As salbutamol is probably secreted in breast milk its use in nursing mothers requires careful consideration.
It is not known whether salbutamol has a harmful effect on the neonate, and so its use should be restricted to situations where it is felt that the expected benefit to the mother is likely to outweigh any potential risk to the neonate.
Adverse events are listed as follows by system organ class and frequency. Frequencies are defined as: Very common (≥1/10), common (≥1/100 and <1/10), uncommon (≥1/1000 and <1/100), rare (≥1/10,000 and <1/1000) and very rare (<1/10,000) including isolated reports. Very common and common events were generally determined from clinical trial data. Rare and very rare events were generally determined from spontaneous data.
Immune system disorders: Very Rare: Hypersensitivity reactions including angioedema, urticaria, bronchospasm, hypotension and collapse.
Metabolism and nutrition disorders: Rare: Hypokalaemia.
Potentially serious hypokalaemia may result from beta
2-agonist therapy.
Respirator Solution/Nebule/Infusion: Very rare: Lactic acidosis.
Lactic acidosis has been reported very rarely in patients receiving intravenous and nebulised salbutamol therapy for the treatment of acute asthma exacerbation.
Nervous system disorders: Very Common: Tremor. Common: Headache. Very Rare: Hyperactivity.
Evohaler/Respirator Solution/Nebule: Common: Tremor, headache.
Cardiac disorders: Common: Tachycardia, palpitations. Rare: Cardiac arrhythmias including atrial fibrillation, supraventricular tachycardia and extrasystoles.
Syrup: Unknown: Myocardial ischaemia* (see Precautions).
*reported spontaneously in post-marketing data therefore frequency regarded as unknown.
Evohaler/Respirator Solution/Nebule: Common: Tachycardia. Uncommon: Palpitations.
Infusion: Very common: Tachycardia, palpitations. Uncommon: Myocardial ischaemia*.
*In the management of pre-term labour with VENTOLIN injection/solution for infusion.
Vascular disorders: Rare: Peripheral vasodilation.
Musculoskeletal and connective tissue disorders: Common: Muscle cramps. Very Rare: Feeling of muscle tension.
Evohaler/Respirator Solution/Nebule: Uncommon: Muscle cramps.
Respiratory, thoracic and mediastinal disorders: Evohaler/Respirator Solution/Nebule: Very Rare: Paradoxical bronchospasm.
Infusion: Uncommon: Pulmonary oedema.
In the management of pre-term labour, VENTOLIN injection and solution for intravenous infusion has uncommonly been associated with pulmonary oedema. Patients with predisposing factors including multiple pregnancies, fluid overload, maternal infection and pre-eclampsia may have an increased risk of developing pulmonary oedema.
Gastrointestinal disorders: Evohaler/Respirator Solution/Nebule: Uncommon: Mouth and throat irritation.
Infusion: Very Rare: Nausea and vomiting.
In the management of premature labour, intravenous infusion of VENTOLIN has very rarely been associated with nausea and vomiting.
Injury, poisoning and procedural complications: Infusion: Very Rare: Slight pain or stinging on intramuscular use of undiluted injection.
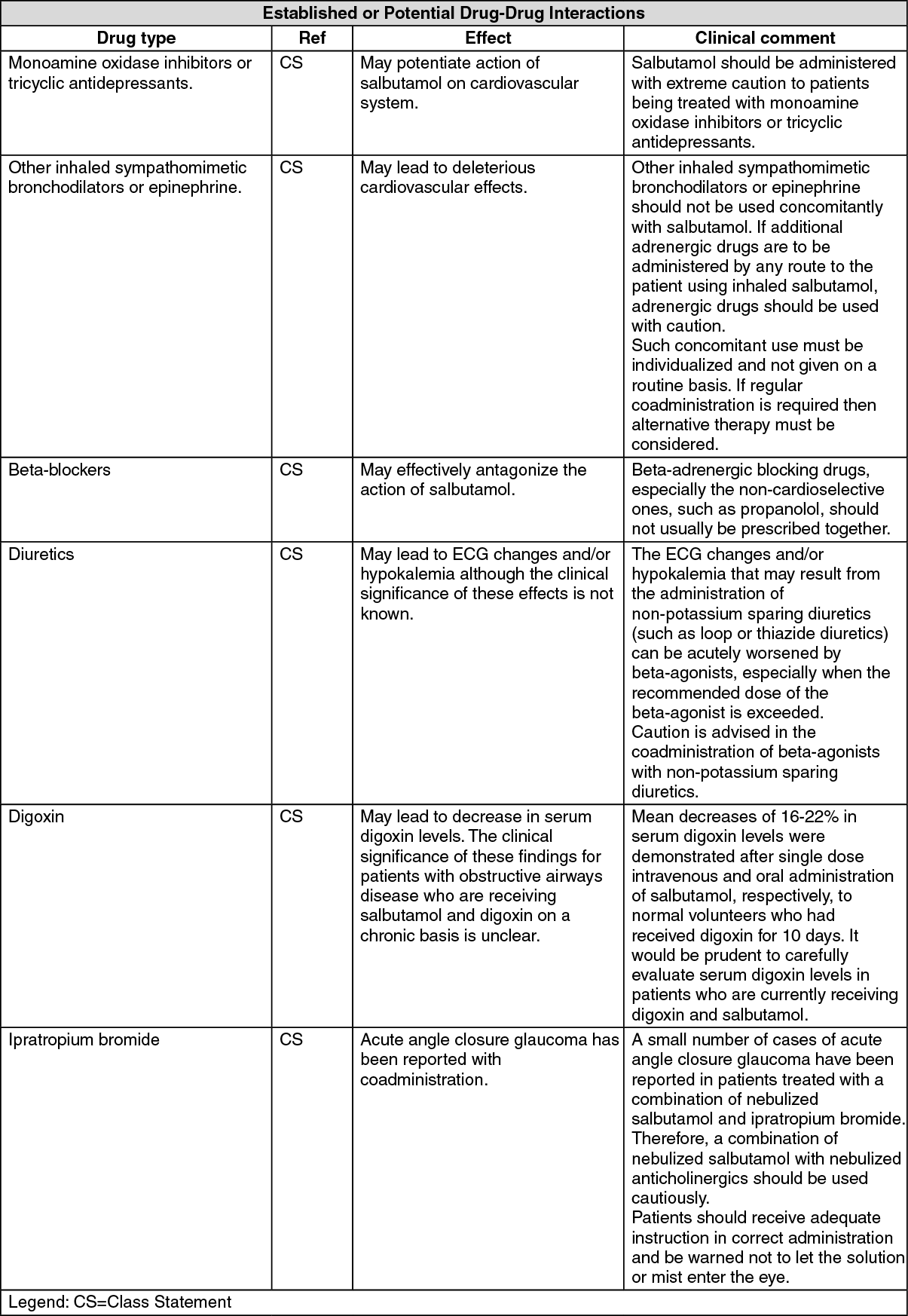
VENTOLIN and non-selective beta-blocking drugs, such as propranolol, should not usually be prescribed together.
Respirator Solution: (See table.)
 Click on icon to see table/diagram/image
Nebule:
Click on icon to see table/diagram/image
Nebule: VENTOLIN is not contraindicated in patients under treatment with monoamine oxidase inhibitors (MAOIs).
Incompatibilities: None known/reported.
Syrup: Ventolin syrup is sugar free. Dilution of Ventolin syrup with Syrup BP or Sorbitol solution is not recommended as this may result in the precipitation of the cellulose thickening agent. If dilution is required freshly prepared Purified Water BP should be used.
Special Precautions for Disposal and Other Handling: Syrup: Ventolin syrup may be diluted with Purified Water BP (50% v/v). The resulting mixture should be protected from light and used within 28 days.
A 50% v/v dilution of Ventolin syrup has been shown to be adequately preserved against microbial contamination. However, to avoid the possibility of introducing excessive microbial contamination, the Purified Water used for dilution should be recently prepared or alternatively it should be boiled and cooled immediately before use.
Admixture of Ventolin syrup with other liquid preparation is not recommended.
Instructions for Use and Handling: Evohaler: Testing the Inhaler: Before using for the first time, remove the mouthpiece cover by gently squeezing the sides of the cover, shake the inhaler well, and release two puffs into the air to make sure that it works. If it has not been used for 5 days, shake it well and release 2 puffs into the air to make sure that it works.
Using the Inhaler: 1. Remove the mouthpiece cover by gently squeezing the sides of the cover.
2. Check inside and outside of the inhaler including the mouthpiece for presence of loose objects.
3. Shake the inhaler well to ensure that any loose objects are removed and that the contents of the inhaler are evenly mixed.
4. Hold the inhaler upright between fingers and thumb with the thumb on the base, below the mouthpiece.
5. Breathe out as far as is comfortable and then place the mouthpiece in the mouth between the teeth and close the lips around it but do not bite it.
6. Just after starting to breathe in through the mouth, press down on the top of the inhaler to release the VENTOLIN while still breathing in steadily and deeply.
7. While holding the breath, take the inhaler from the mouth and take the finger from the top of the inhaler. Continue holding the breath for as long as is comfortable.
8. If the patients is to take further puffs keep the inhaler upright and wait about half a minute before repeating steps three to seven.
9. Replace the mouthpiece cover by firmly pushing and snapping the cap into position.
Important: Do not rush stages 5, 6 and 7. It is important to start to breathe in as slowly as possible just before operating the inhaler.
Practise in front of a mirror for the first few times. If 'mist' is seen coming from the top of the inhaler or the sides of the mouth, start again from stage two.
If the doctor has given different instructions for using the inhaler, follow them carefully. Tell the doctor if there are any difficulties.
Cleaning: The inhaler should be cleaned at least once a week.
1. Remove the metal canister from the plastic casing of the inhaler and remove the mouthpiece cover.
2. Rinse the actuator thoroughly under warm running water.
3. Dry the actuator thoroughly inside and out.
4. Replace the metal canister and mouthpiece cover.
Do not put the metal canister into water.
Dilution: Respirator Solution/Nebule: VENTOLIN respirator solution and/or nebules may be diluted with sterile normal saline.
Any unused solution in the chamber of the nebuliser must be discarded.
Infusion: VENTOLIN parenteral preparations may be diluted with Water for Injections BP, Sodium Chloride Injection BP, Sodium Chloride and Dextrose Injection BP or Dextrose Injection BP. These are the only recommended diluents.
Tablet/Syrup: Store below 30°C.
Syrup: Protect from light.
Evohaler: Replace the mouthpiece cover firmly and snap it into position.
VENTOLIN should be store below 30°C.
Protect from frost and direct sunlight.
As with most inhaled medications in aerosol canisters, the therapeutic effect of this medication may decrease when the canister is cold.
The canister should not be broken, punctured or burnt, even when apparently empty.
Respirator Solution: VENTOLIN Respirator Solution should be stored at a temperature below 30°C and protect from light.
Once the bottle has been opened the contents should be discarded after one month.
Nebule: VENTOLIN Nebules should be stored below 30°C and protected from light.
Infusion: VENTOLIN parenteral preparations should be protected from light and store at a temperature below 30°C.
All unused admixtures of VENTOLIN Parenteral Preparations with infusion fluids should be discarded twenty-four hours after preparation.
R03AC02 - salbutamol ; Belongs to the class of adrenergic inhalants, selective beta-2-adrenoreceptor agonists. Used in the treatment of obstructive airway diseases.
R03CC02 - salbutamol ; Belongs to the class of adrenergics for systemic use, selective beta-2-adrenoreceptor agonists. Used in the treatment of obstructive airway diseases.
Ventolin evohaler 100 mcg
200 dose x 1's
Ventolin infusion (amp) 5 mg/5 mL
10 × 1's
Ventolin respirator soln 5 mg/mL
10 mL x 1's
Ventolin nebules 2.5 mg/2.5 mL
20 × 1's
Ventolin syr 2 mg/5 mL
120 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 5 mg_5 mL33c95761-45ac-46df-8233-9faa000a4bfd.GIF)




 Sign Out
Sign Out
