Pharmacology: Pharmacokinetics: Plasma concentrations: At the end of a 30- minute intravenous infusion of a single dose of Meropenem Powder for Injection (IV) (Intravenous) in healthy volunteers, mean peak plasma concentrations of Meropenem are approximately 23 mcg/mL (range 14 to 26) for the 500 mg dose and 49 mcg/mL (range 39 to 58) for the 1 gram dose.
A 5-minute intravenous bolus injection of Meropenem Powder for injection I.V. in healthy volunteers results in mean peak plasma concentrations of approximately 45 mcg/mL (Range 18 to 65) for the 500 mg dose and 112 mcg/mL (range 83 to 140) for the 1 gram dose.
Following intravenous doses of 500 mg, mean plasma concentrations of Meropenem usually decline to approximately 1 mcg/mL at 6 hours after administration.
No accumulation of Meropenem in plasma was observed with regimens using 500 mg administered every 8 hours or 1 gram administered every 6 hours in healthy volunteers with normal renal function.
Distribution: The plasma protein binding of Meropenem is approximately 2%.
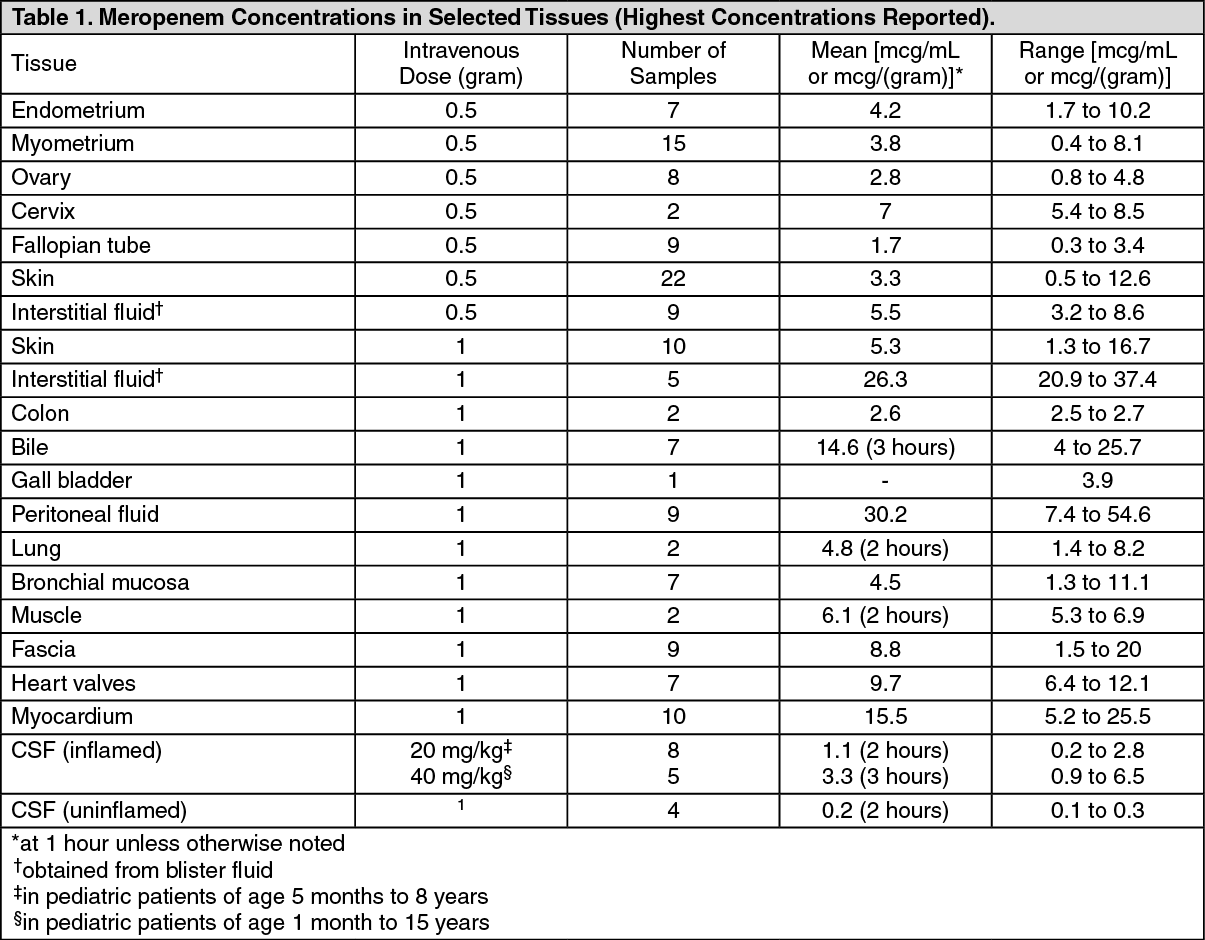
Meropenem penetrates well into most body fluids and tissues including cerebrospinal fluid, achieving concentrations matching or exceeding those required to inhibit most susceptible bacteria. After a single intravenous dose of Meropenem Powder for injection (IV), the highest mean concentrations of Meropenem were found in tissues and fluids at 1 hour (0.5 to 1.5 hours) after the start of infusion, except where Indicated in the tissues and fluids listed in the table as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Metabolism:
Click on icon to see table/diagram/image
Metabolism: There is one metabolite of Meropenem that ls microbiologically inactive.
Excretion: In subjects with normal renal function, the elimination half-life of Meropenem is approximately 1 hour. Meropenem is primarily excreted unchanged by the kidneys. Approximately 70% (50% to 75%) of the dose is excreted unchanged within 12 hours. A further 28% is recovered as the microbiologically Inactive metabolite. Fecal elimination represents only approximately 2% of the dose. The measured renal clearance and the effect of probenecid show that Meropenem undergoes both filtration and tubular secretion. Urinary concentrations of Meropenem in excess of 10 mcg/mL are maintained for up to 5 hours after a 500 mg dose.
Microbiology: Mechanism of Action: The bactericidal activity of Meropenem results from the inhibition of cell wall synthesis. Meropenem readily penetrates the cell wall of most Gram-positive and Gram-negative bacteria to reach penicillin-binding-protein (PBP) targets. Its strongest affinities are toward PBPs 2, 3 and 4 of
Escherichia coli and
Pseudomonas aeruginosa; and PBPs 1, 2 and 4 of
Staphylococcus aureus. Bactericidal concentrations (defined as a 3 log 10 reduction in cell counts within 12 hours to 24 hours) are typically 1 to 2 times the bacteriostatic concentrations of Meropenem, with the exception of
Listeria monocytogenes, against which lethal activity is not observed.
Meropenem has significant stability to hydrolysis by β-lactamases, both penicillinases and cephalosporinases produced by Gram-positive and Gram-negative bacteria.
Meropenem should not be used to treat methicillin-resistant
Staphylococcus aureus (MRSA) or methicillin-resistant
Staphylococcus epidermidis (MRSE).
Mechanism of Resistance: There are several mechanisms of resistance to carbapenems: 1. decreased permeability of the outer membrane of Gram-negative bacteria (due to diminished production of porins) causing reduced bacterial uptake; 2. reduced affinity of the target PBPs; 3. increased expression of efflux pump components, and; 4. production of antibacterial drug-destroying enzymes (carbapenemases, metallo-β-lactamases). Localized clusters of infections due to carbapenem-resistant bacteria have been reported in some regions.
Cross-Resistance: Cross-resistance is sometimes observed with isolates resistant to other carbapenems. Interactions with Other Antibacterial Drugs. In vitro tests show Meropenem to act synergistically with aminoglycoside antibacterials against some isolates of
Pseudomonas aeruginosa.
Spectrum of Activity: Meropenem has been shown to be active against most isolates of the following bacteria, both in vitro and in clinical Infections as described (see Indications).
Gram-positive bacteria:
Enterococcus faecalis (vancomycin-susceptible isolates only)
Staphylococcus aureus (methicillin-susceptible isolates only)
Streptococcus agalactiae
Streptococcus pneumoniae (penicillin-susceptible isolates only)
Streptococcus pyogenes
Viridans group streptococci
Gram-negative bacteria:
Escherichia coli; Neisseria meningitidis; Anaerobic bacteria; Peptostreptococcus species;
Haemophtlus influenzae; Pseudomonas aeruginosa; Bacteroides fragilis; Klebsiella pneumoniae; Proteus mirabilis; Bacteroides thetaiotaomicron.
The following in vitro data are available, but their clinical significance is unknown. At least 90% of the following bacteria have exhibited in vitro minimum inhibitory concentrations (MICs) less than or equal to the susceptible breakpoints for Meropenem. However, the safety and effectiveness of Meropenem in treating clinical infections due to these bacteria have not been established in adequate and well-controlled trials.
Gram-positive bacteria:
Staphylococcus epidermidis (methicillin-susceptible isolates only).
Gram-negative bacteria:
Aeromonas hydrophila; Citrobacter freundii;
Klebsiella oxytoca;
Pasteurella multocida;
Anaerobic bacteria; Bacteroides uniformis;
Campylobaeter jejuni;
Enterobacter cloacae;
Moraxella catarrhalis;
Proteus vulgaris;
Bacteroides distasonis;
Bacteroides ureolyticus;
Citrobacter koseri (formerly
diversus);
Hafnia alvei;
Morganella morganii;
Serratia marcescens;
Bacteroides ovatus;
Baeteroides vulgatus.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out