


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: Mechanism of Action: Persistent infection with oncogenic HPV types has been demonstrated to be responsible for virtually all cases of cervical cancer worldwide.
Cervarix is a non-infectious recombinant vaccine prepared from the highly purified virus-like particles (VLPs) of the major capsid L1 protein of oncogenic HPV types 16 and 18. Since the VLPs contain no viral DNA, they cannot infect cells, reproduce or cause disease. Animal studies have shown that the efficacy of L1 VLP vaccines is largely mediated by the development of a humoral immune response and cell-mediated immune memory.
Cervarix is adjuvanted with AS04 which has been shown in clinical trials to induce a higher and long-lasting immune response compared to the same antigens adjuvanted with aluminium salt [Al(OH)3] alone.
Invasive cervical cancer includes squamous cervical carcinoma (84%) and adenocarcinoma (16%, up to 20% in developed countries with screening programs).
HPV-16 and HPV-18 are responsible for approximately 70% of cervical cancers, 80% of vulvar and vaginal cancers, 90% of anal cancers, 70% of HPV related high-grade vulvar (VIN 2/3) and vaginal intraepithelial neoplasia (VaIN 2/3) and 78% of HPV related high-grade anal (AIN 2/3) intraepithelial neoplasia across all regions worldwide.
Other oncogenic HPV types (HPV-31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, -68) can also cause ano-genital cancers. HPV-16, -18, -45 and -31 are the 4 most common types identified in squamous cervical carcinoma (approximately 76%) and adenocarcinoma (approximately 91%).
Evidence of Anamnestic (Immune Memory) Response: The administration of a challenge dose after a mean of 6.8 years following the first vaccination elicited an anamnestic immune response to HPV-16 and HPV-18 (by ELISA and pseudovirion-based neutralizing assay) at day 7. One month after the challenge dose, GMTs exceeded those observed one month after the primary vaccination course.
An anamnestic response was also observed for the related types HPV-31 and HPV-45 by ELISA.
Prophylactic Efficacy: Clinical efficacy in women aged 15 to 25 years: The efficacy of Cervarix was assessed in 2 controlled, double-blind, randomised clinical studies (HPV-001/007 and HPV-008) that included a total of 19,778 women aged 15 to 25 years at enrollment.
Clinical trial HPV-001/007 was conducted in North America and Latin America. Study HPV-023 followed-up subjects from the Brazilian cohort of study 001/007. Study entry criteria were: negative for oncogenic HPV DNA (HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) in cervical samples, seronegative for HPV-16 and HPV-18 antibodies and normal cytology. These characteristics are representative of a population presumed naïve to oncogenic HPV types prior to vaccination.
Clinical trial HPV-008 was conducted in North America, Latin America, Europe, Asia Pacific and Australia. Pre-vaccination samples were collected for oncogenic HPV DNA (HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) testing and serum testing for HPV-16 and HPV-18 antibodies. Women were vaccinated regardless of baseline cytology and HPV serological and DNA status. These characteristics are representative of a population which includes women with evidence of past and/or current HPV infection.
As in any prophylactic efficacy trial, subjects initially infected with a particular HPV type were not eligible for the efficacy assessment of that type.
Cervical intraepithelial neoplasia (CIN) grade 2 and 3 (CIN2+) was used in the clinical trials as a surrogate marker for cervical cancer. Persistent infection that lasts for at least 6 months has also been shown to be a relevant surrogate marker for cervical cancer. Although CIN grade 1 is not a surrogate marker for cervical cancer, these lesions require medical follow-up.
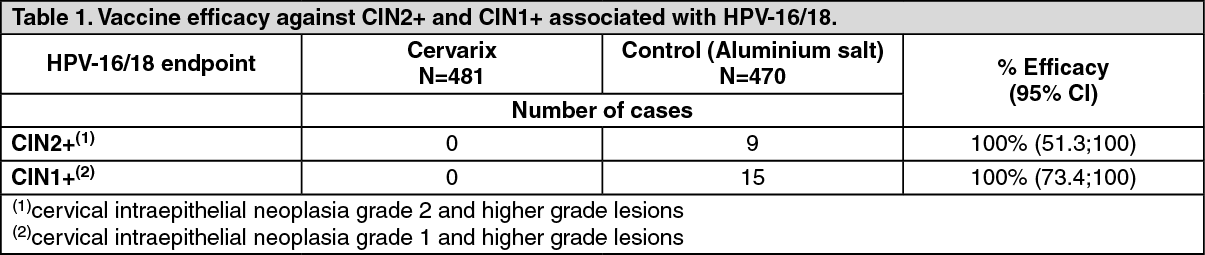
Vaccine efficacy against HPV-16/18 in women naїve to oncogenic HPV types (studies HPV-001/007/023): Efficacy results for histological endpoints associated with HPV-16 and/or HPV-18 (HPV-16/18) observed in study HPV-001/007 (Total Cohort i.e. women who received at least one vaccine dose) are presented in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEfficacy against HPV-16/18 cytological abnormalities was 96.7% (95% CI: 87.3;99.6).
Efficacy against HPV-16/18 persistent infection was 98.2% (95% CI: 89.5;100) and 96.9% (95% CI: 81.4;99.9) when using a 6-month and a 12-month definition, respectively.
In study HPV-023, subjects (N=437) were followed-up to 9.4 years (approximately 113 months) after dose one. There were no new cases of infection or histopathological lesions associated with HPV-16/18 in the vaccine group. In the placebo group, there were 4 cases of 6-month persistent infection, 1 case of 12-month persistent infection and 1 case of CIN1+ associated with HPV-16/18.
In the descriptive combined analysis of studies HPV-001/007/023, efficacy against HPV-16/18 incident and 6-month persistent infection was 91.0% (95% CI: 80.2;96.5) and 96.8% (95% CI: 80.4;99.9), respectively. Despite evidence of continuous exposure to HPV infections as observed in the control group, there is no evidence of waning protection in vaccinated women.
Vaccine efficacy in women with evidence of past and/or current HPV infection (study HPV-008): Prophylactic efficacy against HPV-16/18 in women naїve to HPV-16 and/or HPV-18: In study HPV-008, the primary analyses of efficacy were performed on the According to Protocol cohort (ATP cohort: including women who received 3 vaccine doses and were naїve to the relevant HPV type at month 0 and month 6) and the Total Vaccinated Cohort-1 (TVC-1 cohort: including women who received at least one vaccine dose and were naїve to the relevant HPV type at month 0). Both cohorts included women with normal or low-grade cytology at baseline and excluded only women with high-grade cytology (0.5%).
In addition, analyses of efficacy were performed on the broader Total Vaccinated Cohort (TVC) and TVC-naїve.
In study HPV-008, approximately 26% of women had evidence of current and/or prior HPV-16/18 infection and less than 1% of women were HPV DNA positive for both HPV-16 and HPV-18 types at baseline.
The final analysis of study HPV-008 was event-triggered, i.e. was performed when at least 36 CIN2+ cases associated with HPV-16/18 were accrued in the ATP cohort.
The mean follow-up was approximately 39 months post dose one.
End of study analysis was performed at the end of the 4-year follow-up period (i.e. 48 months post dose one) and included all subjects from the Total Vaccinated Cohort (TVC).
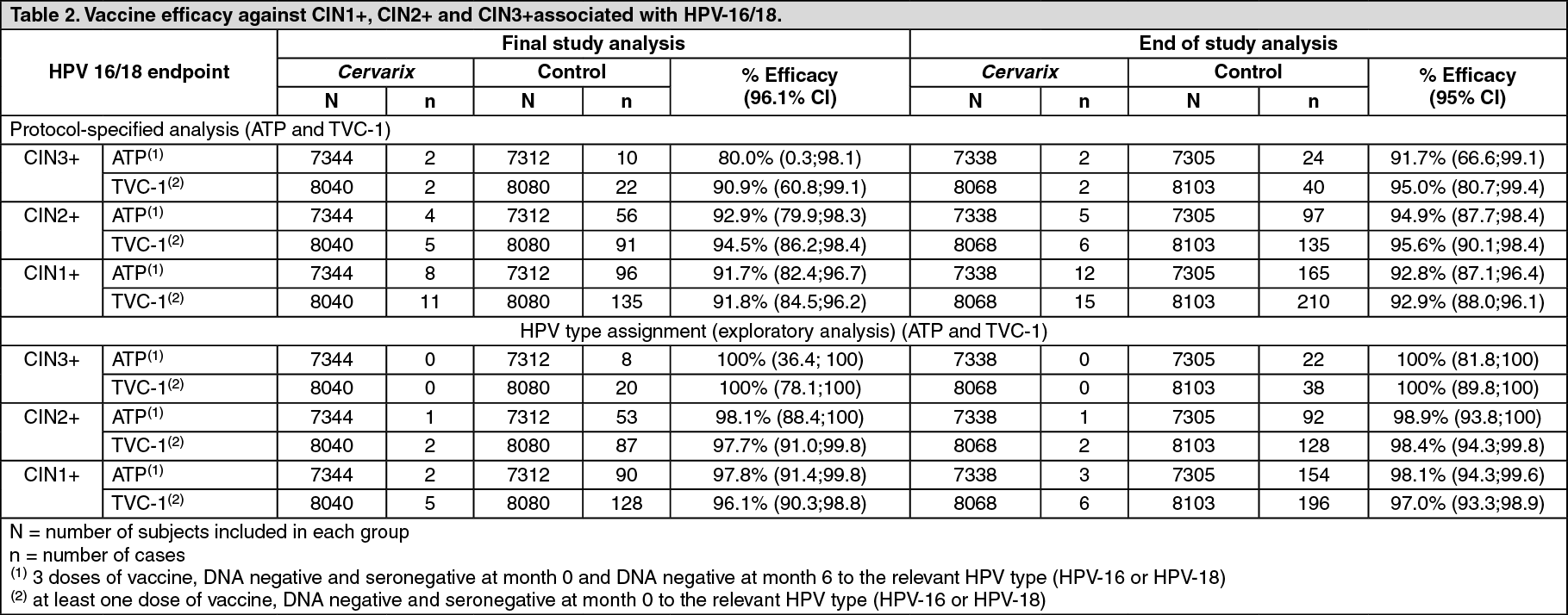
In the protocol-specified analysis, vaccine efficacy against CIN1+ and CIN2+ associated with HPV-16/18 was statistically significant in the ATP and TVC-1 cohorts.
Further investigation identified that several CIN3+, CIN1+ and CIN2+ cases had multiple oncogenic HPV types in the lesion. In order to distinguish between the HPV type(s) most likely to be responsible for a lesion, from the HPV type(s) only temporarily associated, an HPV type assignment was applied (exploratory analysis). The HPV type assignment considered the HPV types detected by Polymerase Chain Reaction (PCR) in at least one of the two preceding cytologic samples, in addition to types detected in the lesion. Based on this HPV type assignment, the analysis excluded cases (in the vaccine group and in the control group) which were not considered to be causally associated with HPV-16 or HPV-18 infections acquired during the trial.
The results observed in both analysis (i.e. protocol-specified analysis and HPV type assignment) are presented in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn addition, at the time of final study analysis, statistically significant vaccine efficacy against CIN2+ associated with HPV-16 and HPV-18 individually was demonstrated in both cohorts for each analysis.
Vaccine efficacy against 6-month and 12-month persistent infection and cytological abnormalities (≥ASCUS) associated with HPV-16/18 was also assessed. The observed vaccine efficacy against each endpoint was statistically significant in both cohorts: At the time of final study analysis: 6-month persistent infection: 94.3% (91.5;96.3) in ATP cohort and 90.2% (87.3;92.6) in TVC-1 cohort; 12-month persistent infection: 91.4% (86.1;95.0) in ATP cohort and 85.3% (79.9;89.4) in TVC-1 cohort; cytological abnormalities (≥ASCUS): 89.0% (84.9;92.1) in ATP cohort and 86.7% (82.8;89.8) in TVC-1 cohort.
At the end of study analysis: 6-month persistent infection: 94.3% (92.0;96.1) in ATP cohort and 91.0% (88.5;93.0) in TVC-1 cohort; 12-month persistent infection: 92.9% (89.4;95.4) in ATP cohort and 88.2% (84.5%;91.2%) in TVC-1 cohort; cytological abnormalities (≥ASCUS): 90.7% (87.8;93.1) in ATP cohort and 88.6% (85.6;91.0) in TVC-1 cohort.
At the time of the final study analysis, statistically significant vaccine efficacy against VIN1+ (vulvar intraepithelial neoplasia grade 1 and higher grade lesions) or VaIN1+ (vaginal intraepithelial neoplasia grade 1 and higher grade lesions) associated with HPV-16/18 was also observed in both cohorts: 80.0% (96.1% CI: 0.3;98.1) in ATP cohort and 83.2% (96.1% CI: 20.2;98.4) in TVC-1 cohort. At the end of study analysis, vaccine efficacy against VIN1+ or VaIN1+ associated with HPV-16/18 was 75.1% (95% CI: 22.9;94.0) in ATP cohort and 77.7% (95% CI: 32.4;94.5) in TVC-1 cohort. There were 2 cases of VIN2+ or VaIN2+ associated with HPV-16 or HPV-18 in the vaccine group and 7 cases in the control group in the ATP cohort. The study was not powered to demonstrate a difference between the vaccine and the control group for these endpoints.
There was no evidence of protection from disease caused by the HPV types for which subjects were HPV DNA positive at study entry. However, individuals already infected with one of the vaccine-related HPV types prior to vaccination were protected from clinical disease caused by the other vaccine HPV type.
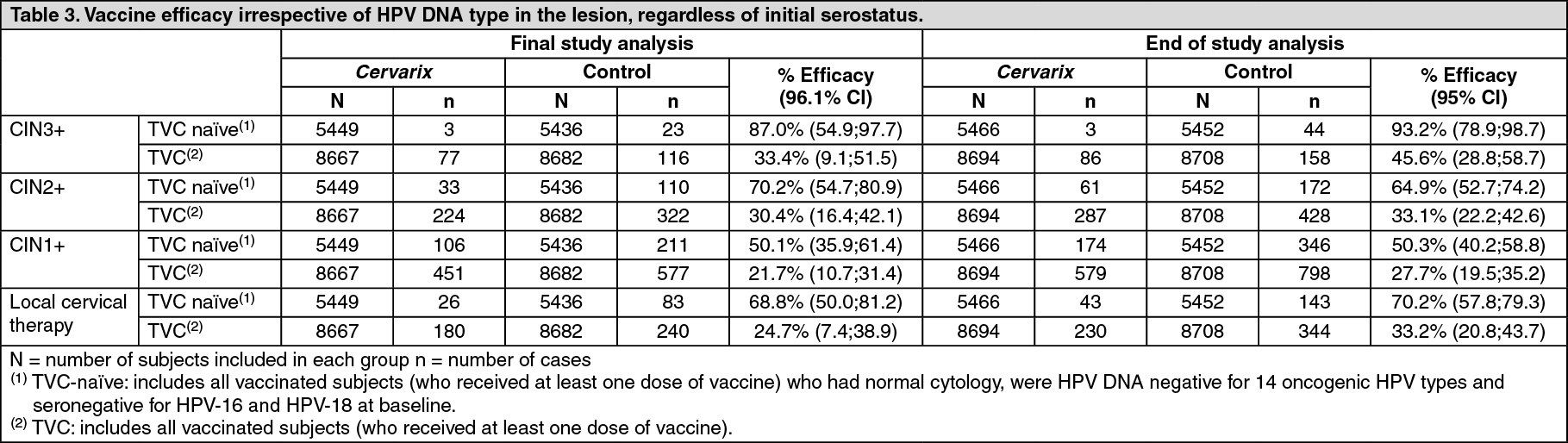
Overall impact of the vaccine on HPV disease burden: The overall vaccine efficacy irrespective of HPV DNA type in the lesion and stratified by baseline HPV DNA and serostatus was evaluated in study HPV-008.
In the TVC and TVC-naїve cohorts which included all vaccinated women, vaccine efficacy against CIN3+, CIN2+ and CIN1+ was demonstrated (Table 3). The impact of Cervarix on reduction of local cervical therapy (Loop Electro-Excision Procedure, Cone, Knife or Laser) was also demonstrated in the same cohorts (Table 3).
The TVC-naїve is a subset of the TVC that includes women with normal cytology, and who were HPV DNA negative for 14 oncogenic HPV types (HPV-16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, -68) and seronegative for HPV-16 and HPV-18 at baseline. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageProphylactic efficacy against infection by oncogenic HPV types other than HPV-16 and HPV-18: In study HPV-008, vaccine efficacy against 12 non-vaccine oncogenic HPV types (HPV-31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, -68) was evaluated in ATP and TVC-1 cohorts.
At the time of the final study analysis, statistically significant vaccine efficacy against CIN2+ for all HPV types combined (HPV-31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, -68) excluding HPV types 16 and 18 was demonstrated with 54.0% (96.1% CI: 34.0;68.4) in ATP cohort and 46.0% (96.1% CI: 27.0;60.3) in TVC-1 cohort. At the end of study analysis, vaccine efficacy against CIN2+ for all HPV types combined excluding HPV types 16 and 18 was 46.8% (95% CI: 30.7;59.4) in the ATP cohort and 40.8% (95% CI: 25.5;53.1) in the TVC-1 cohort.
At the time of the final study analysis, statistically significant vaccine efficacy against 6-month persistent infection and against CIN2+ has been observed for the following individual HPV types: 6-month persistent infection: types 31, 33, 45 in ATP cohort; types 31, 33, 45, 51 in TVC-1 cohort.
CIN2+: types 31, 51, 58 in ATP cohort; types 31, 33, 35, 51 in TVC-1 cohort.
At the end of study analysis, more cases were accrued and a lower limit of the 95% CI above zero has been observed for HPV types 31, 33, 45 and 51 for both 6-month persistent infection and CIN2+ in the ATP and TVC-1 cohorts. For CIN2+, a lower limit of the 95% CI above zero has also been observed for HPV type 39 in the ATP cohort and HPV type 66 in the TVC-1 cohort.
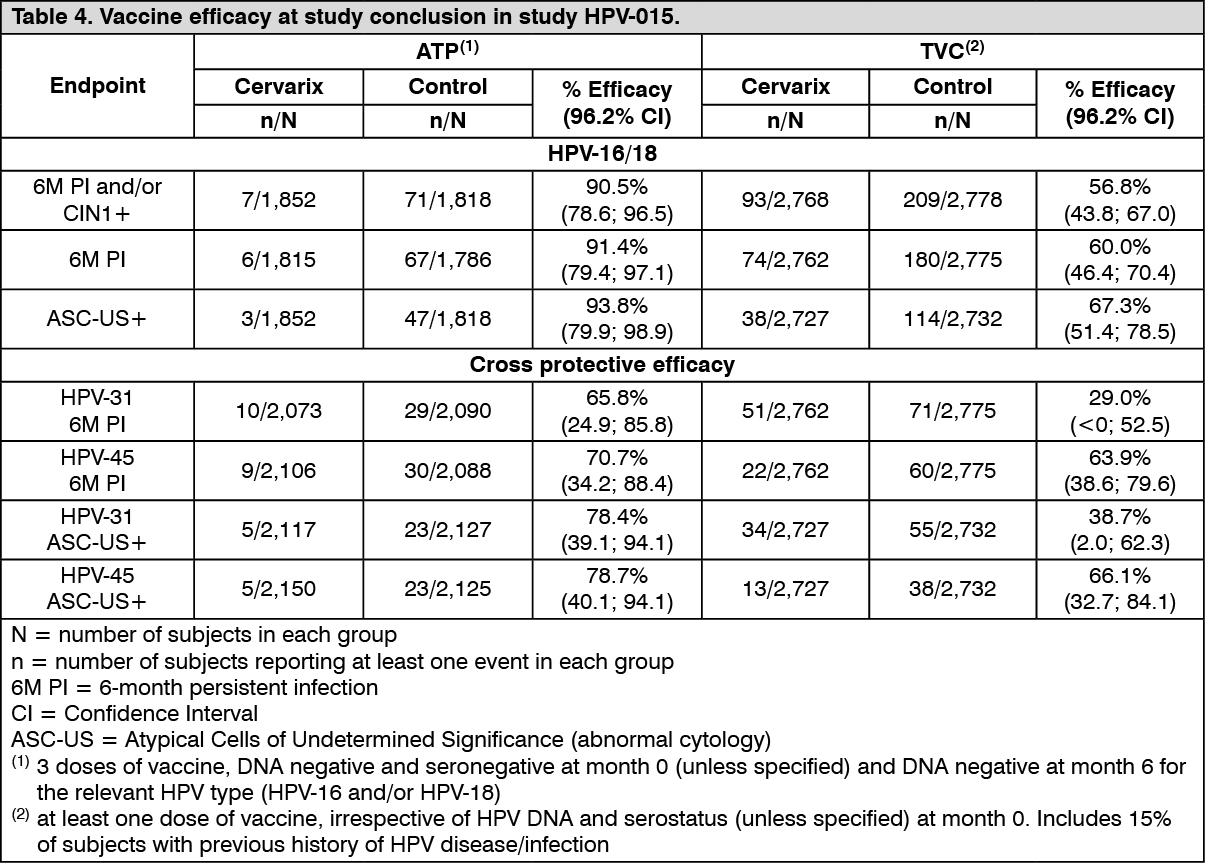
Clinical efficacy in women aged 26 years and older: The efficacy of Cervarix was assessed in a double-blind, randomised Phase III clinical trial (HPV-015) that included a total of 5,778 women aged 26-72 years (Median: 37.0 years). The study was conducted in North America, Latin America, Asia Pacific and Europe. Final analysis was performed at study conclusion 7 years after the first Cervarix dose.
The primary endpoint was a combination of a virological and histopathological endpoint: HPV 16/18 related 6-month persistent infection and/or CIN1+. The primary analyses of efficacy were performed on the ATP cohort for efficacy and the TVC which included a subset of up to 15% of women with a history of HPV-associated infection or disease.
Vaccine efficacy at study conclusion is summarised in the following table. (See Table 4.)
 Click on icon to see table/diagram/image
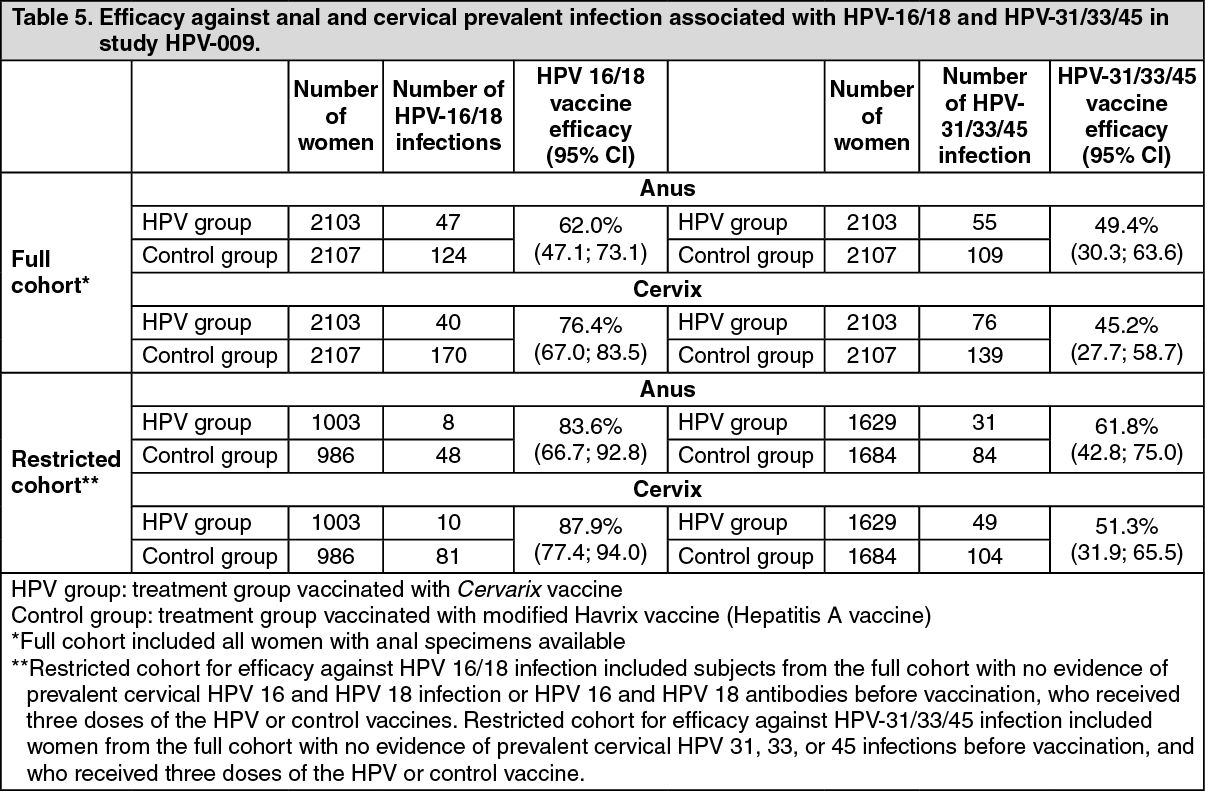
Click on icon to see table/diagram/imageClinical efficacy against anal prevalent infection in women aged 18-25 years: Study HPV-009 evaluated vaccine efficacy against anal prevalent infection at the 4-year study visit. Vaccine efficacy against HPV-16/18 and against non-vaccine types HPV-31/33/45 is presented in Table 5. Cervical infection in the same women at the same visit was assessed for comparison purpose. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageVaccine-Induced Immunogenicity: The antibody response to HPV-16 and HPV-18 was measured using a type specific ELISA which was shown to strongly correlate with neutralisation assays (including pseudovirion-based neutralizing assay developed by the US National Cancer Institute). Transudation of antibodies from serum to the cervical mucosa has been demonstrated in clinical trials.
The immunogenicity induced by three doses of Cervarix has been evaluated in over 5,000 female subjects from 9 to 55 years of age and over 800 male subjects aged 10 to 18 years.
In clinical trials, more than 99% of initially seronegative subjects had seroconverted to both HPV type 16 and 18 one month after the third dose. Vaccine-induced IgG Geometric Mean Titres (GMT) were well above titres observed in women previously infected but who cleared HPV infection (natural infection). Initially seropositive and seronegative subjects reached similar titres after vaccination.
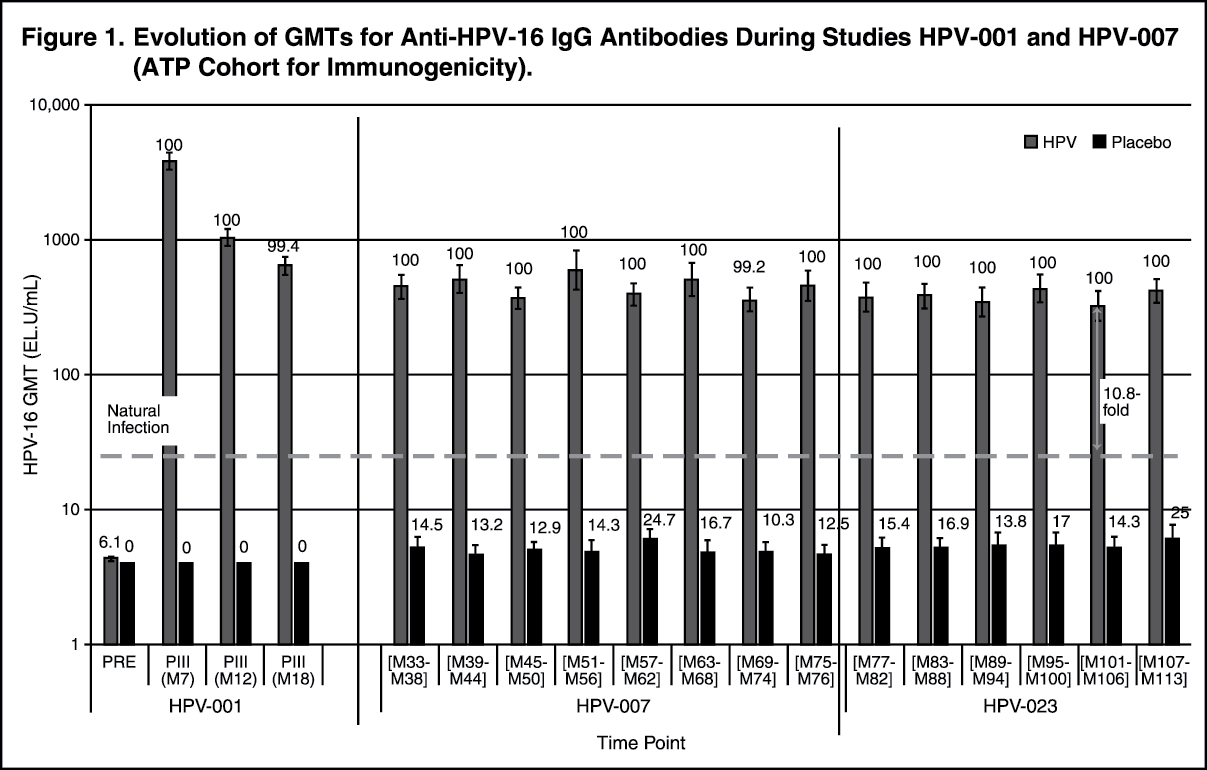
Immunogenicity in women aged 15 to 25 years: In study HPV-001/007, the immune response against HPV-16 and HPV-18 was evaluated up to 76 months post dose one in women 15 to 25 years old at the time of vaccination. In study HPV-023, this immune response continued to be evaluated up to 9.4 years post dose one in a subset of the population from study HPV-001/007.
In study HPV-023, 100% of women were seropositive for both HPV-16 and HPV-18 by ELISA or by pseudovirion-based neutralizing assay (PBNA) up to 9.4 years after first vaccination. (See Figures 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image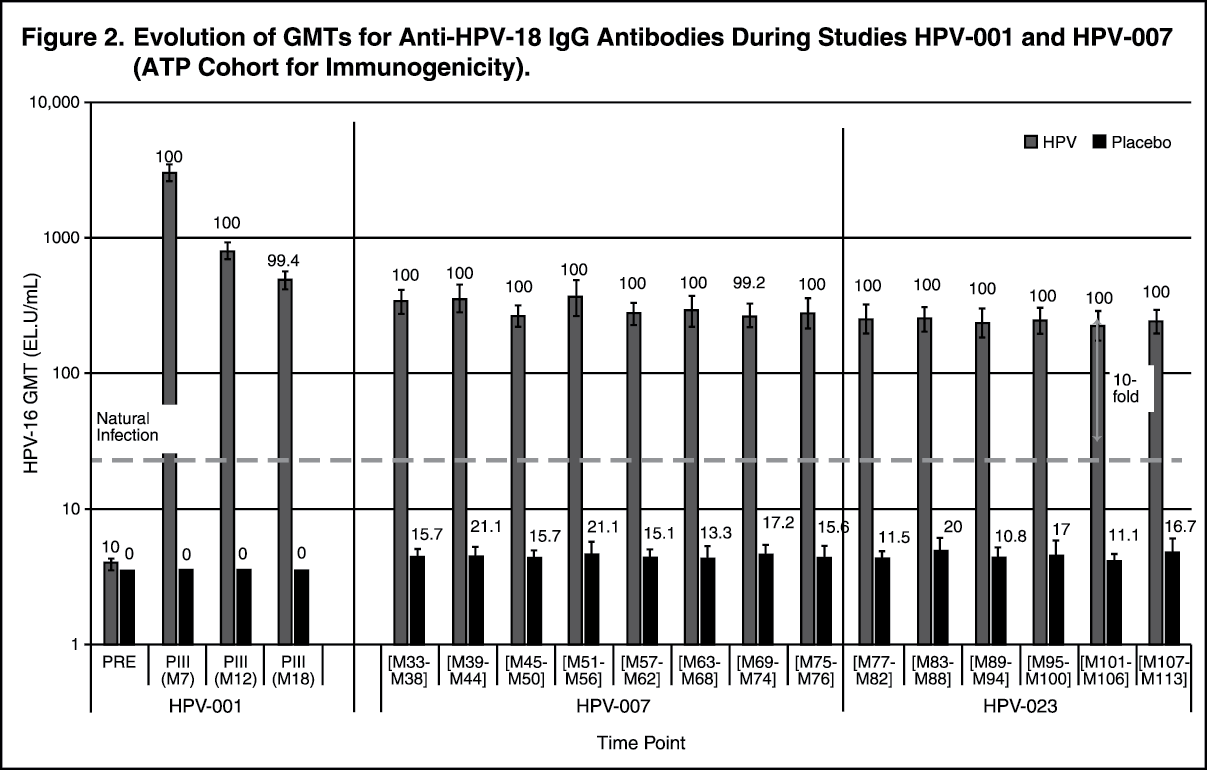 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageVaccine-induced IgG Geometric Mean Titres (GMT) for both HPV-16 and HPV-18 peaked at month 7 and then declined to reach a plateau from month 18 with no substantial decline up to the end of the follow-up period (month 113). At month 113, GMTs for both HPV-16 and HPV-18 were still at least 10-fold higher than titres observed in women previously infected but who cleared HPV infection (natural infection) and 100% of the women were seropositive for both antigens.
In study HPV-008, immunogenicity up to month 48 was similar to the response observed in study HPV-001/007. A similar kinetic profile was observed with the neutralizing antibodies.
Bridging the efficacy of Cervarix demonstrated in 15 to 25 year olds to other age groups: In a pooled analysis, (HPV-029, -030 & -0.48), 99.7% and 100% of females aged 9 years seroconverted to HPV types 16 and 18, respectively after the third dose (at month 7) with GMTs at least 1.4-fold and 2.4-fold higher as compared to females aged 10-14 years and 15 to 25 years, respectively.
In two clinical trials (HPV-012 & -013) performed in girls aged 10 to 14 years, all subjects seroconverted to both HPV type 16 and 18 after the third dose (at month 7) with GMTs at least 2-fold higher as compared to women aged 15 to 25 years.
In an ongoing clinical trial (HPV-070) performed in girls aged 9 to 14 years receiving a 2-dose schedule (0, 6 months or 0, 12 months), all subjects seroconverted to both HPV types 16 and 18 one month after the second dose. The immune response after 2 doses in females aged 9 to 14 years was demonstrated to be non-inferior to the immune response after 3 doses in women aged 15 to 25 years.
The efficacy of Cervarix is inferred on the basis of immunogenicity data observed in girls vaccinated from age 9 to 14 years.
Duration of the immune response in women aged 26 years and older: In the Phase III study (HPV-015) in women 26 years and older all subjects seroconverted one month after the third dose. At the 84-month time point, i.e., 78 months after completion of the full vaccination course, 99.3% and 95.9% of initially seronegative women remained seropositive for anti-HPV-16 and anti-HPV-18 antibodies, respectively. Antibody titres peaked at month 7 then gradually declined up to month 18 and stabilized to reach a plateau up to month 84.
In another clinical study (HPV-014) performed in women aged 15 to 55 years (229 aged 15-25 years, 226 aged 26-45 years and 211 aged 46-55 years), all women were seropositive to both HPV type 16 and 18 after the third dose (at month 7). The GMTs were however, lower in the 26-55 years old population compared to women aged 15 to 25 years. Subjects (142 aged 15-25 years, 172 aged 26-45 years and 156 aged 46-55 years) who completed study HPV-014 and received the 3-dose schedule were followed-up for up to 10 years in the extension study HPV-060. Ten years after administration of the first dose, 100% of subjects in the 15-25 years group, 99.2% in the 26-45 years group and 96.3% in the 46-55 years group were still seropositive for HPV-16, and 99.2%, 93.7% and 83.8% for HPV-18, respectively. In all age groups, GMTs remained 5- to 32-fold for HPV-16 and 3- to 14-fold for HPV-18 above those elicited in women who cleared a natural infection.
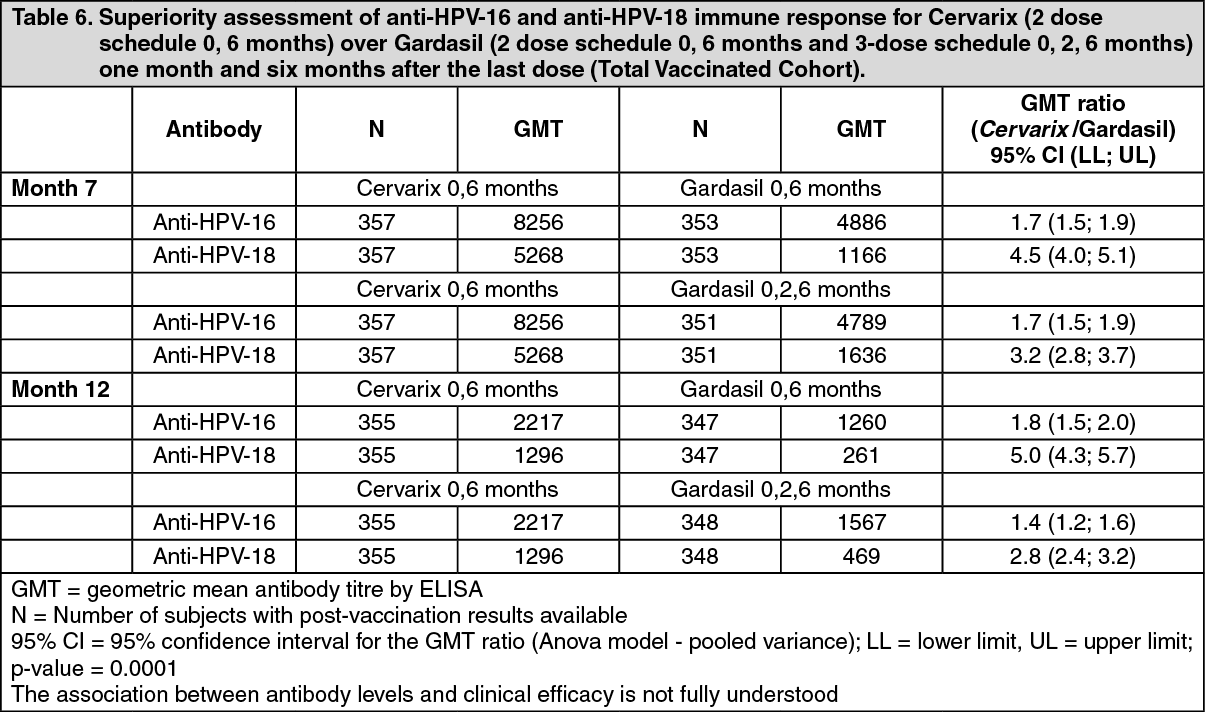
Comparison of immunogenicity of Cervarix and Gardasil: In girls aged 9 to 14 years: In a comparison trial with Gardasil (study HPV-071) in girls aged 9-14 years, superiority of the immune response elicited by Cervarix administered according to the 2-dose schedule 0, 6 months compared to that of Gardasil administered according to the 2-dose 0, 6 months and the standard 3-dose 0, 2, 6 months schedules was demonstrated for both HPV-16 and HPV-18 by ELISA (Table 6). (See Table 6.)
 Click on icon to see table/diagram/image
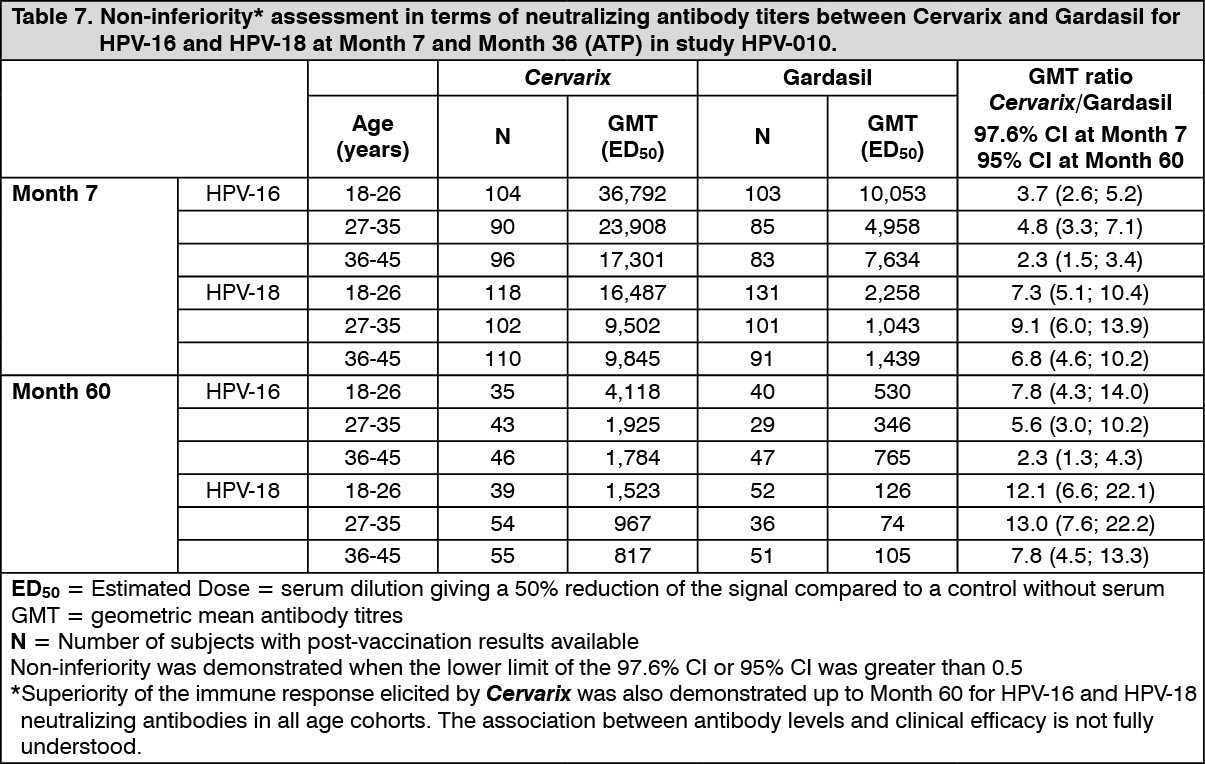
Click on icon to see table/diagram/imageIn women aged 18 to 45 years: In a non-inferiority comparative trial with Gardasil (study HPV-010) in women aged 18-45 years, non-inferiority of the immune response elicited by Cervarix was demonstrated for both HPV-16 and HPV-18 neutralizing antibodies in all age cohorts up to three years after first vaccination (Table 7). (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmunogenicity in HIV infected women: Two clinical studies assessed safety and immunogenicity of Cervarix: A study performed in 120 asymptomatic HIV infected females aged 18 to 25 years (61 subjects received Cervarix) in South Africa (HPV-020).
A comparative study of Cervarix and Gardasil performed in 257 asymptomatic HIV-infected females aged 15-25 years (129 subjects received Cervarix) in Brazil, Estonia, India and Thailand (HPV-019).
In both studies, seroconversion at Month 7 in HIV-infected subjects receiving Cervarix was 100% for both antigens. In HPV-019, seropositivity rate at Month 24 after Cervarix vaccination was 100% for HPV-16 antibodies and >96% for HPV-18 antibodies with a Geometric Mean Concentration (GMC) level more than 12 times higher than the response to natural HPV infection. In both studies the antibody GMCs in HIV-infected subjects appeared lower than in HIV negative subjects. The clinical relevance of this observation is unknown.
In HPV-019, superiority of immune responses (neutralizing antibodies) to both HPV-16 (GMT ratio = 2.74 [95% CI 1.83;4.11]) and HPV-18 (GMT ratio = 7.44 [95% CI 4.79;11.54]) antigens was demonstrated with Cervarix compared to Gardasil, at Month 7 in HIV-infected subjects.
The observed reactogenicity and safety profile of Cervarix in HIV-infected women was in line with the known safety profile in healthy subjects (see Adverse Reactions).
The vaccine did not affect the CD4+ cell count, the HIV viral load and the HIV clinical stage.
Immunogenicity in males aged 10 to 18 years: Immunogenicity in males was assessed in 2 clinical trials HPV-011 (N=173) and HPV-040 (N=556). The data showed comparable immunogenicity in males and females. In study HPV-011, all subjects seroconverted to both HPV-16 and 18 and GMT levels were non inferior to those observed in females aged 15 to 25 years in study HPV-012.
Clinical Studies: See Pharmacodynamics as previously mentioned.
Pharmacokinetics: Evaluation of pharmacokinetic properties is not required for vaccines.
Toxicology: Pre-clinical Safety Data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, acute and repeated dose toxicity, local tolerance, fertility, embryo-foetal and postnatal toxicity (up to the end of the lactation period).