


 Sign Out
Sign Out

Posology: Previously Untreated HL: The recommended dose in combination with chemotherapy (doxorubicin [A], vinblastine [V] and dacarbazine [D] [AVD]) is 1.2 mg/kg administered as an intravenous infusion over 30 minutes on days 1 and 15 of each 28-day cycle for 6 cycles (see Pharmacology: Pharmacodynamics under Actions).
Primary prophylaxis with growth factor support (G-CSF), beginning with the first dose, is recommended for all adult patients with previously untreated HL receiving combination therapy (see Precautions).
Refer to the summary of product characteristics (SmPC) of chemotherapy agents given in combination with BRENTUXIMAB VEDOTIN (ADCETRIS) for patients with previously untreated HL.
HL at increased risk of relapse or progression: The recommended dose is 1.8 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks.
BRENTUXIMAB VEDOTIN (ADCETRIS) treatment should start following recovery from ASCT based on clinical judgment. These patients should receive up to 16 cycles (see Pharmacology: Pharmacodynamics under Actions).
Relapsed or refractory HL: The recommended dose is 1.8 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks.
The recommended starting dose for the retreatment of patients who have previously responded to treatment with BRENTUXIMAB VEDOTIN (ADCETRIS) is 1.8 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks. Alternatively, treatment may be started at the last tolerated dose (see Pharmacology: Pharmacodynamics under Actions).
Treatment should be continued until disease progression or unacceptable toxicity (see Precautions).
Patients who achieve stable disease or better should receive a minimum of 8 cycles and up to a maximum of 16 cycles (approximately 1 year) (see Pharmacology: Pharmacodynamics under Actions).
Previously untreated sALCL or other CD30-expressing peripheral T-cell lymphomas: The recommended dose in combination with chemotherapy (cyclophosphamide [C], doxorubicin [H] and prednisone [P] [CHP]) is 1.8 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks for 6 to 8 cycles (see Pharmacology: Pharmacodynamics under Actions).
Primary prophylaxis with G-CSF, beginning with the first dose, is recommended for all adult patients with previously untreated sALCL or other CD30-expressing peripheral T-cell lymphomas, receiving combination therapy (see Precautions).
Refer to the SmPCs of chemotherapy agents given in combination with BRENTUXIMAB VEDOTIN (ADCETRIS) for patients with previously untreated sALCL or other CD30-expressing peripheral T-cell lymphomas.
Relapsed or refractory sALCL: The recommended dose is 1.8 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks.
The recommended starting dose for the retreatment of patients who have previously responded to treatment with BRENTUXIMAB VEDOTIN (ADCETRIS) is 1.8 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks. Alternatively, treatment may be started at the last tolerated dose (see Pharmacology: Pharmacodynamics under Actions).
Treatment should be continued until disease progression or unacceptable toxicity (see Precautions).
Patients who achieve stable disease or better should receive a minimum of 8 cycles and up to a maximum of 16 cycles (approximately 1 year) (see Pharmacology: Pharmacodynamics under Actions).
CTCL: The recommended dose is 1.8 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks.
Patients with CTCL should receive up to 16 cycles (see Pharmacology: Pharmacodynamics under Actions).
General: If the patient's weight is more than 100 kg, the dose calculation should use 100 kg (see Special precautions for disposal and other handling under Cautions for Usage).
Complete blood counts should be monitored prior to administration of each dose of this treatment (see Precautions).
Patients should be monitored during and after infusion (see Precautions).
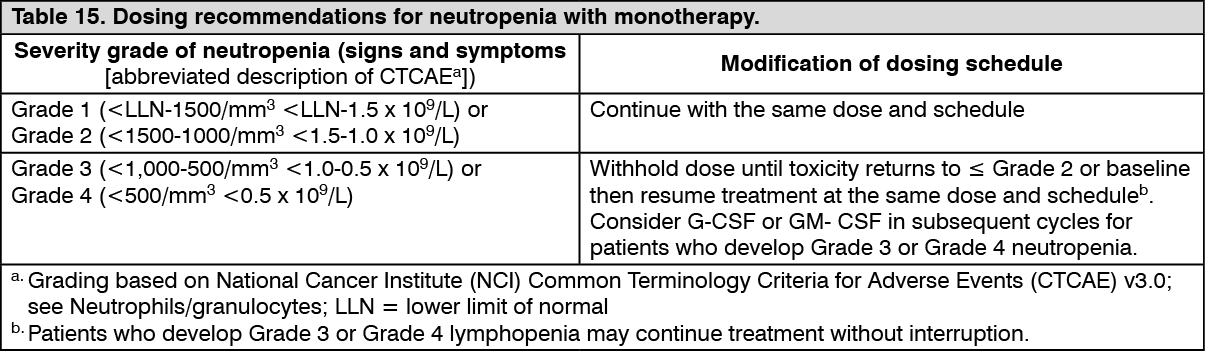
Dose adjustments: Neutropenia: If neutropenia develops during treatment, it should be managed by dose delays. See Table 15 and Table 16 for appropriate dosing recommendations for monotherapy and combination therapy, respectively (see also Precautions). (See Tables 15 and 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image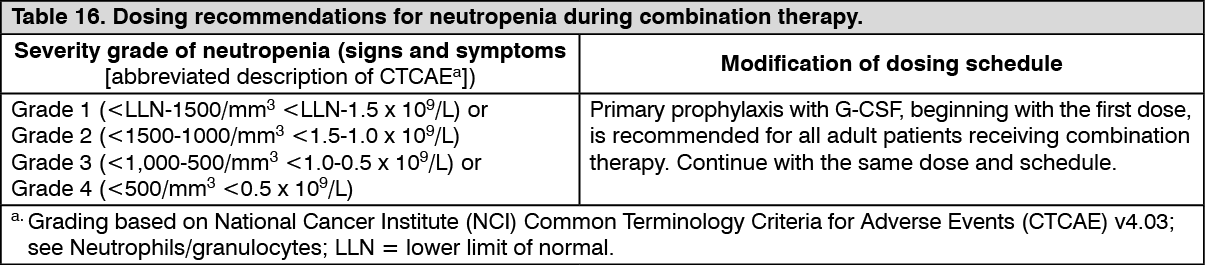 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePeripheral neuropathy: If peripheral sensory or motor neuropathy emerges or worsens during treatment see Tables 17 and 18 as follows for appropriate dosing recommendations for monotherapy and combination therapy (see Precautions). (See Tables 17 and 18.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image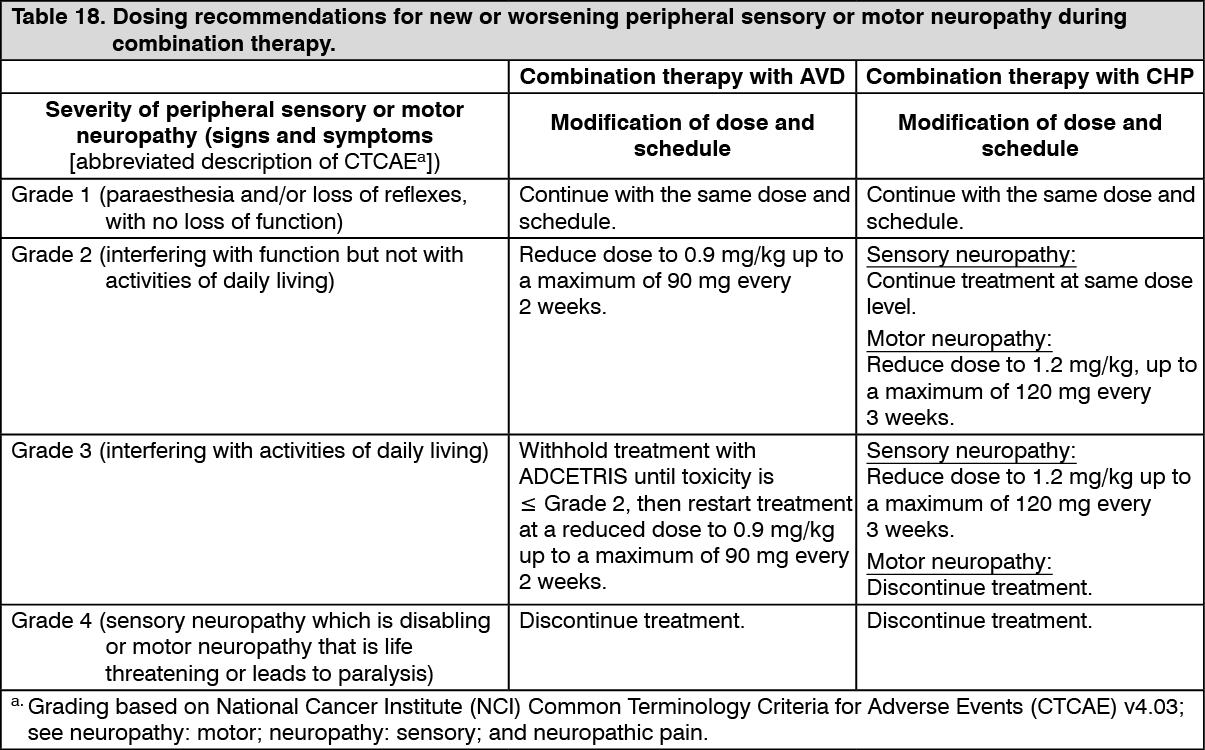 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSpecial patient populations: Renal and hepatic impairment: Combination therapy: Patients with renal impairment should be closely monitored for adverse events. There is no clinical trial experience using BRENTUXIMAB VEDOTIN (ADCETRIS) in combination with chemotherapy in patients with renal impairment, where serum creatinine is ≥2.0 mg/dL and/or creatinine clearance or calculated creatinine clearance is ≤40 mL/minute. Use of BRENTUXIMAB VEDOTIN (ADCETRIS) in combination with chemotherapy should be avoided in patients with severe renal impairment.
Patients with hepatic impairment should be closely monitored for adverse events. The recommended starting dose in patients with mild hepatic impairment receiving BRENTUXIMAB VEDOTIN (ADCETRIS) in combination with AVD is 0.9 mg/kg administered as an intravenous infusion over 30 minutes every 2 weeks. The recommended starting dose in patients with mild hepatic impairment receiving BRENTUXIMAB VEDOTIN (ADCETRIS) in combination with CHP is 1.2 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks. There is no clinical trial experience using BRENTUXIMAB VEDOTIN (ADCETRIS) in combination with chemotherapy in patients with hepatic impairment, where total bilirubin is >1.5 times the upper limit of normal (ULN) (unless due to Gilbert syndrome), or aspartate aminotransferase (AST) or alanine aminotransferase (ALT) are >3 times the ULN, or >5 times the ULN if their elevation may be reasonably ascribed to the presence of HL in the liver. Use of BRENTUXIMAB VEDOTIN (ADCETRIS) in combination with chemotherapy should be avoided in patients with moderate and severe hepatic impairment.
Monotherapy: The recommended starting dose in patients with severe renal impairment is 1.2 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks. Patients with renal impairment should be closely monitored for adverse events (see Pharmacology: Pharmacokinetics under Actions).
The recommended starting dose in patients with hepatic impairment is 1.2 mg/kg administered as an intravenous infusion over 30 minutes every 3 weeks. Patients with hepatic impairment should be closely monitored for adverse events (see Pharmacology: Pharmacokinetics under Actions).
Elderly: The dosing recommendations for patients aged 65 and older are the same as for adults. Currently available data are described in Adverse Reactions, Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions.
Paediatric population: The safety and efficacy of BRENTUXIMAB VEDOTIN (ADCETRIS) in children less than 18 years have not yet been established. Currently available data are described in Adverse Reactions and Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions but no recommendation on a posology can be made.
In nonclinical studies, thymus depletion has been observed (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Method of administration: The recommended dose of BRENTUXIMAB VEDOTIN (ADCETRIS) is infused over 30 minutes.
For instructions on reconstitution and dilution of the medicinal product before administration, see Special precautions for disposal and other handling under Cautions for Usage.
BRENTUXIMAB VEDOTIN (ADCETRIS) must not be administered as an intravenous push or bolus. BRENTUXIMAB VEDOTIN (ADCETRIS) should be administered through a dedicated intravenous line and it must not be mixed with other medicinal products (see Incompatibilities under Cautions for Usage).