Vortioxetine hydrobromide.
Each film-coated tablet contains 5 mg Vortioxetine (as 6.355 mg Vortioxetine hydrobromide).
Each film-coated tablet contains 10 mg Vortioxetine (as 12.710 mg Vortioxetine hydrobromide).
Each film-coated tablet contains 15 mg Vortioxetine (as 19.065 mg Vortioxetine hydrobromide).
Excipients/Inactive Ingredients: 5 mg: Tablet core: Mannitol, Microcystalline cellulose, Hydroxypropylcellulose, Sodium starch glycolate (type A), Magnesium stearate.
Tablet coating: Hypromellose, Macrogol 400, Titanium dioxide (E171), Iron oxide red (E172).
10 mg tablets:Tablet core: Mannitol, Microcystalline cellulose, Hydroxypropylcellulose, Sodium starch glycolate (type A), Magnesium stearate.
Tablet coating: Hypromellose, Macrogol 400, Titanium dioxide (E171), Iron oxide yellow (E172).
15 mg tablets: Tablet core: Mannitol, Microcystalline cellulose, Hydroxypropylcellulose, Sodium starch glycolate (type A), Magnesium stearate.
Tablet coating: Hypromellose, Macrogol 400, Titanium dioxide (E171), Iron oxide red (E172), Iron oxide yellow (E172).
Pharmacotherapeutic Group: Other antidepressants. ATC Code: N06AX26.
Pharmacology: Pharmacodynamics: Mechanism of action: The mechanism of action of vortioxetine is thought to be related to its direct modulation of serotonergic receptor activity and inhibition of the serotonin (5-HT) transporter. Non-clinical data indicate that vortioxetine is a 5-HT3, 5-HT7, and 5-HT1D receptor antagonist, 5-HT1B receptor partial agonist, 5-HT1A receptor agonist and inhibitor of the 5-HT transporter, leading to modulation of neurotransmission in several systems, including the serotonin, norepinephrine, dopamine, histamine, acetylcholine, GABA and glutamate systems. This multimodal activity is considered responsible for the antidepressant and anxiolytic-like effects and the improvement of cognitive function, learning and memory observed with vortioxetine in animal studies. In addition, a nonclinical behavioural study in male animals indicates that vortioxetine does not induce sexual dysfunction. However, the precise contribution of the individual targets to the observed pharmacodynamic profile remains unclear and caution should be applied when extrapolating animal data directly to man.
In humans, two positron emission tomography (PET) studies have been conducted using 5-HT transporter ligands (11C-MADAM or 11C-DASB) to quantify the 5-HT transporter occupancy in the brain across different dose levels. The mean 5-HT transporter occupancy in the specific regions of interest was approximately 50% at 5 mg/day, 65% at 10 mg/day and increased to above 80% at 20 mg/day.
Vortioxetine has shown clinical antidepressant effects at 5-HT transporter occupancies as low as 50%.
Clinical efficacy and safety: The efficacy and safety of vortioxetine have been studied in a clinical programme that included more than 6,700 patients, of whom more than 3,700 were treated with vortioxetine in short-term (≤12 weeks) studies in major depressive disorder (MDD). Twelve double-blind, placebo controlled, 6/8-week, fixed-dose studies have been conducted to investigate the short-term efficacy of vortioxetine in MDD both in adults and in the elderly. The efficacy of vortioxetine was demonstrated across 9 of the 12 studies, as measured by improvement in the Montgomery and Åsberg Depression Rating Scale (MADRS) or Hamilton Depression Rating Scale 24-item (HAM-D24) total score, and supported by clinical relevance as demonstrated by the proportions of responders and remitters and the improvement in Clinical Global Impression - Global Improvement (CGI-I) score. The efficacy of vortioxetine increased with increasing dose.
Furthermore, vortioxetine, in the dose range of 5-20 mg/day, demonstrated efficacy on the broad range of depressive symptoms (assessed by improvement in all MADRS single-item scores) and on the anxiety symptoms in depression (assessed using the HAM-A total score).
Maintenance: The maintenance of antidepressant efficacy was demonstrated in a relapse-prevention study. Patients in remission after an initial 12-week open-label treatment period with vortioxetine were randomised to vortioxetine 5 or 10 mg/day or placebo and observed for relapse during a double-blind period of at least 24 weeks (24 to 64 weeks). Vortioxetine was superior (p=0.004) to placebo on the primary outcome measure, the time to relapse of MDD, with a hazard ratio of 2.0; that is, the risk of relapse was two times higher in the placebo group than in the vortioxetine group.
Elderly: In the double-blind, placebo-controlled, 8-week, fixed-dose study in elderly (aged ≥65 years) depressed patients, vortioxetine 5 mg/day was superior to placebo as measured by improvement in the MADRS and HAM-D24 total scores.
In the dose range of 5 to 20 mg/day vortioxetine, efficacy and tolerability in the elderly was in line with the results in the adult population.
Patients with severe depression or high levels of anxiety symptoms: Antidepressant efficacy was also demonstrated in severely depressed patients (baseline MADRS total score ≥30) and in depressed patients with a high level of anxiety symptoms (baseline HAM-A total score ≥20) in short-term studies including the study in the elderly and in the long-term relapse-prevention study.
Effects of vortioxetine on the Digit Symbol Substitution Test (DSST), the University of California San Diego Performance-Based Skills Assessment (UPSA) (objective measures) and Perceived Deficits Questionnaire (PDQ) and Cognitive and Physical Functioning Questionnaire CPFQ (subjective measures) scores: The efficacy of vortioxetine (5-20 mg/day) in patients with MDD has been investigated in 2 adult and 1 elderly short-term, placebo-controlled studies.
Vortioxetine had a statistically significant effect versus placebo on the Digit Symbol Substitution Test (DSST), ranging from Δ = 1.75 (p = 0.019) to 4.26 (p <0.0001) in the 2 studies in adults and Δ = 2.79 (p = 0.023) in the study in the elderly. In the meta-analyses (ANCOVA, LOCF) of the mean change from baseline in DSST number of correct symbols in all 3 studies, vortioxetine separated from placebo (p<0.05) with a standardised effect size of 0.35. When adjusting for the change in MADRS the total score in the meta-analysis of the same studies showed that vortioxetine separated from placebo (p<0.05) with a standardised effect size of 0.24.
One study assessed the effect of vortioxetine on functional capacity using the University of California San Diego Performance-Based Skills Assessment (UPSA). Vortioxetine separated from placebo statistically with results of 8.0 for vortioxetine versus 5.1 points for placebo (p=0.0003).
In one study, vortioxetine was superior to placebo on subjective measures, evaluated using the Perceived Deficits Questionnaire with results of -14.6 for vortioxetine and -10.5 for placebo (p=0.002).
Vortioxetine did not separate from placebo on subjective measures when evaluated using the Cognitive and Physical Functioning Questionnaire with results of -8.1 for vortioxetine versus -6.9 for placebo (p=0.086).
Patients with inadequate response to SSRI/SNRI treatment: In a 12-week, double-blind, flexible-dose, comparative study in patients with moderate to severe depression who switched antidepressant treatment after an inadequate response to an SSRI/SNRI for the current episode vortioxetine 10-20 mg/day was statistically significantly better than agomelatine 25-50 mg/day as measured by improvement in the MADRS total score. The clinical relevance was supported by the proportion of remitters and improvement in CGI-I and Sheehan Disability Scale (SDS) scores.
Health-related quality of life and overall functioning: Vortioxetine was superior to placebo in health-related quality of life, as assessed using the SF-36 Mental Component Summary and the Quality of Life Enjoyment Satisfaction Questionnaire total and life satisfaction scores. This was supported by clinically relevant improvements in the overall health rating as measured using EQ-5D (EuroQol index) and in the overall functioning as assessed using the Sheehan Disability Scale (SDS) total score in the areas of work, social life, and family life versus placebo or an active comparator (agomelatine). Furthermore, the superior effects relative to placebo in health related quality of life were maintained in the long-term relapse prevention study.
Tolerability and safety: The safety and tolerability of vortioxetine have been established in short- and long-term studies across the dose range of 5 to 20 mg/day. For information on undesirable effects, see Adverse Reactions.
Vortioxetine did not increase the incidence of insomnia or somnolence relative to placebo.
In clinical short- and long-term placebo-controlled studies, potential discontinuation symptoms were systematically evaluated after abrupt treatment cessation of vortioxetine.
There was no clinically relevant difference to placebo in the incidence or nature of the discontinuation symptoms after either short-term (6-12 weeks) or long-term (24-64 weeks) treatment with vortioxetine.
The incidence of self-reported adverse sexual reactions was low and similar to placebo in clinical short- and long-term studies with vortioxetine. In studies using the Arizona Sexual Experience Scale (ASEX), the incidence of treatment-emergent sexual dysfunction (TESD) and the ASEX total score showed no significant difference to placebo in symptoms of sexual dysfunction for doses 5-20 mg/day, however higher doses were associated with a numerical increase in TESD.
Vortioxetine had no effect relative to placebo on body weight, heart rate, or blood pressure in clinical short- and long-term studies.
No clinically significant changes were observed in hepatic and renal assessments in clinical studies.
Vortioxetine has not shown any clinically significant effect on ECG parameters, including the QT, QTc, PR and QRS intervals, in patients with MDD. In a thorough QTc study in healthy subjects at doses up to 40 mg daily, no potential for the prolongation of the QTc interval was observed.
Paediatric population: Clinical studies on the use of Brintellix (Vortioxetine hydrobromide) in children and adolescents have not been conducted; therefore, the safety and efficacy of Brintellix (Vortioxetine hydrobromide) (see Dosage & Administration). in the paediatric population have not been established.
Pharmacokinetics: Absorption: Vortioxetine is slowly but well absorbed after oral administration and the peak plasma concentration is reached within 7 to 11 hours. Following multiple dosing of 5, 10, or 20 mg/day, mean Cmax values of 9 to 33 ng/mL were observed. The absolute bioavailability is 75%. No effect of food on the pharmacokinetics was observed (see Dosage & Administration).
Distribution: The mean volume of distribution (Vss) is 2,600 L, indicating extensive extravascular distribution. Vortioxetine is highly bound to plasma proteins (98 to 99%) and the binding appears to be independent of vortioxetine plasma concentrations.
Biotransformation: Vortioxetine is extensively metabolised in the liver, primarily through oxidation and subsequent glucuronic acid conjugation.
In vitro, the cytochrome P450 isozymes CYP2D6, CYP3A4/5, CYP2C19, CYP2C9, CYP2A6, CYP2C8, and CYP2B6 are involved in the metabolism of vortioxetine.
No inhibitory or inducing effect of vortioxetine was observed in vitro for the CYP isozymes CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1, or CYP3A4/5. Vortioxetine is a poor P-gp substrate and inhibitor.
The major metabolite of vortioxetine is pharmacologically inactive.
Elimination: The mean elimination half-life and oral clearance are 66 hours and 33 L/h, respectively. Approximately 2/3 of the inactive vortioxetine metabolites are excreted in the urine and approximately 1/3 in the faeces. Only negligible amounts of vortioxetine are excreted in the faeces. Steady-state plasma concentrations are achieved in approximately 2 weeks.
Linearity/non-linearity: The pharmacokinetics are linear and time independent in the dose range studied (2.5 to 60 mg/day).
In accordance with the half-life, the accumulation index is 5 to 6 based on AUC0-24h following multiple doses of 5 to 20 mg/day.
Special populations: Elderly: In elderly healthy subjects (aged ≥65 years; n=20), the exposure to vortioxetine increased up to 27% (Cmax and AUC) compared to young healthy control subjects (aged ≤45 years) after multiple doses of 10 mg/day. No dose adjustment is needed (see Dosage & Administration).
Renal impairment: Following a single dose of 10 mg vortioxetine, renal impairment estimated using the Cockcroft-Gault formula (mild, moderate, or severe; n=8 per group) caused modest exposure increases (up to 30%), compared to healthy matched controls. In patients with end-stage renal disease, only a small fraction of vortioxetine was lost during dialysis (AUC and Cmax were 13% and 27% lower; n=8) following a single 10 mg dose of vortioxetine. No dose adjustment is needed (see Precautions).
Hepatic impairment: Following a single dose of 10 mg vortioxetine, no impact of mild or moderate hepatic impairment (Child-Pugh Criteria A or B; n=8 per group) was observed on the pharmacokinetics of vortioxetine (changes in AUC were less than 10%). No dose adjustment is needed (see Dosage & Administration). Vortioxetine has not been studied in patients with severe hepatic impairment and caution should be exercised when treating these patients (see Precautions).
CYP2D6 poor metabolisers: The plasma concentration of vortioxetine was approximately two times higher in CYP2D6 poor metabolisers than in extensive metabolisers. In the presence of strong CYP3A4/2C9-inhibitors, the exposure could potentially be higher (see Interactions). Depending on individual patient response, a dose adjustment may be considered (see Dosage & Administration).
Toxicology: Preclinical safety data: Administration of vortioxetine in the general toxicity studies in mice, rats and dogs was mainly associated with CNS-related clinical signs. These included salivation (rat and dog), pupil dilatation (dog), and one episode of convulsions in each of two dogs. A no-effect level for convulsions was established with a corresponding safety margin of 5 considering the maximum recommended therapeutic dose of 20 mg/day. Target organ toxicity was restricted to kidneys (rats) and liver (mice and rats). The changes in the kidney in rats (glomerulonephritis, renal tubular obstruction, crystalline material in renal tubule) and in the liver of mice and rats (hepatocellular hypertrophy, hepatocyte necrosis, bile duct hyperplasia, crystalline material in bile ducts) were seen at exposures more than 10-fold (mice) and 2-fold (rats) the human exposure at the maximum recommended therapeutic dose of 20 mg/day. These findings were mainly attributed to rodent-specific vortioxetine-related crystalline material obstruction of the renal tubules and the bile ducts, respectively, and considered of low risk to humans.
Vortioxetine was not genotoxic in a standard battery of in vitro and in vivo tests.
Based on results from conventional 2-year carcinogenicity studies in mice or rats, vortioxetine is not considered to pose a risk of carcinogenicity in humans.
Vortioxetine had no effect on rat fertility, mating performance, reproductive organs, or sperm morphology and motility. Vortioxetine was not teratogenic in rats or rabbits, but reproductive toxicity in terms of effects on foetal weight and delayed ossification were seen in the rat at exposures more than 10-fold the human exposure at the maximum recommended therapeutic dose of 20 mg/day. Similar effects were seen in the rabbit at sub-therapeutic exposure.
In a pre- and post-natal study in rats, vortioxetine was associated with increased pup mortality, reduced bodyweight gain, and delayed pup development at doses that did not result in maternal toxicity and with associated exposures similar to those achieved in humans following administration of vortioxetine 20 mg/day (see Use in Pregnancy & Lactation).
Vortioxetine-related material was distributed to the milk of lactating rats (see Use in Pregnancy & Lactation).
In juvenile toxicity studies in rats, all vortioxetine treatment-related findings were consistent with those noted in adult animals.
Environmental risk assessment studies have shown that vortioxetine has the potential to be persistent, bioaccumulative and toxic to the environment (risk to fish). However, by recommended patient usage vortioxetine is considered to pose negligible risk to the aquatic and terrestrial environment see (Special precautions for disposal under Cautions for Usage).
Brintellix (Vortioxetine hydrobromide) is indicated for the treatment of major depressive disorder in adults.
Posology (tablet): The starting and recommended dose of Brintellix (Vortioxetine hydrobromide) is 10 mg Vortioxetine once daily.
Depending on individual patient response, the dose may be increased to a maximum of 20 mg Vortioxetine once daily or decreased to a minimum of 5 mg Vortioxetine once daily.
After the depressive symptoms resolve, treatment for at least 6 months is recommended for consolidation of the antidepressive response.
Treatment discontinuation: Patients treated with Brintellix can abruptly stop taking the medicinal product without the need for a gradual reduction in dose (see Pharmacology: Pharmacodynamics under Actions).
Special population: Elderly patients: The lowest effective dose of 5 mg vortioxetine once daily should always be used as the starting dose in patients ≥65 years of age. Caution is advised when treating patients ≥65 years of age with doses higher than 10 mg vortioxetine once daily for which data are limited (see Precautions).
Special population: Cytochrome P450 inhibitors: Depending on individual patient response, a lower dose of vortioxetine may be considered if strong CYP2D6 inhibitors (e.g. bupropion, quinidine, fluoxetine, paroxetine) are added to Brintellix treatment (see Interactions).
Special population: Cytochrome P450 inducers: Depending on individual patient response, a dose adjustment of vortioxetine may be considered if a broad cytochrome P450 inducer (e.g. rifampicin, carbamazepine, phenytoin) is added to Brintellix (Vortioxetine hydrobromide) treatment (see Interactions).
Special population: Paediatric population: The safety and efficacy of Brintellix in children and adolescents aged less than 18 years have not been established. No data are available (see Precautions).
Method of administration: Brintellix (Vortioxetine hydrobromide) is for oral use. The film-coated tablets can be taken with or without food.
Ingestion of vortioxetine in the dose range of 40 to 75 mg have caused an aggravation of the following adverse reactions: nausea, postural dizziness, diarrhoea, abdominal discomfort, generalised pruritus, somnolence and flushing.
Post-marketing experience mainly concerns vortioxetine overdoses of up to 80 mg. In the majority of cases, no symptoms or mild symptoms were reported. The most frequently reported symptoms were nausea and vomiting.
There is limited experience with vortioxetine overdoses above 80 mg. Following dosages several fold higher than the therapeutic dose range, events of seizure and serotonin syndrome have been reported.
Management of overdose should consist of treating clinical symptoms and relevant monitoring.
Medical follow-up in a specialised environment is recommended.
Hypersensitivity to the active substance or to any of the excipients listed in Description.
Concomitant use with nonselective monoamine oxidase inhibitors (MAOIs) or selective MAO-A inhibitors (see Interactions).
Suicide/suicidal thoughts or clinical worsening: Depression is associated with an increased risk of suicidal thoughts, self harm and suicide (suicide related events). This risk persists until significant remission occurs. As improvement may not occur during the first few weeks or more of treatment, patients should be closely monitored until such improvement occurs. It is general clinical experience that the risk of suicide may increase in the early stages of recovery.
Patients with a history of suicide-related events or those exhibiting a significant degree of suicidal ideation prior to commencement of treatment are known to be at greater risk of suicidal thoughts or suicide attempts, and should receive careful monitoring during treatment. A meta-analysis of placebo controlled clinical trials of antidepressants in adult patients with psychiatric disorders showed an increased risk of suicidal behaviour with antidepressants compared to placebo, in patients less than 25 years old.
Close supervision of patients and in particular those at high risk should accompany treatment especially in early treatment and following dose changes. Patients (and caregivers of patients) should be alerted to the need to monitor for any clinical worsening, suicidal behaviour or thoughts and unusual changes in behaviour and to seek medical advice immediately if these symptoms present.
Seizures: Seizures are a potential risk with antidepressants. Therefore, Brintellix (Vortioxetine hydrobromide) should be introduced cautiously in patients who have a history of seizures or in patients with unstable epilepsy (see Interactions). Treatment should be discontinued in any patient who develops seizures or for whom there is an increase in seizure frequency.
Serotonin Syndrome or Neuroleptic Malignant Syndrome (NMS): Serotonin Syndrome (SS) or Neuroleptic Malignant Syndrome (NMS), potentially life-threatening conditions, may occur with Brintellix (Vortioxetine hydrobromide). The risk of SS or NMS is increased with concomitant use of serotonergic active substances (including triptans), medicinal products that impair the metabolism of serotonin (including MAOIs), antipsychotics, and other dopamine antagonists. Patients should be monitored for the emergence of signs and symptoms of SS or NMS (see Contraindications and Interactions).
Serotonin Syndrome symptoms include mental status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g. tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperreflexia, uncoordination) and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhoea). If this occurs, treatment with Brintellix (Vortioxetine hydrobromide) should be discontinued immediately and symptomatic treatment should be initiated.
Mania/hypomania: Brintellix (Vortioxetine hydrobromide) should be used with caution in patients with a history of mania/hypomania and should be discontinued in any patient entering a manic phase.
Haemorrhage: Bleeding abnormalities, such as ecchymoses, purpura and other haemorrhagic events, such as gastrointestinal or gynaecological bleeding, has been reported rarely with the use of antidepressants with serotonergic effect (SSRIs, SNRIs). Caution is advised in patients taking anticoagulants and/or medicinal products known to affect platelet function [e.g., atypical antipsychotics and phenothiazines, most tricyclic antidepressants, non-steroidal anti-inflammatory drugs (NSAIDs), acetylsalicylic acid (ASA)] (see Interactions) and in patients with known bleeding tendencies/disorders.
Hyponatraemia: Hyponatraemia, probably due to inappropriate antidiuretic hormone secretion (SIADH), has been reported rarely with the use of antidepressants with serotonergic effect (SSRIs, SNRIs). Caution should be exercised in patients at risk, such as the elderly, patients with cirrhosis of the liver or patients concomitantly treated with medications known to cause hyponatraemia.
Discontinuation of Brintellix (Vortioxetine hydrobromide) should be considered in patients with symptomatic hyponatraemia and appropriate medical intervention should be instituted.
Renal impairment: Limited data is available for patients with severe renal impairment. Caution should therefore be exercised (see Pharmacology: Pharmacokinetics under Actions).
Hepatic impairment: Vortioxetine has not been studied in patients with severe hepatic impairment and caution should be exercised when treating these patients (see Pharmacology: Pharmacokinetics under Actions).
Effects on ability to drive and use machines: No significant impairment, relative to placebo, in driving performance, cognitive function or other psychomotor skills (using a battery of neuropsychological tests) was observed when healthy subjects were administered single and multiple doses of 10 mg/day vortioxetine.
However, as adverse reactions such as dizziness have been reported, patients should exercise caution when driving or operating hazardous machinery.
Use in Children: Brintellix (Vortioxetine hydrobromide) is not recommended for the treatment of depression in patients aged less than 18 years since the safety and efficacy of Vortioxetine have not been established in this age group (see Dosage & Administration). In clinical studies in children and adolescents treated with other antidepressants, suicide-related behaviour (suicide attempt and suicidal thoughts) and hostility (predominantly aggression, oppositional behaviour, anger) were more frequently observed than in those treated with placebo.
Pregnancy: There are limited data from the use of vortioxetine in pregnant women. Animal studies did not demonstrate a teratogenic effect of vortioxetine, but effects on foetal weight and delayed ossification were seen (see Pharmacology: Toxicology: Preclinical safety data under Actions).
The following symptoms may occur in the newborn after maternal use of a serotonergic medicinal product in later stages of pregnancy: respiratory distress, cyanosis, apnoea, seizures, temperature instability, feeding difficulty, vomiting, hypoglycaemia, hypertonia, hypotonia, hyperreflexia, tremor, jitteriness, irritability, lethargy, constant crying, somnolence and difficulty sleeping. These symptoms could be due to either discontinuation effects or excess serotonergic activity. In the majority of instances, such complications began immediately or soon (<24 hours) after delivery.
Epidemiological data suggest that the use of SSRIs in pregnancy, particularly in late pregnancy, may increase the risk of persistent pulmonary hypertension in the newborn (PPHN). Although no studies have investigated the association of PPHN with vortioxetine treatment, this potential risk cannot be ruled out taking into account the related mechanism of action (increase in serotonin concentrations).
Brintellix (Vortioxetine hydrobromide) should only be administered to pregnant women if the expected benefits outweigh the potential risk to the foetus.
Breast-feeding: Available data in animals have shown excretion of vortioxetine/vortioxetine metabolites in milk. It is expected that vortioxetine will be excreted into human milk (see Pharmacology: Toxicology: Preclinical safety data under Actions).
A risk to the breastfeeding child cannot be excluded.
A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from Brintellix (Vortioxetine hydrobromide) treatment taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman.
Fertility: Fertility studies in male and female rats showed no effect of vortioxetine on fertility, sperm quality or mating performance (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Human case reports with medicinal products from the related pharmacological class of antidepressants (SSRIs) have shown an effect on sperm quality that is reversible. Impact on human fertility has not been observed so far.
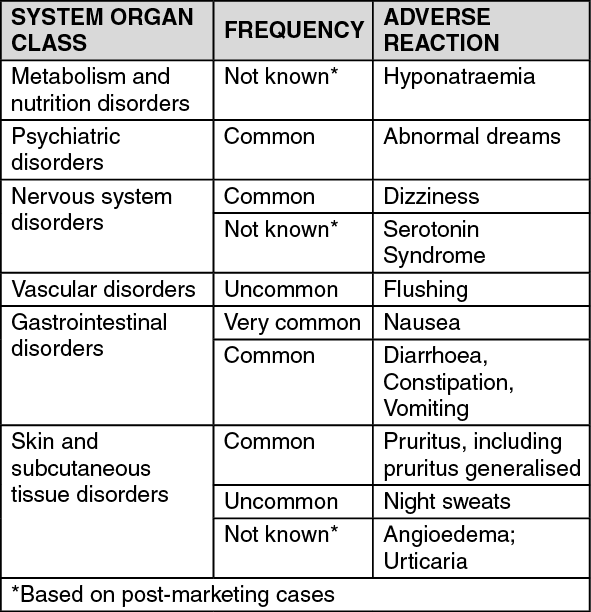
Summary of the safety profile: The most common adverse reaction was nausea.
Tabulated list of adverse reactions: Adverse reactions are listed as follows using the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data). The list is based on information from clinical trials and post-marketing experience. (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions: Nausea:
Click on icon to see table/diagram/image
Description of selected adverse reactions: Nausea: Nausea was usually mild or moderate and occurred within the first two weeks of treatment. The reactions were usually transient and did not generally lead to cessation of therapy. Gastrointestinal adverse reactions, such as nausea, occurred more frequently in women than men.
Sexual dysfunction: In clinical studies, sexual dysfunction was assessed using the Arizona Sexual Experience Scale (ASEX). Doses of 5 to 15 mg showed no difference to placebo. However, the 20 mg dose of vortioxetine was associated with an increase in treatment-emergent sexual dysfunction (TESD) (see Pharmacology: Pharmacodynamics under Actions).
Class effect: Epidemiological studies, mainly conducted in patients 50 years of age and older, show an increased risk of bone fractures in patients receiving a drug from related pharmacological classes of antidepressants (SSRIs or TCAs). The mechanism behind this risk is unknown, and it is not known if this risk is also relevant for vortioxetine.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
Vortioxetine is extensively metabolised in the liver primarily through oxidation and subsequent glucuronic acid conjugation. In vitro, the cytochrome P450 isozymes CYP2D6, CYP3A4/5, CYP2C19, CYP2C9, CYP2A6, CYP2C8 and CYP2B6 are involved in the metabolism of vortioxetine (see Pharmacology: Pharmacokinetics under Actions).
Potential for other medicinal products to affect vortioxetine: Irreversible non-selective MAOIs: Due to the risk of Serotonin Syndrome, vortioxetine is contraindicated in any combination with irreversible non-selective MAOIs. Vortioxetine must not be initiated for at least 14 days after discontinuation of treatment with an irreversible non-selective MAOI. Vortioxetine must be discontinued for at least 14 days before starting treatment with an irreversible non-selective MAOI (see Contraindications).
Reversible, selective MAO-A inhibitor (moclobemide): The combination of vortioxetine with a reversible and selective MAO-A inhibitor, such as moclobemide, is contraindicated (see Contraindications). If the combination proves necessary, the added medicinal product should be given with minimum dosage and under close clinical monitoring for Serotonin Syndrome (see Precautions).
Reversible, non-selective MAOI (linezolid): The combination of vortioxetine with a weak reversible and non-selective MAOI, such as the antibiotic linezolid, is contraindicated (see Contraindications). If the combination proves necessary, the added medicinal product should be given with minimum dosage and under close clinical monitoring for Serotonin Syndrome (see Precautions).
Irreversible, selective MAO-B inhibitor (selegiline, rasagiline): Although a lower risk of Serotonin Syndrome is expected with selective MAO-B inhibitors than with MAO-A inhibitors, the combination of vortioxetine with irreversible MAO-B inhibitors, such as selegiline or rasagiline should be exercised with caution. Close monitoring for Serotonin Syndrome is necessary if used concomitantly (see Precautions).
Serotonergic medicinal products: Co-administration of medicinal products with serotonergic effect (e.g., tramadol, sumatriptan and other triptans) may lead to Serotonin Syndrome (see Precautions).
St. John's wort: Concomitant use of antidepressants with serotonergic effect and herbal remedies containing St. John's wort (Hypericum perforatum) may result in a higher incidence of adverse reactions including Serotonin Syndrome (see Precautions).
Medicinal products lowering the seizure threshold: Antidepressants with serotonergic effect can lower the seizure threshold. Caution is advised when concomitantly using other medicinal products capable of lowering the seizure threshold [(e.g. antidepressants (tricyclics, SSRIs, SNRIs), neuroleptics (phenothiazines, thioxanthenes and butyrophenones), mefloquin, bupropion, tramadol)] (see Precautions).
ECT (electroconvulsive therapy): There is no clinical experience with concurrent administration of vortioxetine and ECT, therefore caution is advisable.
CYP2D6 inhibitors: The exposure to vortioxetine increased 2.3-fold for area under the curve (AUC) when vortioxetine 10 mg/day was co administered with bupropion (a strong CYP2D6 inhibitor 150 mg twice daily) for 14 days in healthy subjects. Co-administration resulted in a higher incidence of adverse reactions when bupropion was added to vortioxetine than when vortioxetine was added to bupropion. Depending on individual patient response, a lower dose of vortioxetine may be considered if strong CYP2D6 inhibitor (e.g., bupropion, quinidine, fluoxetine, paroxetine) is added to vortioxetine treatment (see Dosage & Administration).
CYP3A4 inhibitors and CYP2C9, and CYP2C19 inhibitors: When vortioxetine was co-administered following 6 days of ketoconazole 400 mg/day (a CYP3A4/5 and P-glycoprotein inhibitor) or following 6 days of fluconazole 200 mg/day (a CYP2C9, CYP2C19, and CYP3A4/5 inhibitor) in healthy subjects, a 1.3-fold and 1.5-fold increase, respectively, in vortioxetine AUC was observed. No dose adjustment is needed.
No inhibitory effect of 40 mg single-dose omeprazole (CYP2C19 inhibitor) was observed on the multiple-dose pharmacokinetics of vortioxetine in healthy subjects.
Cytochrome P450 inhibitors: The exposure to vortioxetine increased 2.3-fold for Areal Under Curve (AUC) when vortioxetine 10 mg/day was co administered with bupropion (a strong CYP2D6 inhibitor 150 mg twice daily) for 14 days in healthy subjects. Co-administration resulted in a higher incidence of adverse reactions when bupropion was added to vortioxetine than when vortioxetine was added to bupropion. Depending on individual patient response, a lower dose of vortioxetine may be considered if strong CYP2D6 inhibitors (e.g. bupropion, quinidine, fluoxetine, paroxetine) are added to vortioxetine treatment (see Dosage & Administration).
When vortioxetine was co-administered following 6 days of ketoconazole 400 mg/day (a CYP3A4/5 and P-glycoprotein inhibitor) or following 6 days of fluconazole 200 mg/day (a CYP2C9, CYP2C19, and CYP3A4/5 inhibitor) in healthy subjects, a 1.3-fold and 1.5-fold increase, respectively in vortioxetine AUC was observed. No dose adjustment is needed.
Interactions in CYP2D6 poor metabolisers: Co-administration of strong inhibitors of CYP3A4 (such as itraconazole, voriconazole, clarithromycin, telithromycin, nefazodone, conivaptan and many of the HIV protease inhibitors) and inhibitors of CYP2C9 (such as fluconazole and amiodarone) to CYP2D6 poor metabolisers (see Pharmacology: Pharmacokinetics under Actions) has not been investigated specifically, but it is anticipated that it will lead to a more marked increased exposure of vortioxetine in these patients as compared to the moderate effect described previously. Depending on individual patient response, a lower dose of vortioxetine may be considered if a strong inhibitor of CYP3A4 or CYP2C9 is co-administered in CYP2D6 poor metabolisers.
Co-administration of strong inhibitors of CYP3A4 and CYP2C9 to CYP2D6 poor metabolisers has not been investigated specifically, but it is anticipated that it will lead to increased exposure of vortioxetine in these patients (see Pharmacology: Pharmacokinetics under Actions).
Cytochrome P450 inducers: When a single dose of 20 mg vortioxetine was co-administered following 10 days of rifampicin 600 mg/day (a broad inducer of CYP isozymes) in healthy subjects, a 72% decrease in AUC of vortioxetine was observed. Depending on individual patient response, a dose adjustment may be considered if a broad cytochrome P450 inducer (e.g. rifampicin, carbamazepine, phenytoin) is added to vortioxetine treatment (see Dosage & Administration).
Alcohol: No effect on the pharmacokinetics of vortioxetine or ethanol and no significant impairment, relative to placebo, in cognitive function was observed when vortioxetine single doses of 20 mg or 40 mg was co-administered with a of single dose of ethanol (0.6 g/kg) in healthy subjects.
Acetylsalicylic acid: No effect of multiple doses of acetylsalicylic acid 150 mg/day on the multiple-dose pharmacokinetics of vortioxetine was observed in healthy subjects.
Potential for vortioxetine to affect other medicinal products: Anticoagulants and antiplatelet medicinal products: No significant effects, relative to placebo, were observed in INR, prothrombin or plasma R/S warfarin values following co-administration of multiple doses of vortioxetine with stable doses of warfarin in healthy subjects. Also, no significant inhibitory effect, relative to placebo, on platelet aggregation or pharmacokinetics of acetylsalicylic acid or salicylic acid was observed when acetylsalicylic acid 150 mg/day was co-administered following multiple doses of vortioxetine administration in healthy subjects. However, as for other serotonergic medicinal products, caution should be exercised when vortioxetine is combined with oral anticoagulants or antiplatelet medicinal products due to a potential increased risk of bleeding attributable to a pharmacodynamic interaction (see Precautions).
Potential pharmacokinetic interactions: Cytochrome P450 substrates: In vitro, vortioxetine did not show any relevant potential for inhibition or induction of cytochrome P450 isozymes (see Pharmacology: Pharmacokinetics under Actions).
Following multiple doses of vortioxetine, no inhibitory effect was observed in healthy subjects for the cytochrome P450 isozymes CYP2C19 (omeprazole, diazepam), CYP3A4/5 (ethinyl estradiol, midazolam), CYP2B6 (bupropion), CYP2C9 (tolbutamide, S-warfarin), CYP1A2 (caffeine) or CYP2D6 (dextromethorphan).
No pharmacodynamic interactions were observed. No significant impairment, relative to placebo, in cognitive function was observed for vortioxetine following co-administration with single 10 mg dose of diazepam. No significant effects, relative to placebo, were observed in the levels of sex hormones following co administration of vortioxetine with a combined oral contraceptive (ethinyl estradiol 30 μg/levonorgestrel 150 μg).
Lithium, tryptophan: No clinically relevant effect was observed during steady-state lithium exposure following co-administration with multiple doses of vortioxetine in healthy subjects. However, there have been reports of enhanced effects when antidepressants with serotonergic effect have been given together with lithium or tryptophan, therefore concomitant use of vortioxetine with these medicinal products should be undertaken with caution.
Incompatibilities: Not applicable.
Special precautions for disposal: Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Store at temperatures not exceeding 30°C.
Shelf-Life: 48 months.
N06AX26 - vortioxetine ; Belongs to the class of other antidepressants.
Brintellix FC tab 10 mg
28's (P1,726.79/box)
Brintellix FC tab 15 mg
28's (P2,936.37/box)
Brintellix FC tab 5 mg
28's (P924.11/box)



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out