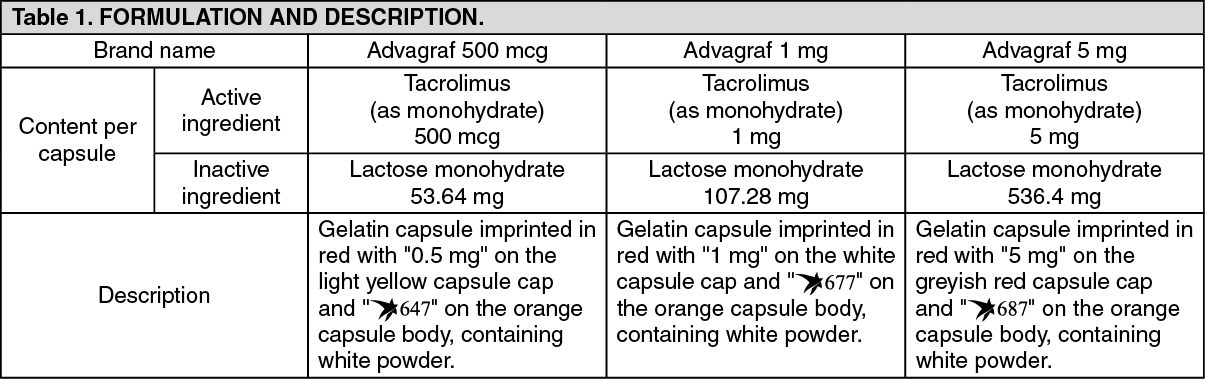
See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacotherapeutic group: Calcineurin inhibitors.
Pharmacology: Pharmacodynamics: Mechanism of action: At the molecular level, the effects of tacrolimus appear to be mediated by binding to a cytosolic protein (FKBP12) which is responsible for the intracellular accumulation of the compound. The FKBP12-tacrolimus complex specifically and competitively binds to and inhibits calcineurin, leading to a calcium-dependent inhibition of T-cell signal transduction pathways, thereby preventing transcription of a discrete set of cytokine genes.
Tacrolimus is a highly potent immunosuppressive agent and has proven activity in both in vitro and in vivo experiments.
In particular, tacrolimus inhibits the formation of cytotoxic lymphocytes, which are mainly responsible for graft rejection. Tacrolimus suppresses T-cell activation and T-helper-cell dependent B-cell proliferation, as well as the formation of lymphokines (such as interleukins-2, -3, and γ-interferon) and the expression of the interleukin-2 receptor.
Results from clinical trials performed with once-daily tacrolimus Advagraf: Liver transplantation: The efficacy and safety of Advagraf and Prograf, both in combination with corticosteroids, was compared in 471 de novo liver transplant recipients. The event rate of biopsy confirmed acute rejection within the first 24 weeks after transplantation was 32.6% in the Advagraf group (N=237) and 29.3% in the Prograf group (N=234). The treatment difference (Advagraf - Prograf) was 3.3% (95% confidence interval [-5.7%, 12.3%]). The 12-month patient survival rates were 89.2% for Advagraf and 90.8% for Prograf; in the Advagraf arm 25 patients died (14 female, 11 male) and in the Prograf arm 24 patients died (5 female, 19 male). 12-month graft survival was 85.3% for Advagraf and 85.6% for Prograf.
Kidney transplantation: The efficacy and safety of Advagraf and Prograf, both in combination with mycophenolate mofetil (MMF) and corticosteroids, was compared in 667 de novo kidney transplant recipients. The event rate for biopsy-confirmed acute rejection within the first 24 weeks after transplantation was 18.6% in the Advagraf group (N=331) and 14.9% in the Prograf group (N=336). The treatment difference (Advagraf-Prograf) was 3.8% (95% confidence interval [-2.1%, 9.6%]). The 12-month patient survival rates were 96.9% for Advagraf and 97.5% for Prograf; in the Advagraf arm 10 patients died (3 female, 7 male) and in the Prograf arm 8 patients died (3 female, 5 male). 12-month graft survival was 91.5% for Advagraf and 92.8% for Prograf.
The efficacy and safety of Prograf, ciclosporin and Advagraf, all in combination with basiliximab antibody induction, MMF and corticosteroids, was compared in 638 de novo kidney transplant recipients. The incidence of efficacy failure at 12 months (defined as death, graft loss, biopsy-confirmed acute rejection, or lost to follow-up) was 14.0% in the Advagraf group (N=214), 15.1% in the Prograf group (N=212) and 17.0% in the ciclosporin group (N=212). The treatment difference was -3.0% (Advagraf-ciclosporin) (95.2% confidence interval [-9.9%, 4.0%]) for Advagraf vs. ciclosporin and -1.9% (Prograf-ciclosporin) (95.2% confidence interval [-8.9%, 5.2%]) for Prograf vs. ciclosporin. The 12-month patient survival rates were 98.6% for Advagraf, 95.7% for Prograf and 97.6% for ciclosporin; in the Advagraf arm 3 patients died (all male), in the Prograf arm 10 patients died (3 female, 7 male) and in the ciclosporin arm 6 patients died (3 female, 3 male). 12-month graft survival was 96.7% for Advagraf, 92.9% for Prograf and 95.7% for ciclosporin.
Clinical efficacy and safety of Prograf capsules bid in primary organ transplantation: In prospective studies oral Prograf was investigated as primary immunosuppressant in approximately 175 patients following lung, 475 patients following pancreas and 630 patients following intestinal transplantation. Overall, the safety profile of oral Prograf in these published studies appeared to be similar to what was reported in the large studies, where Prograf was used as primary treatment in liver, kidney and heart transplantation. Efficacy results of the largest studies in each indication are summarised as follows.
Lung transplantation: The interim analysis of a recent multicentre study using oral Prograf discussed 110 patients who underwent 1:1 randomisation to either tacrolimus or ciclosporin. Tacrolimus was started as continuous intravenous infusion at a dose of 0.01 to 0.03 mg/kg/day and oral tacrolimus was administered at a dose of 0.05 to 0.3 mg/kg/day. A lower incidence of acute rejection episodes for tacrolimus- versus ciclosporin-treated patients (11.5% versus 22.6%) and a lower incidence of chronic rejection, the bronchiolitis obliterans syndrome (2.86% versus 8.57%), was reported within the first year after transplantation. The 1-year patient survival rate was 80.8% in the tacrolimus and 83% in the ciclosporin group.
Another randomised study included 66 patients on tacrolimus versus 67 patients on ciclosporin. Tacrolimus was started as continuous intravenous infusion at a dose of 0.025 mg/kg/day and oral tacrolimus was administered at a dose of 0.15 mg/kg/day with subsequent dose adjustments to target trough levels of 10 to 20 ng/ml. The 1-year patient survival was 83% in the tacrolimus and 71% in the ciclosporin group, the 2-year survival rates were 76% and 66%, respectively. Acute rejection episodes per 100 patient-days were numerically fewer in the tacrolimus (0.85 episodes) than in the ciclosporin group (1.09 episodes). Obliterative bronchiolitis developed in 21.7% of patients in the tacrolimus group compared with 38.0% of patients in the ciclosporin group (p=0.025). Significantly more ciclosporin-treated patients (n=13) required a switch to tacrolimus than tacrolimus-treated patients to ciclosporin (n=2) (p=0.02) (Keenan et al., Ann Thoracic Surg 1995;60:580).
In an additional two-centre study, 26 patients were randomised to the tacrolimus versus 24 patients to the ciclosporin group. Tacrolimus was started as continuous intravenous infusion at a dose of 0.05 mg/kg/day and oral tacrolimus was administered at a dose of 0.1 to 0.3 mg/kg/day with subsequent dose adjustments to target trough levels of 12 to 15 ng/ml. The 1-year survival rates were 73.1% in the tacrolimus versus 79.2% in the ciclosporin group. Freedom from acute rejection was higher in the tacrolimus group at 6 months (57.7% versus 45.8%) and at 1 year after lung transplantation (50% versus 33.3%).
The three studies demonstrated similar survival rates. The incidences of acute rejection were numerically lower with tacrolimus in all three studies and one of the studies reported a significantly lower incidence of bronchiolitis obliterans syndrome with tacrolimus.
Pancreas transplantation: A multicentre study using oral Prograf included 205 patients undergoing simultaneous pancreas-kidney transplantation who were randomised to tacrolimus (n=103) or to ciclosporin (n=102). The initial oral per protocol dose of tacrolimus was 0.2 mg/kg/day with subsequent dose adjustments to target trough levels of 8 to 15 ng/ml by Day 5 and 5 to 10 ng/ml after Month 6. Pancreas survival at 1 year was significantly superior with tacrolimus: 91.3% versus 74.5% with ciclosporin (p <0.0005), whereas renal graft survival was similar in both groups. In total 34 patients switched treatment from ciclosporin to tacrolimus, whereas only 6 tacrolimus patients required alternative therapy.
Intestinal transplantation: Published clinical experience from a single centre on the use of oral Prograf for primary treatment following intestinal transplantation showed that the actuarial survival rate of 155 patients (65 intestine alone, 75 liver and intestine, and 25 multivisceral) receiving tacrolimus and prednisone was 75% at 1 year, 54% at 5 years, and 42% at 10 years. In the early years the initial oral dose of tacrolimus was 0.3 mg/kg/day. Results continuously improved with increasing experience over the course of 11 years. A variety of innovations, such as techniques for early detection of Epstein-Barr (EBV) and CMV infections, bone marrow augmentation, the adjunct use of the interleukin-2 antagonist daclizumab, lower initial tacrolimus doses with target trough levels of 10 to 15 ng/ml, and most recently allograft irradiation were considered to have contributed to improved results in this indication over time.
Pharmacokinetics: Absorption: In man tacrolimus has been shown to be able to be absorbed throughout the gastrointestinal tract. Available tacrolimus is generally rapidly absorbed. Advagraf is a prolonged-release formulation of tacrolimus resulting in an extended oral absorption profile with an average time to maximum blood concentration (Cmax) of approximately 2 hours (tmax).
Absorption is variable and the mean oral bioavailability of tacrolimus (investigated with the Prograf formulation) is in the range of 20%-25% (individual range in adult patients 6%-43%). The oral bioavailability of Advagraf was reduced when it was administered after a meal. Both the rate and extent of absorption of Advagraf were reduced when administered with food.
Bile flow does not influence the absorption of tacrolimus and therefore treatment with Advagraf may commence orally.
A strong correlation exists between AUC and whole blood trough levels at steady-state for Advagraf. Monitoring of whole blood trough levels therefore provides a good estimate of systemic exposure.
Distribution: In man, the disposition of tacrolimus after intravenous infusion may be described as biphasic.
In the systemic circulation, tacrolimus binds strongly to erythrocytes resulting in an approximate 20:1 distribution ratio of whole blood/plasma concentrations. In plasma, tacrolimus is highly bound (>98.8%) to plasma proteins, mainly to serum albumin and α-1-acid glycoprotein.
Tacrolimus is extensively distributed in the body. The steady-state volume of distribution based on plasma concentrations is approximately 1300 l (healthy subjects). Corresponding data based on whole blood averaged 47.6 l.
Metabolism: Tacrolimus is widely metabolised in the liver, primarily by the cytochrome P450-3A4 (CYP3A4) and the cytochrome P450-3A5 (CYP3A5). Tacrolimus is also considerably metabolised in the intestinal wall. There are several metabolites identified. Only one of these has been shown in vitro to have immunosuppressive activity similar to that of tacrolimus. The other metabolites have only weak or no immunosuppressive activity. In systemic circulation only one of the inactive metabolites is present at low concentrations. Therefore, metabolites do not contribute to the pharmacological activity of tacrolimus.
Excretion: Tacrolimus is a low-clearance substance. In healthy subjects, the average total body clearance estimated from whole blood concentrations was 2.25 l/h. In adult liver, kidney and heart transplant patients, values of 4.1 l/h, 6.7 l/h and 3.9 l/h, respectively, have been observed. Factors such as low haematocrit and protein levels, which result in an increase in the unbound fraction of tacrolimus, or corticosteroid-induced increased metabolism, are considered to be responsible for the higher clearance rates observed following transplantation.
The half-life of tacrolimus is long and variable. In healthy subjects, the mean half-life in whole blood is approximately 43 hours.
Following intravenous and oral administration of 14C-labelled tacrolimus, most of the radioactivity was eliminated in the faeces. Approximately 2% of the radioactivity was eliminated in the urine. Less than 1% of unchanged tacrolimus was detected in the urine and faeces, indicating that tacrolimus is almost completely metabolised prior to elimination: bile being the principal route of elimination.
Toxicology: Preclinical safety data: The kidneys and the pancreas were the primary organs affected in toxicity studies performed in rats and baboons. In rats, tacrolimus caused toxic effects to the nervous system and the eyes. Reversible cardiotoxic effects were observed in rabbits following intravenous administration of tacrolimus.
Embryotoxicity was observed in animal studies.
Tacrolimus subcutaneously administered to male rats at a doses of 2 or 3 mg/kg/day (1.6 to 6.4 times the clinical dose range based on body surface area) resulted in a dose-related decrease in sperm count.
Tacrolimus given orally at 1.0 mg/kg (0.8 to 2.2 times the clinical dose range based on body surface area) to male and female rats, prior to and during mating, as well as to dams during gestation and lactation, was associated with embryolethality and adverse effects on female reproduction which were indicated by a higher rate of post-implantation loss and increased numbers of undelivered and nonviable pups. When given at 3.2 mg/kg (2.6 to 6.9 times the clinical dose range based on body surface area), tacrolimus was associated with maternal and paternal toxicity as well as reproductive toxicity including marked adverse effects on estrus cycles, parturition, pup viability, and pup malformations.
For the prophylaxis of transplant rejection in adult kidney or liver allograft recipients, and treatment of allograft rejection resistant to treatment with other immunosuppressive medicinal products in adult patients.
Advagraf is a once-a-day oral formulation of tacrolimus. Tacrolimus monohydrate (Advagraf) therapy requires careful monitoring by adequately qualified and equipped personnel. This medicinal product should only be prescribed, and changes in immunosuppressive therapy initiated, by physicians experienced in immunosuppressive therapy and the management of transplant patients.
Inadvertent, unintentional or unsupervised switching of immediate- or prolonged-release formulations of tacrolimus is unsafe. This can lead to graft rejection or increased incidence of side effects, including under- or over-immunosuppression, due to clinically relevant differences in systemic exposure to tacrolimus. Patients should be maintained on a single formulation of tacrolimus with the corresponding daily dosing regimen; alterations in formulation or regimen should only take place under the close supervision of a transplant specialist (see Precautions and Adverse Reactions). Following conversion to any alternative formulation, therapeutic drug monitoring must be performed and dose adjustments made to ensure that systemic exposure to tacrolimus is maintained.
Posology: The recommended initial doses presented as follows are intended to act solely as a guideline. Tacrolimus monohydrate (Advagraf) is routinely administered in conjunction with other immunosuppressive agents in the initial post-operative period. The dose may vary depending upon the immunosuppressive regimen chosen. Tacrolimus monohydrate (Advagraf) dosing should primarily be based on clinical assessments of rejection and tolerability in each patient individually aided by blood level monitoring (see as follows under "Therapeutic drug monitoring"). If clinical signs of rejection are apparent, alteration of the immunosuppressive regimen should be considered.
In de novo kidney and liver transplant patients AUC0-24 of tacrolimus for Advagraf on Day 1 was 30% and 50% lower respectively, when compared with that for Prograf at equivalent doses. By Day 4, systemic exposure as measured by trough levels is similar for both kidney and liver transplant patients with both formulations. Careful and frequent monitoring of tacrolimus trough levels is recommended in the first two weeks post-transplant with Advagraf to ensure adequate drug exposure in the immediate post-transplant period. As tacrolimus is a substance with low clearance, adjustments to the Advagraf dose regimen may take several days before steady state is achieved.
To suppress graft rejection, immunosuppression must be maintained; consequently, no limit to the duration of oral therapy can be given.
Prophylaxis of kidney transplant rejection: Tacrolimus monohydrate (Advagraf) therapy should commence at a dose of 0.20-0.30 mg/kg/day administered once daily in the morning. Administration should commence within 24 hours after the completion of surgery.
Tacrolimus monohydrate (Advagraf) doses are usually reduced in the post-transplant period. It is possible in some cases to withdraw concomitant immunosuppressive therapy, leading to Tacrolimus monohydrate (Advagraf) monotherapy. Post-transplant changes in the condition of the patient may alter the pharmacokinetics of tacrolimus and may necessitate further dose adjustments.
Prophylaxis of liver transplant rejection: Tacrolimus monohydrate (Advagraf) therapy should commence at a dose of 0.10-0.20 mg/kg/day administered once daily in the morning. Administration should commence approximately 12-18 hours after the completion of surgery.
Tacrolimus monohydrate (Advagraf) doses are usually reduced in the post-transplant period. It is possible in some cases to withdraw concomitant immunosuppressive therapy, leading to Tacrolimus monohydrate (Advagraf) monotherapy. Post-transplant improvement in the condition of the patient may alter the pharmacokinetics of tacrolimus and may necessitate further dose adjustments.
Conversion of Prograf-treated patients to Advagraf: Allograft transplant patients maintained on twice daily Prograf capsules dosing requiring conversion to once daily Advagraf should be converted on a 1:1 (mg:mg) total daily dose basis. Tacrolimus monohydrate (Advagraf) should be administered in the morning.
In stable patients converted from Prograf capsules (twice daily) to Advagraf (once daily) on a 1:1 (mg:mg) total daily dose basis, the systemic exposure to tacrolimus (AUC0-24) for Advagraf was approximately 10% lower than that for Prograf. The relationship between tacrolimus trough levels (C24) and systemic exposure (AUC0-24) for Advagraf is similar to that of Prograf. When converting from Prograf capsules to Advagraf, trough levels should be measured prior to conversion and within two weeks after conversion. Following conversion, tacrolimus trough levels should be monitored and if necessary dose adjustments made to maintain similar systemic exposure. Dose adjustments should be made to ensure that similar systemic exposure is maintained.
Conversion from ciclosporin to tacrolimus: Care should be taken when converting patients from ciclosporin-based to tacrolimus-based therapy (see Precautions and Interactions). The combined administration of ciclosporin and tacrolimus is not recommended. Tacrolimus monohydrate (Advagraf) therapy should be initiated after considering ciclosporin blood concentrations and the clinical condition of the patient. Dosing should be delayed in the presence of elevated ciclosporin blood levels. In practice, tacrolimus-based therapy has been initiated 12-24 hours after discontinuation of ciclosporin. Monitoring of ciclosporin blood levels should be continued following conversion as the clearance of ciclosporin might be affected.
Treatment of allograft rejection: Increased doses of tacrolimus, supplemental corticosteroid therapy, and introduction of short courses of mono-/polyclonal antibodies have all been used to manage rejection episodes. If signs of toxicity such as severe adverse reactions are noted (see Adverse Reactions), the dose of tacrolimus monohydrate (Advagraf) may need to be reduced.
Treatment of allograft rejection after kidney or liver transplantation: For conversion from other immunosuppressants to once daily tacrolimus monohydrate (Advagraf), treatment should begin with the initial oral dose recommended in kidney and liver transplantation respectively for prophylaxis of transplant rejection.
Treatment of allograft rejection after heart transplantation: In adult patients converted to tacrolimus monohydrate (Advagraf), an initial oral dose of 0.15 mg/kg/day should be administered once daily in the morning.
Treatment of allograft rejection after transplantation of other allografts: Although there is no clinical experience with tacrolimus monohydrate (Advagraf) in lung-, pancreas- or intestine-transplanted patients, Prograf has been used in lung-transplanted patients at an initial oral dose of 0.10-0.15 mg/kg/day, in pancreas-transplanted patients at an initial oral dose of 0.2 mg/kg/day and in intestinal transplantation at an initial oral dose of 0.3 mg/kg/day.
Dose adjustments in special populations: Hepatic impairment: Dose reduction may be necessary in patients with severe liver impairment in order to maintain the tacrolimus blood trough levels within the recommended target range.
Renal impairment: As the pharmacokinetics of tacrolimus are unaffected by renal function (see Pharmacology: Pharmacokinetics under Actions), no dose adjustment is required. However, owing to the nephrotoxic potential of tacrolimus careful monitoring of renal function is recommended (including serial serum creatinine concentrations, calculation of creatinine clearance and monitoring of urine output).
Race: In comparison to Caucasians, black patients may require higher tacrolimus doses to achieve similar trough levels.
Gender: There is no evidence that male and female patients require different doses to achieve similar trough levels.
Elderly patients: There is no evidence currently available to indicate that dosing should be adjusted in elderly patients.
Therapeutic drug monitoring: Dosing should primarily be based on clinical assessments of rejection and tolerability in each individual patient aided by whole blood tacrolimus trough level monitoring.
As an aid to optimise dosing, several immunoassays are available for determining tacrolimus concentrations in whole blood. Comparisons of concentrations from the published literature to individual values in clinical practice should be assessed with care and knowledge of the assay methods employed. In current clinical practice, whole blood levels are monitored using immunoassay methods. The relationship between tacrolimus trough levels (C24) and systemic exposure (AUC0-24) is similar between the two formulations Advagraf and Prograf.
Blood trough levels of tacrolimus should be monitored during the post-transplantation period. Tacrolimus blood trough levels should be determined approximately 24 hours post-dosing of Advagraf, just prior to the next dose. Frequent trough level monitoring in the initial two weeks post transplantation is recommended, followed by periodic monitoring during maintenance therapy. Blood trough levels of tacrolimus should also be closely monitored following conversion from Prograf to Advagraf, dose adjustments, changes in the immunosuppressive regimen, or co-administration of substances which may alter tacrolimus whole blood concentrations (see Interactions). The frequency of blood level monitoring should be based on clinical needs. As tacrolimus is a substance with low clearance, following adjustments to the Advagraf dose regimen it may take several days before the targeted steady state is achieved.
Data from clinical studies suggest that the majority of patients can be successfully managed if tacrolimus blood trough levels are maintained below 20 ng/ml. It is necessary to consider the clinical condition of the patient when interpreting whole blood levels. In clinical practice, whole blood trough levels have generally been in the range 5-20 ng/ml in liver transplant recipients and 10-20 ng/ml in kidney and heart transplant patients in the early post-transplant period. During subsequent maintenance therapy, blood concentrations have generally been in the range of 5-15 ng/ml in liver, kidney and heart transplant recipients.
Method of administration: Advagraf is a once-a-day oral formulation of tacrolimus. It is recommended that the oral daily dose of Advagraf be administered once daily in the morning. Tacrolimus monohydrate (Advagraf) prolonged-release hard capsules should be taken immediately following removal from the blister. Patients should be advised not to swallow the desiccant. The capsules should be swallowed whole with fluid (preferably water). Tacrolimus monohydrate (Advagraf) should generally be administered on an empty stomach or at least 1 hour before or 2 to 3 hours after a meal, to achieve maximal absorption (see Pharmacology: Pharmacokinetics under Actions). A forgotten morning dose should be taken as soon as possible on the same day. A double dose should not be taken on the next morning.
Experience with overdose is limited. Several cases of accidental overdose have been reported with tacrolimus; symptoms have included tremor, headache, nausea and vomiting, infections, urticaria, lethargy and increases in blood urea nitrogen, serum creatinine and alanine aminotransferase levels.
No specific antidote to tacrolimus therapy is available. If overdose occurs, general supportive measures and symptomatic treatment should be conducted.
Based on its high molecular weight, poor aqueous solubility, and extensive erythrocyte and plasma protein binding, it is anticipated that tacrolimus will not be dialysable. In isolated patients with very high plasma levels, haemofiltration or -diafiltration have been effective in reducing toxic concentrations. In cases of oral intoxication, gastric lavage and/or the use of adsorbents (such as activated charcoal) may be helpful, if used shortly after intake.
Hypersensitivity to tacrolimus, or to any of the excipients.
Hypersensitivity to other macrolides.
Medication errors, including inadvertent, unintentional or unsupervised substitution of immediate- or prolonged-release tacrolimus formulations, have been observed. This has led to serious adverse events, including graft rejection, or other side effects which could be a consequence of either under- or over-exposure to tacrolimus. Patients should be maintained on a single formulation of tacrolimus with the corresponding daily dosing regimen; alterations in formulation or regimen should only take place under the close supervision of a transplant specialist (see Dosage & Administration and Adverse Reactions).
Advagraf is not recommended for use in children below 18 years due to limited data on safety and/or efficacy.
For treatment of allograft rejection resistant to treatment with other immunosuppressive medicinal products in adult patients clinical data are not yet available for the prolonged-release formulation Advagraf.
For prophylaxis of transplant rejection in adult heart allograft recipients clinical data are not yet available for tacrolimus monohydrate (Advagraf).
During the initial post-transplant period, monitoring of the following parameters should be undertaken on a routine basis: blood pressure, ECG, neurological and visual status, fasting blood glucose levels, electrolytes (particularly potassium), liver and renal function tests, haematology parameters, coagulation values, and plasma protein determinations. If clinically relevant changes are seen, adjustments of the immunosuppressive regimen should be considered.
Substances with potential for interaction: Inhibitors or inducers of CYP3A4 should only be co-administered with tacrolimus after consulting a transplant specialist, due to the potential for drug interactions resulting in serious adverse reactions including rejection or toxicity (see Interactions).
CYP3A4 inhibitors: Concomitant use with CYP3A4 inhibitors may increase tacrolimus blood levels, which could lead to serious adverse reactions, including nephrotoxicity, neurotoxicity and QT prolongation. When concomitant use of strong CYP3A4 inhibitors (such as ritonavir, cobicistat, ketoconazole, itraconazole, posaconazole, voriconazole, telithromycin, clarithromycin or josamycin) with tacrolimus is required, tacrolimus blood levels should be monitored frequently, starting within the first few days of co-administration, under the supervision of a transplant specialist, to adjust the tacrolimus dose as appropriate in order to maintain similar tacrolimus exposure. Renal function, ECG including the QT interval, and the clinical condition of the patient should also be closely monitored.
Dose adjustment needs to be based upon the individual situation of each patient. An immediate dose reduction at the time of treatment initiation may be required (see Interactions).
Similarly, discontinuation of CYP3A4 inhibitors may affect the rate of metabolism of tacrolimus, thereby leading to subtherapeutic blood levels of tacrolimus, and therefore requires close monitoring and supervision of a transplant specialist.
CYP3A4 inducers: Concomitant use with CYP3A4 inducers may decrease tacrolimus blood levels, potentially increasing the risk of transplant rejection. When concomitant use of strong CYP3A4 inducers (such as rifampicin, phenytoin, carbamazepine) with tacrolimus is required, tacrolimus blood levels should be monitored frequently, starting within the first few days of co-administration, under the supervision of a transplant specialist, to adjust the tacrolimus dose if appropriate, in order to maintain similar tacrolimus exposure. Graft function should also be closely monitored (see Interactions).
Similarly, discontinuation of CYP3A4 inducers may affect the rate of metabolism of tacrolimus, thereby leading to supratherapeutic blood levels of tacrolimus, and therefore requires close monitoring and supervision of a transplant specialist.
Herbal preparations: Herbal preparations containing St. John's wort (Hypericum perforatum) should be avoided when taking Advagraf due to the risk of interactions that lead to a decrease in both blood concentrations and the therapeutic effect of tacrolimus (see Interactions).
Other interactions: The combined administration of ciclosporin and tacrolimus should be avoided and care should be taken when administering tacrolimus to patients who have previously received ciclosporin (see Dosage & Administration and Interactions).
High potassium intake or potassium-sparing diuretics should be avoided (see Interactions).
Certain combinations of tacrolimus with drugs known to have nephrotoxic or neurotoxic effects may increase the risk of these effects (see Interactions).
Vaccination: Immunosuppressants may affect the response to vaccination and vaccination during treatment with tacrolimus may be less effective. The use of live attenuated vaccines should be avoided.
Nephrotoxicity: Tacrolimus can result in renal function impairment in post-transplant patients. Acute renal impairment without active intervention may progress to chronic renal impairment. Patients with impaired renal function should be monitored closely as the dosage of tacrolimus may need to be reduced. The risk for nephrotoxicity may increase when tacrolimus is concomitantly administered with drugs associated with nephrotoxicity (see Interactions). When co-administration cannot be avoided, tacrolimus trough blood level and renal function should be monitored closely and dosage reduction should be considered if nephrotoxicity occurs.
Gastrointestinal disorder: Gastrointestinal perforation has been reported in patients treated with tacrolimus. As gastrointestinal perforation is a medically important event that may lead to a life-threatening or serious condition, adequate treatments should be considered immediately after suspected symptoms or signs occur.
Since levels of tacrolimus in blood may significantly change during diarrhoea episodes, extra monitoring of tacrolimus concentrations is recommended during episodes of diarrhoea.
Cardiac disorders: Ventricular hypertrophy or hypertrophy of the septum, reported as cardiomyopathies, have been observed in Prograf treated patients on rare occasions and may also occur with Advagraf. Most cases have been reversible, occurring with tacrolimus blood trough concentrations much higher than the recommended maximum levels. Other factors observed to increase the risk of these clinical conditions included pre-existing heart disease, corticosteroid usage, hypertension, renal or hepatic dysfunction, infections, fluid overload, and oedema. Accordingly, high-risk patients receiving substantial immunosuppression should be monitored, using such procedures as echocardiography or ECG pre- and post-transplant (e.g., initially at 3 months and then at 9-12 months). If abnormalities develop, dose reduction of Advagraf, or change of treatment to another immunosuppressive agent should be considered. Tacrolimus may prolong the QT interval and may cause Torsades de pointes. Caution should be exercised in patients with risk factors for QT prolongation, including patients with a personal or family history of QT prolongation, congestive heart failure, bradyarrhythmias and electrolyte abnormalities. Caution should also be exercised in patients diagnosed or suspected to have Congenital Long QT Syndrome or acquired QT prolongation or patients on concomitant medications known to prolong the QT interval, induce electrolyte abnormalities or known to increase tacrolimus exposure (see Interactions).
Lymphoproliferative disorders and malignancies: Patients treated with tacrolimus have been reported to develop EBV-associated lymphoproliferative disorders (see Adverse Reactions). A combination of immunosuppressives such as antilymphocytic antibodies (e.g., basiliximab, daclizumab) given concomitantly increases the risk of EBV-associated lymphoproliferative disorders. EBV-Viral Capsid Antigen (VCA)-negative patients have been reported to have an increased risk of developing lymphoproliferative disorders. Therefore, in this patient group, EBV-VCA serology should be ascertained before starting treatment with Advagraf. During treatment, careful monitoring with EBV-PCR is recommended. Positive EBV-PCR may persist for months and is per se not indicative of lymphoproliferative disease or lymphoma.
As with other potent immunosuppressive compounds, the risk of secondary cancer is unknown (see Adverse Reactions).
As with other immunosuppressive agents, owing to the potential risk of malignant skin changes, exposure to sunlight and UV light should be limited by wearing protective clothing and using a sunscreen with a high protection factor.
Opportunistic infections: Patients treated with immunosuppressants, including Tacrolimus monohydrate (Advagraf) are at increased risk for opportunistic infections (bacterial, fungal, viral and protozoal) such as CMV infection, BK virus associated nephropathy and JC virus associated progressive multifocal leukoencephalopathy (PML). These infections are often related to a high total immunosuppressive burden and may lead to serious or fatal conditions including graft rejection that physicians should consider in the differential diagnosis in immunosuppressed patients with deteriorating renal function or neurological symptoms.
Posterior reversible encephalopathy syndrome (PRES): Patients treated with tacrolimus have been reported to develop posterior reversible encephalopathy syndrome (PRES). If patients taking tacrolimus present with symptoms indicating PRES such as headache, altered mental status, seizures, and visual disturbances, a radiological procedure (e.g., MRI) should be performed. If PRES is diagnosed, adequate blood pressure and seizure control and immediate discontinuation of systemic tacrolimus is advised. Most patients completely recover after appropriate measures are taken.
Thrombotic microangiopathy (TMA) (including haemolytic uraemic syndrome (HUS) and thrombotic thrombocytopaenic purpura (TTP)): The diagnosis of TMA, including thrombotic thrombocytopaenic purpura (TTP) and haemolytic uraemic syndrome (HUS), sometimes leading to renal failure or a fatal outcome, should be considered in patients presenting with haemolytic anaemia, thrombocytopenia, fatigue, fluctuating neurological manifestation, renal impairment, and fever.
The concomitant administration of tacrolimus with a mammalian target of rapamycin (mTOR) inhibitor (e.g., sirolimus, everolimus) may increase the risk of thrombotic microangiopathy (including haemolytic uraemic syndrome and thrombotic thrombocytopaenic purpura).
Pure Red Cell Aplasia: Cases of pure red cell aplasia (PRCA) have been reported in patients treated with tacrolimus. All patients reported risk factors for PRCA such as parvovirus B19 infection, underlying disease or concomitant medications associated with PRCA.
Special populations: There is limited experience in non-Caucasian patients and patients at elevated immunological risk (e.g., retransplantation, evidence of panel reactive antibodies, PRA).
Dose reduction may be necessary in patients with severe liver impairment (see Dosage & Administration).
Excipients: As tacrolimus monohydrate (Advagraf) capsules contain lactose, patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
The printing ink used to mark Tacrolimus monohydrate (Advagraf) capsules contains soya lecithin. In patients who are hypersensitive to peanut or soya, the risk and severity of hypersensitivity should be weighed against the benefit of using Tacrolimus monohydrate (Advagraf). This medicine contains less than 1 mmol sodium (23 mg) per capsule, that is to say essentially 'sodium-free'.
Effects on ability to drive and use machines: Tacrolimus may cause visual and neurological disturbances. This effect may be enhanced if Tacrolimus monohydrate (Advagraf) is administered in association with alcohol.
No studies on the effects of Tacrolimus monohydrate (Advagraf) on the ability to drive and use machines have been performed.
Pregnancy: Human data show that tacrolimus crosses the placenta and infants exposed to tacrolimus in utero may be at a risk of prematurity, birth defects/congenital anomalies, low birth weight, and foetal distress.
The use of tacrolimus during pregnancy has been associated with preterm delivery, neonatal hyperkalaemia and renal dysfunction.
Tacrolimus may increase hyperglycaemia in pregnant women with diabetes (including gestational diabetes). Monitor maternal blood glucose levels regularly.
Tacrolimus may exacerbate hypertension in pregnant women and increase pre-eclampsia. Monitor and control blood pressure.
Females and males of reproductive potential should consider the use of appropriate contraception prior to starting treatment with tacrolimus.
Tacrolimus treatment can be considered in pregnant women, when there is no safer alternative and when the perceived benefit justifies the potential risk to the foetus.
In rats and rabbits, tacrolimus caused embryofoetal toxicity at doses which demonstrated maternal toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Lactation: Human data demonstrate that tacrolimus is excreted in breast milk. The effects of tacrolimus on the breastfed infant, or on milk production have not been assessed. As detrimental effects on the newborn cannot be excluded, women should not breast-feed whilst receiving tacrolimus.
Fertility: A negative effect of tacrolimus on male fertility in the form of reduced sperm counts and motility was observed in rats (see Pharmacology: Toxicology: Preclinical safety data under Actions).
The adverse reaction profile associated with immunosuppressive agents is often difficult to establish owing to the underlying disease and the concurrent use of multiple medicinal products.
The most commonly reported adverse drug reactions (occurring in >10% of patients) are tremor, renal impairment, hyperglycaemic conditions, diabetes mellitus, hyperkalaemia, infections, hypertension and insomnia.
Many of the adverse reactions stated as follows are reversible and/or respond to dose reduction. The frequency of adverse reactions is defined as follows: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. (See Tables 2a and 2b.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Metabolic interactions: Systemically available tacrolimus is metabolised by hepatic CYP3A4. There is also evidence of gastrointestinal metabolism by CYP3A4 in the intestinal wall. Concomitant use of medicinal products or herbal remedies known to inhibit or induce CYP3A4 may affect the metabolism of tacrolimus and thereby increase or decrease tacrolimus blood levels. Similarly, discontinuation of such products or herbal remedies may affect the rate of metabolism of tacrolimus and thereby the blood levels of tacrolimus.
Pharmacokinetics studies have indicated that the increase in tacrolimus blood levels when co-administered with inhibitors of CYP3A4 is mainly a result of increase in oral bioavailability of tacrolimus owing to the inhibition of gastrointestinal metabolism. Effect on hepatic clearance is less pronounced.
It is recommended strongly to closely monitor tacrolimus blood levels under supervision of a transplant specialist, as well as, monitor for graft function, QT prolongation (with ECG), renal function and other side effects, including neurotoxicity whenever substances which have the potential to alter CYP3A4 metabolism are used concomitantly, and to adjust or interrupt the tacrolimus dose if appropriate in order to maintain similar tacrolimus exposure (see Dosage & Administration and Precautions). Similarly, patients should be closely monitored when using tacrolimus concomitantly with multiple substances that affect CYP3A4 as the effects on tacrolimus exposure may be enhanced or counteracted.
Medicinal products which have effects on tacrolimus are listed in the table as follows. The examples of drug-drug interactions are not intended to be inclusive or comprehensive and therefore the label of each drug that is co-administered with tacrolimus should be consulted for information related to the route of metabolism, interaction pathways, potential risks, and specific actions to be taken with regards to co-administration. (See Table 3.)
Click on icon to see table/diagram/image
As tacrolimus treatment may be associated with hyperkalaemia, or may increase pre-existing hyperkalaemia, high potassium intake, or potassium-sparing diuretics (e.g. amiloride, triamterene, or spironolactone) should be avoided (see Precautions). Care should be taken when tacrolimus is co-administered with other agents that increase serum potassium, such as trimethoprim and cotrimoxazole (trimethoprim/sulfamethoxazole), as trimethoprim is known to act as a potassium-sparing diuretic like amiloride. Close monitoring of serum potassium is recommended.
Effect of tacrolimus on the metabolism of other medicinal products: Tacrolimus is a known CYP3A4 inhibitor; thus concomitant use of tacrolimus with medicinal products known to be metabolised by CYP3A4 may affect the metabolism of such medicinal products.
The half-life of ciclosporin is prolonged when tacrolimus is given concomitantly. In addition, synergistic/additive nephrotoxic effects can occur. For these reasons, the combined administration of ciclosporin and tacrolimus is not recommended and care should be taken when administering tacrolimus to patients who have previously received ciclosporin (see Dosage & Administration and Precautions).
Tacrolimus has been shown to increase the blood level of phenytoin.
As tacrolimus may reduce the clearance of steroid-based contraceptives leading to increased hormone exposure, particular care should be exercised when deciding upon contraceptive measures.
Limited knowledge of interactions between tacrolimus and statins is available. Clinical data suggest that the pharmacokinetics of statins are largely unaltered by the co-administration of tacrolimus.
Animal data have shown that tacrolimus could potentially decrease the clearance and increase the half-life of pentobarbital and antipyrine.
Mycophenolic acid. Caution should be exercised when switching combination therapy from ciclosporin, which interferes with enterohepatic recirculation of mycophenolic acid, to tacrolimus, which is devoid of this effect, as this might result in changes of mycophenolic acid exposure. Drugs which interfere with mycophenolic acid's enterohepatic cycle have potential to reduce the plasma level and efficacy of mycophenolic acid. Therapeutic drug monitoring of mycophenolic acid may be appropriate when switching from ciclosporin to tacrolimus or vice versa.
Immunosuppressants may affect the response to vaccination and vaccination during treatment with tacrolimus may be less effective. The use of live attenuated vaccines should be avoided (see Precautions).
Incompatibilities: Tacrolimus is not compatible with PVC (polyvinylchloride). Tubing, syringes and other equipment used to prepare a suspension of Advagraf capsule contents must not contain PVC.
Special precaution for disposal: Based on immunosuppressive effects of tacrolimus, inhalation or direct contact with skin or mucous membranes by the formulations for powder contained in tacrolimus products should be avoided during preparation. If such contact occurs, wash the skin and flush the affected eye or eyes.
Store at temperatures not exceeding 30°C.
Shelf life: 3 years.
Special precautions for storage: Store in the original package in order to protect from moisture.
L04AD02 - tacrolimus ; Belongs to the class of calcineurin inhibitors. Used as immunosuppressants.
Advagraf PR cap 1 mg
50's
Advagraf PR cap 5 mg
50's
Advagraf PR cap 500 mcg
50's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image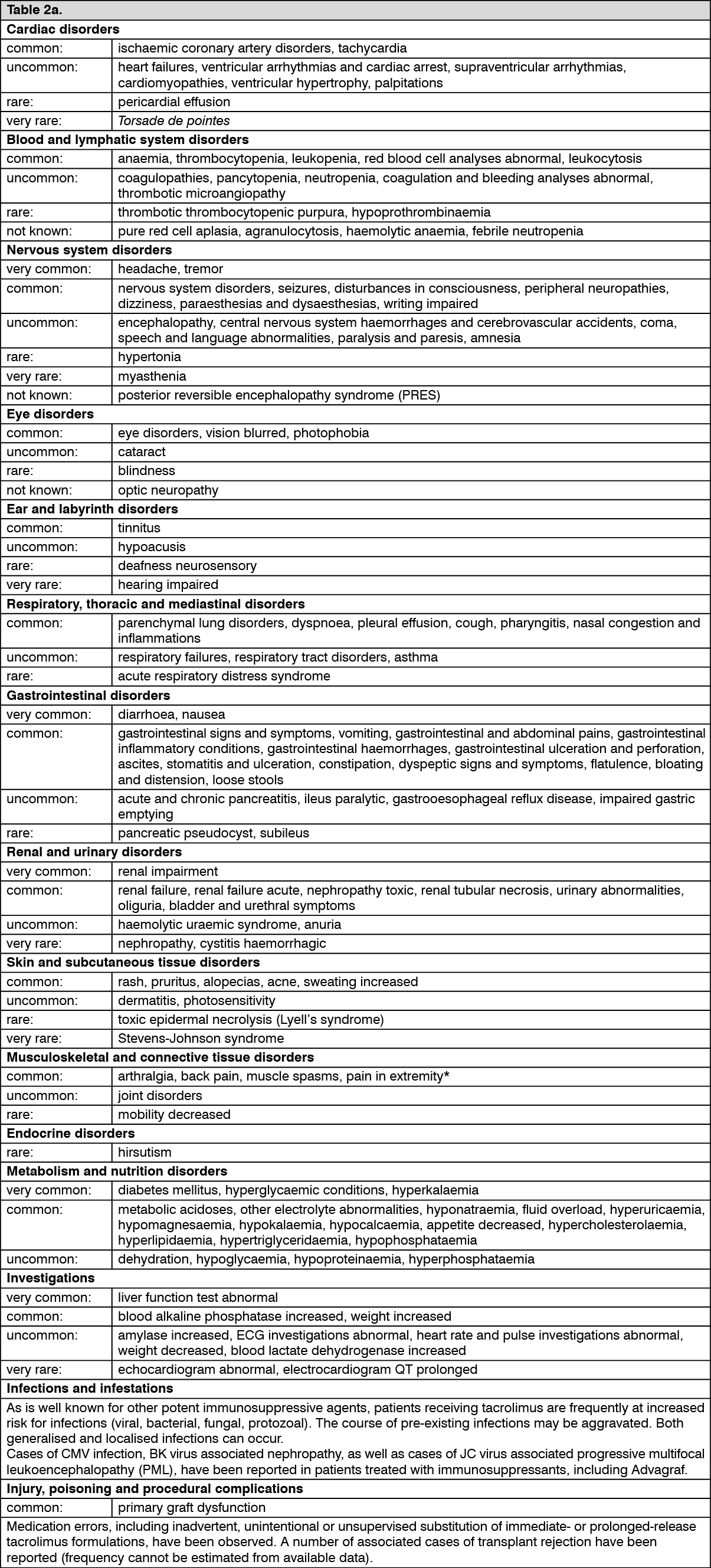 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image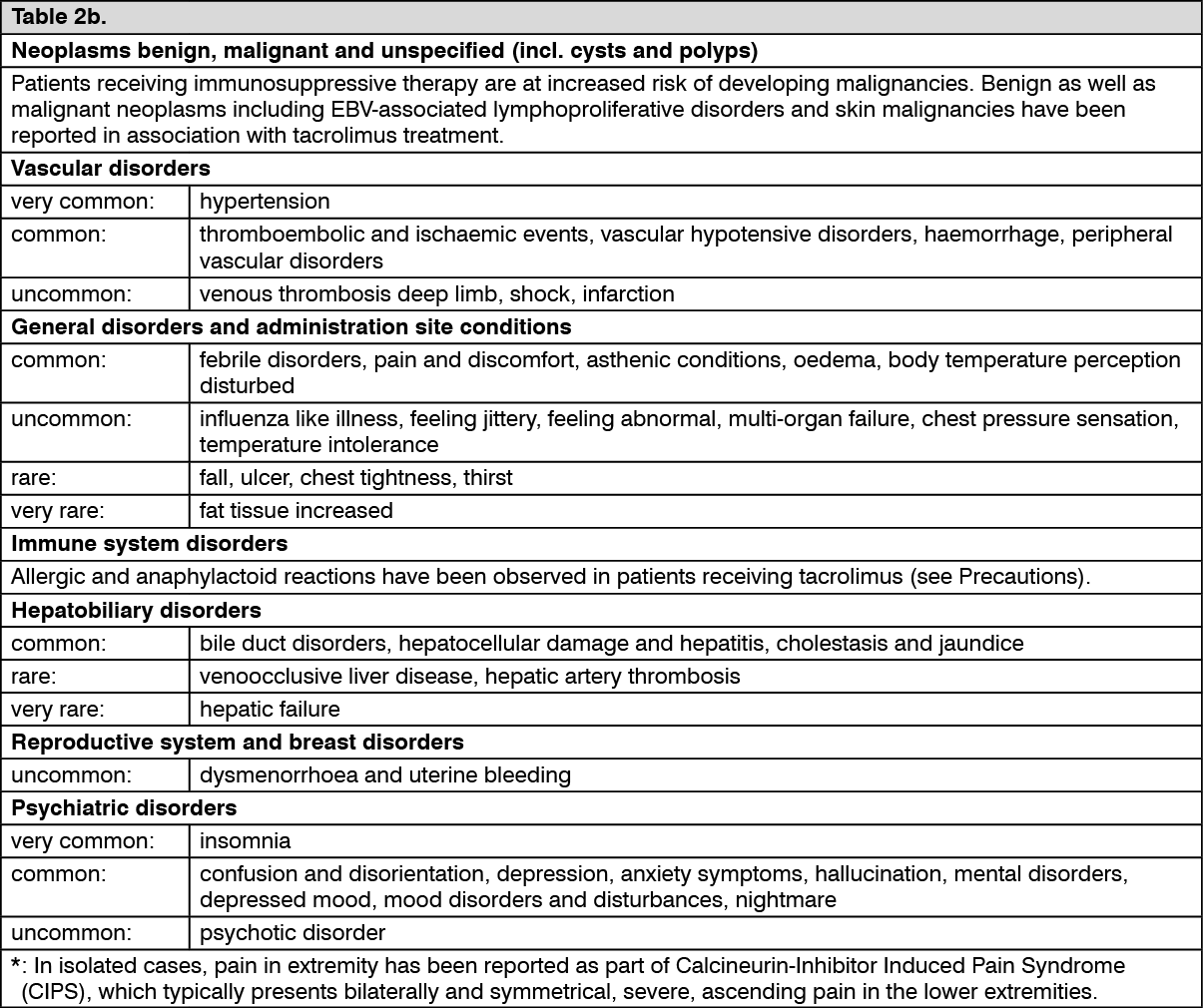 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image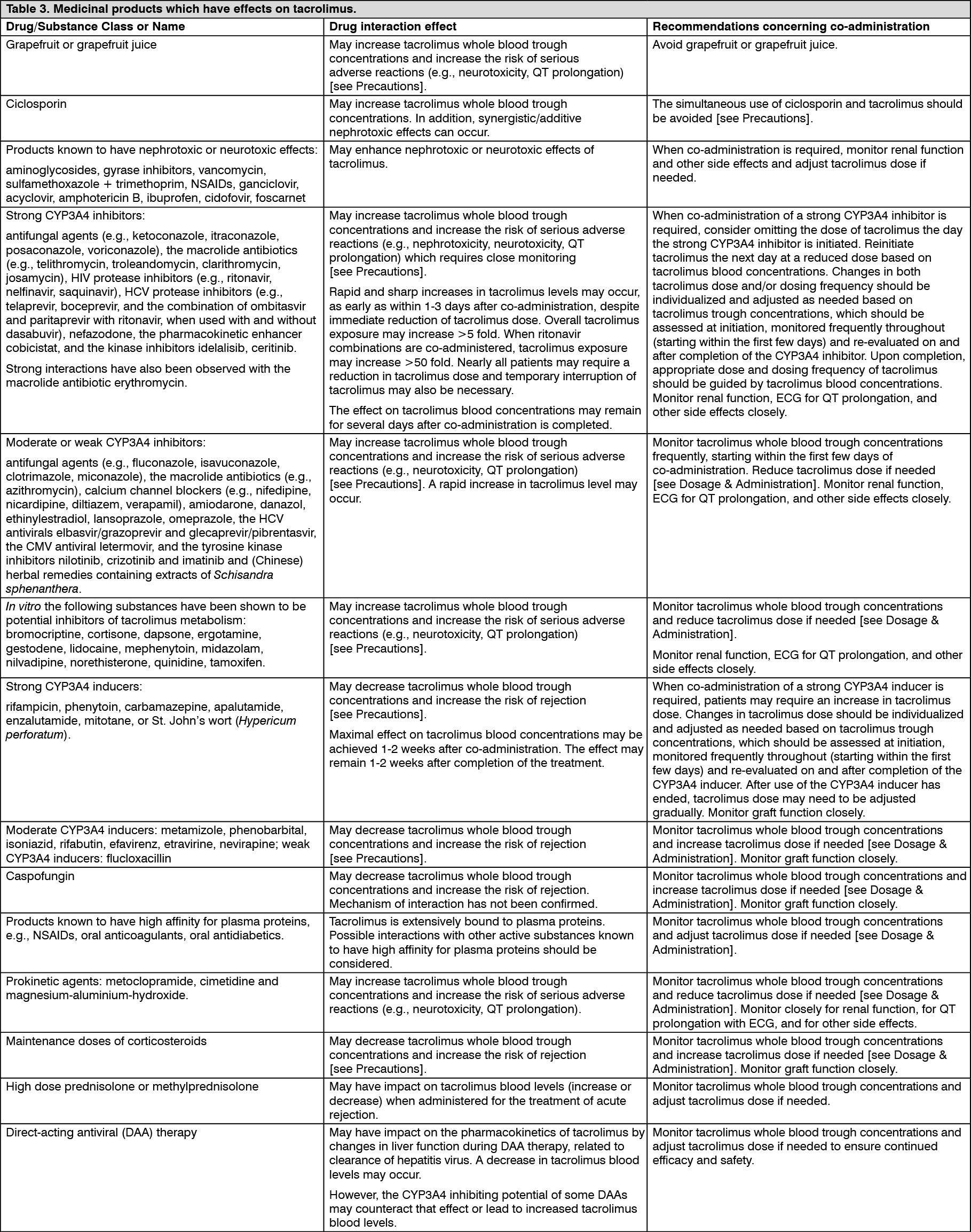 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
