Treatment must be initiated and administered under the supervision of a physician qualified and experienced in the use of chemotherapeutic agents. Bortezomib for injection must be reconstituted by a healthcare professional.
Posology for treatment of progressive multiple myeloma (patients who have received at least one prior therapy): Monotherapy: Bortezomib for injection 3.5 mg powder for solution for injection is administered via intravenous or subcutaneous injection at the recommended dose of 1.3 mg/m
2 body surface area twice weekly for two weeks on days 1, 4, 8, and 11 in a 21-day treatment cycle. This 3-week period is considered a treatment cycle. It is recommended that patients receive 2 cycles of Bortezomib for injection following a confirmation of a complete response. It is also recommended that responding patients who do not achieve a complete remission receive a total of 8 cycles of Bortezomib for injection therapy. At least 72 hours should elapse between consecutive doses of Bortezomib for injection.
Dose adjustments during treatment and re-initiation of treatment for monotherapy: Bortezomib for injection treatment must be withheld at the onset of any Grade 3 non-haematological or any Grade 4 haematological toxicities, excluding neuropathy as discussed as follows. Once the symptoms of the toxicity have resolved, Bortezomib for injection treatment may be re-initiated at a 25% reduced dose (1.3 mg/m
2 reduced to 1.0 mg/m
2; 1.0 mg/m
2 reduced to 0.7 mg/m
2). If the toxicity is not resolved or if it recurs at the lowest dose, discontinuation of Bortezomib for injection must be considered unless the benefit of treatment clearly outweighs the risk.
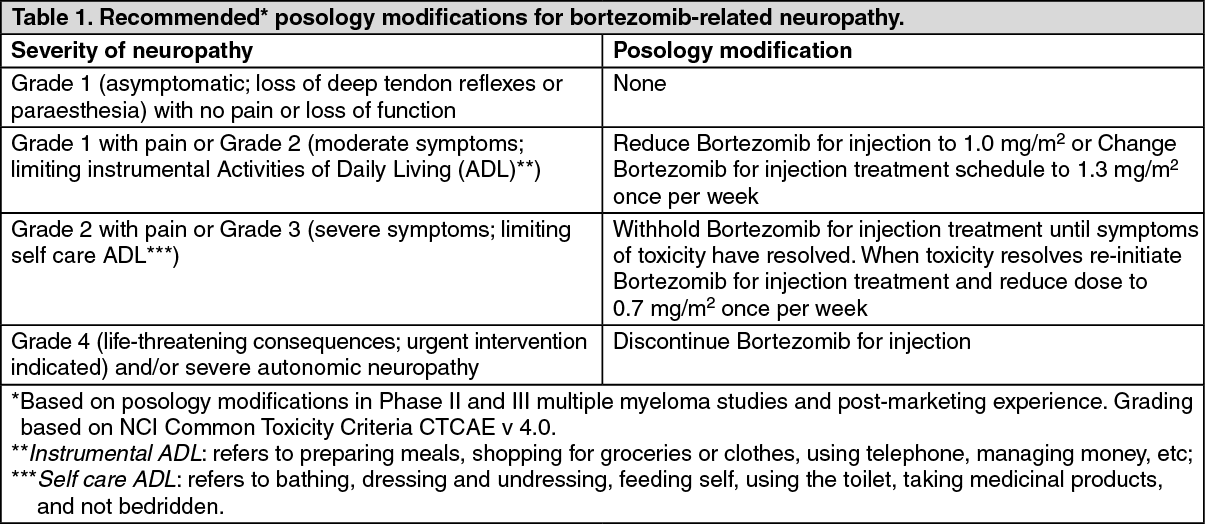
Neuropathic pain and/or peripheral neuropathy: Patients who experience bortezomib-related neuropathic pain and/or peripheral neuropathy are to be managed as presented in Table 1. Patients with pre-existing severe neuropathy may be treated with Bortezomib for injection only after careful risk/benefit assessment. (See Table 1.)
 Click on icon to see table/diagram/image
Combination therapy with pegylated liposomal doxorubicin:
Click on icon to see table/diagram/image
Combination therapy with pegylated liposomal doxorubicin: Bortezomib for injection 3.5 mg powder for solution for injection is administered via intravenous or subcutaneous injection at the recommended dose of 1.3 mg/m
2 body surface area twice weekly for two weeks on days 1, 4, 8, and 11 in a 21-day treatment cycle. This 3-week period is considered a treatment cycle. At least 72 hours should elapse between consecutive doses of Bortezomib for injection.
Pegylated liposomal doxorubicin is administered at 30 mg/m
2 on day 4 of the Bortezomib for injection treatment cycle as a 1 hour intravenous infusion administered after the Bortezomib for injection.
Up to 8 cycles of this combination therapy can be administered as long as patients have not progressed and tolerate treatment. Patients achieving a complete response can continue treatment for at least 2 cycles after the first evidence of complete response, even if this requires treatment for more than 8 cycles. Patients whose levels of paraprotein continue to decrease after 8 cycles can also continue for as long as treatment is tolerated and they continue to respond.
Combination with dexamethasone: Bortezomib for injection 3.5 mg powder for solution for injection is administered via intravenous or subcutaneous injection at the recommended dose of 1.3 mg/m
2 body surface area twice weekly for two weeks on days 1, 4, 8, and 11 in a 21-day treatment cycle. This 3-week period is considered a treatment cycle. At least 72 hours should elapse between consecutive doses of Bortezomib for injection.
Dexamethasone is administered orally at 20 mg on days 1, 2, 4, 5, 8, 9, 11, and 12 of the Bortezomib for injection treatment cycle.
Patients achieving a response or a stable disease after 4 cycles of this combination therapy can continue to receive the same combination for a maximum of 4 additional cycles.
Dose adjustments for combination therapy for patients with progressive multiple myeloma: For Bortezomib for injection dosage adjustments for combination therapy follow dose modification guidelines described under monotherapy previously.
Posology for previously untreated multiple myeloma patients not eligible for haematopoietic stem cell transplantation: Combination therapy with melphalan and prednisone: Bortezomib for injection 3.5 mg powder for solution for injection is administered via intravenous or subcutaneous injection in combination with oral melphalan and oral prednisone as shown in Table 2. A 6-week period is considered a treatment cycle. In Cycles 1-4, Bortezomib for injection is administered twice weekly on days 1, 4, 8, 11, 22, 25, 29 and 32. In Cycles 5-9, Bortezomib for injection is administered once weekly on days 1, 8, 22 and 29. At least 72 hours should elapse between consecutive doses of Bortezomib for injection.
Melphalan and prednisone should both be given orally on days 1, 2, 3 and 4 of the first week of each Bortezomib for injection treatment cycle. Nine treatment cycles of this combination therapy are administered. (See Table 2.)
Click on icon to see table/diagram/image
Dose adjustments during treatment and re-initiation of treatment for combination therapy with melphalan and prednisone: Prior to initiating a new cycle of therapy: Platelet counts should be ≥70 x 109/L and the absolute neutrophils count should be ≥1.0 x 109/L; Non-haematological toxicities should have resolved to Grade 1 or baseline. (See Table 3.)
Click on icon to see table/diagram/image
Posology for previously untreated multiple myeloma patients eligible for haematopoietic stem cell transplantation (induction therapy): Combination therapy with dexamethasone: Bortezomib for injection 3.5 mg powder for solution for injection is administered via intravenous or subcutaneous injection at the recommended dose of 1.3 mg/m
2 body surface area twice weekly for two weeks on days 1, 4, 8, and 11 in a 21-day treatment cycle. This 3-week period is considered a treatment cycle. At least 72 hours should elapse between consecutive doses of Bortezomib for injection.
Dexamethasone is administered orally at 40 mg on days 1, 2, 3, 4, 8, 9, 10 and 11 of the Bortezomib for injection treatment cycle. Four treatment cycles of this combination therapy are administered.
Combination therapy with dexamethasone and thalidomide: Bortezomib for injection 3.5 mg powder for solution for injection is administered via intravenous or subcutaneous injection at the recommended dose of 1.3 mg/m
2 body surface area twice weekly for two weeks on days 1, 4, 8, and 11 in a 28-day treatment cycle. This 4-week period is considered a treatment cycle. At least 72 hours should elapse between consecutive doses of Bortezomib for injection.
Dexamethasone is administered orally at 40 mg on days 1, 2, 3, 4, 8, 9, 10 and 11 of the Bortezomib for injection treatment cycle.
Thalidomide is administered orally at 50 mg daily on days 1-14 and if tolerated the dose is increased to 100 mg on days 15-28, and thereafter may be further increased to 200 mg daily from cycle 2 (see Table 4).
Four treatment cycles of this combination are administered. It is recommended that patients with at least partial response receive 2 additional cycles. (See Table 4).
Click on icon to see table/diagram/image
Dosage adjustments for transplant eligible patients: For Bortezomib for injection dosage adjustments for neuropathy refer to Table 1.
In addition, when Bortezomib for injection is given in combination with other chemotherapeutic medicinal products, appropriate dose reductions for these products should be considered in the event of toxicities according to the recommendations.
Special populations:
Elderly: There is no evidence to suggest that dose adjustments are necessary in patients over 65 years of age.
There are no studies on the use of Bortezomib for injection in elderly patients with previously untreated multiple myeloma who are eligible for high-dose chemotherapy with haematopoietic stem cell transplantation. Therefore no dose recommendations can be made in this population.
Hepatic impairment: Patients with mild hepatic impairment do not require a dose adjustment and should be treated per the recommended dose. Patients with moderate or severe hepatic impairment should be started on Bortezomib for injection at a reduced dose of 0.7 mg/m
2 per injection during the first treatment cycle, and a subsequent dose escalation to 1.0 mg/m
2 or further dose reduction to 0.5 mg/m
2 may be considered based on patient tolerability. (See Table 5.)
Click on icon to see table/diagram/image
Renal impairment: The pharmacokinetics of bortezomib are not influenced in patients with mild to moderate renal impairment (Creatinine Clearance [CrCl] >20 mL/min/1.73 m
2); therefore, dose adjustments are not necessary for these patients. It is unknown if the pharmacokinetics of bortezomib are influenced in patients with severe renal impairment not undergoing dialysis (CrCl <20 mL/min/1.73 m
2). Since dialysis may reduce bortezomib concentrations, Bortezomib for injection should be administered after the dialysis procedure.
Paediatric population: The safety and efficacy of Bortezomib for injection in children below 18 years of age have not been established. No data are available.
Method of administration: Bortezomib for injection 3.5 mg powder for solution for injection is available for intravenous or subcutaneous administration. Bortezomib for injection 1 mg powder for solution for injection is available for intravenous administration only.
Bortezomib for injection should not be given by other routes. Intrathecal administration has resulted in death.
Intravenous injection: Bortezomib for injection 3.5 mg reconstituted solution is administered as a 3-5 second bolus intravenous injection through a peripheral or central intravenous catheter followed by a flush with sodium chloride 9 mg/mL (0.9%) solution for injection. At least 72 hours should elapse between consecutive doses of Bortezomib for injection.
Subcutaneous injection: Bortezomib for injection 3.5 mg reconstituted solution is administered subcutaneously through the thighs (right or left) or abdomen (right or left). The solution should be injected subcutaneously, at a 45-90° angle. Injection sites should be rotated for successive injections.
If local injection site reactions occur following Bortezomib for injection subcutaneous injection, either a less concentrated Bortezomib for injection solution (Bortezomib for injection 3.5 mg to be reconstituted to 1 mg/mL instead of 2.5 mg/mL) may be administered subcutaneously or a switch to intravenous injection is recommended.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image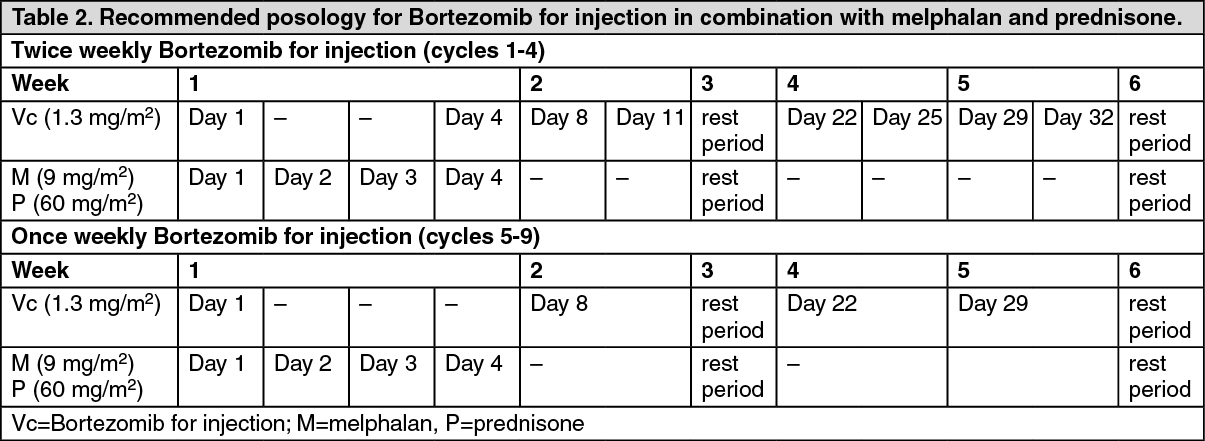 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image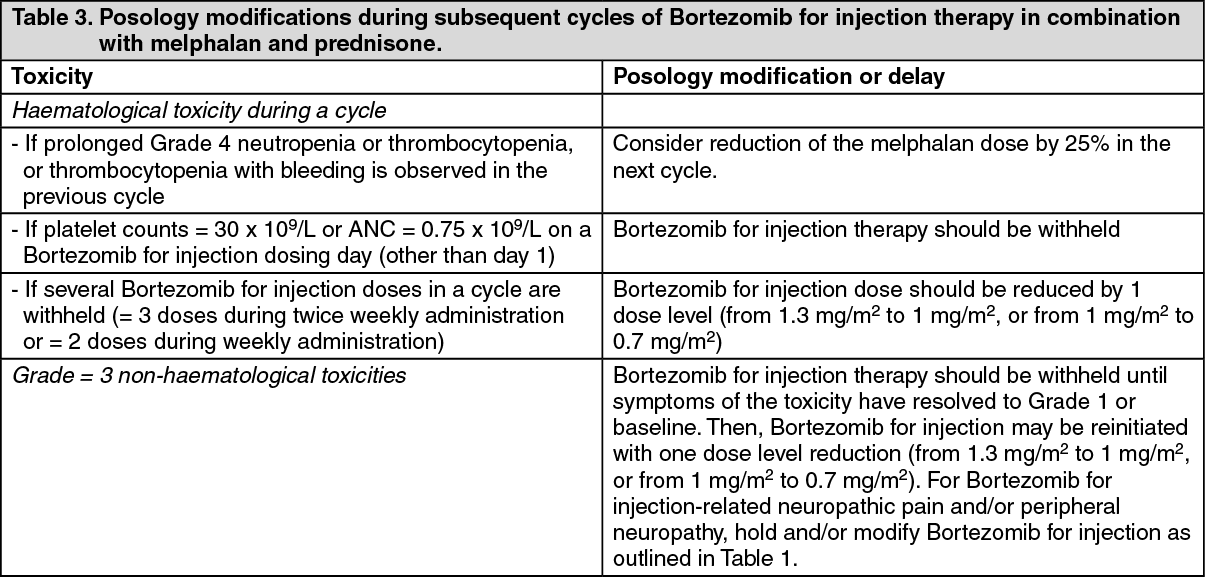 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image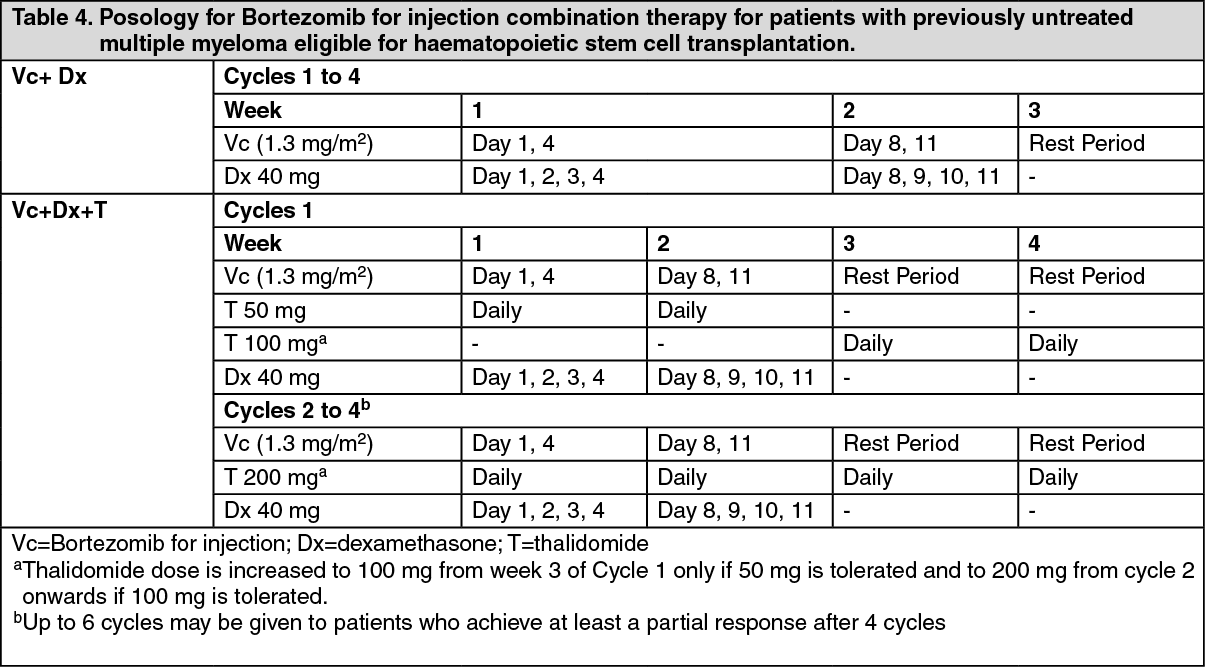 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image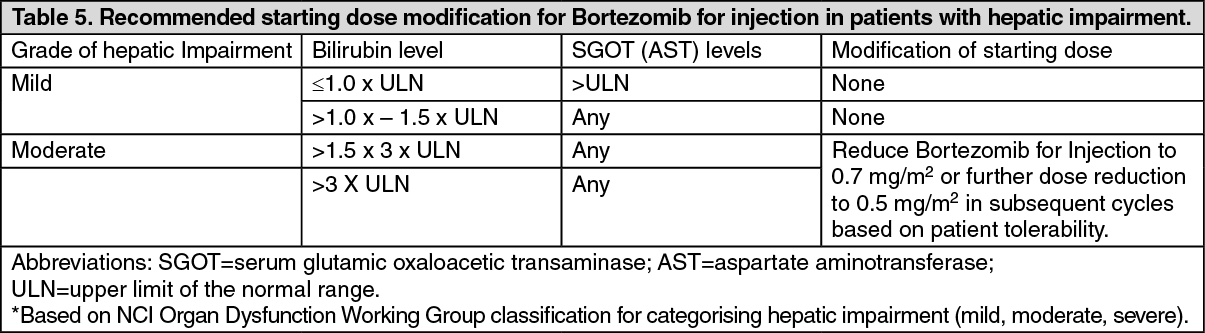 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
