Hematological Effects: Gemcitabine is a myelosuppressant: anemia, leukopenia and thrombocytopenia may occur. Myelosuppression is usually mild to moderate, of short duration, reversible, not cumulative over time, and is more pronounced for the granulocyte count. Anemia is manageable with the use of conventional transfusions. Dose reduction or omission may be necessary for severe leukopenia or thrombocytopenia (see Dosage & Administration). Febrile neutropenia is also commonly reported. Rare cases of petechiae or mild blood loss (hemorrhage) have been reported. Thrombocytosis was reported very rarely.
Gastrointestinal (GI) Effects: Nausea and vomiting were commonly reported but were usually mild to moderate in severity, rarely dose-limiting and easily manageable with standard antiemetics. Diarrhea and stomatitis are commonly reported, but no patient discontinued treatment because of diarrhea. Oral toxicity (soreness or erythema) and mild constipation have been reported rarely.
Hepatic Effects: In clinical studies, gemcitabine was associated with transient elevations in serum transaminases; however, there was no evidence of increasing hepatotoxicity with either longer duration of exposure to gemcitabine or with greater cumulative doses. Elevated liver function test results, including increased concentrations of aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyltransferase (GGT, γ-glutamyltranspeptidase, GGTP), alkaline phosphatase, and bilirubin, have been reported rarely. These effects are usually mild, non-progressive, and rarely necessitate stopping treatment. ALT effects decline over time despite continued treatment. Serious hepatotoxicity, including hepatic failure and death, has been reported very rarely in patients receiving gemcitabine alone or in combination with other potentially hepatotoxic agents.
Genitourinary Effects: Mild proteinuria and hematuria were reported, but are rarely clinically significant and are not usually associated with any change in serum creatinine or BUN. However, a few cases of renal failure of uncertain etiology have been reported and gemcitabine should be used with caution in patients with impaired renal function. Renal failure may be irreversible even with discontinuation of therapy and dialysis may be required. Rare cases of possible HUS have been reported (see Precautions). Cumulative renal toxicity has not been observed.
Fever and Flu-like Symptoms: Gemcitabine may cause fever even in the absence of infections. Fever was frequently associated with other flu-like symptoms and was usually mild and clinically manageable. Reported flu-like symptoms were usually mild, short-lived, and rarely dose-limiting. Individual symptoms of fever, asthenia, anorexia, headache, cough, chills, and myalgia were commonly reported. Fever and asthenia were also reported as isolated symptoms. Insomnia, rhinitis, sweating, and malaise were reported infrequently.
Dermatological Effects: Rash and pruritus were reported in some patients. The rash was usually mild, not dose-limiting, responded to local therapy, and typically a macular or finely granular maculopapular pruritic eruption of mild to moderate severity involving the trunk and extremities. Minimal to moderate hair loss was reported in a few patients. Complete but reversible alopecia was reported rarely. Severe skin reactions, including desquamation and bullous skin eruptions such as toxic epidermal necrolysis (TEN) and Stevens Johnson syndrome (SJS), have been reported very rarely.
Respiratory Effects: Severe and sometimes fatal adverse pulmonary effects, including pulmonary edema, interstitial pneumonitis, pulmonary fibrosis, and adult respiratory distress syndrome (ARDS), have been reported in patients receiving one or more doses of gemcitabine; the drug should be discontinued immediately and appropriate supportive care (e.g., diuretics, bronchodilators, corticosteroids, and/or oxygen) should be promptly provided in patients developing such effects. Onset of pulmonary symptoms has occurred up to 2 weeks following administration of the last dose of gemcitabine, and in rare instances, respiratory failure and death have occurred despite discontinuance of gemcitabine therapy. Dyspnea occurring within hours following gemcitabine injection has been reported in a few patients. This is usually mild and short-lived, rarely dose-limiting and usually abates spontaneously without any specific therapy. Dose-limiting pulmonary toxicity, including pulmonary fibrosis and pneumonitis, occurred in patients receiving gemcitabine and concurrent thoracic radiation therapy for NSCLC. Fatal pulmonary veno-occlusive disease has been reported in a patient who developed progressive dyspnea during gemcitabine therapy.
Edema: Edema, peripheral edema, generalized edema, and some cases of facial edema have been reported. Pulmonary edema was reported rarely. Edema or peripheral edema is usually mild to moderate, rarely dose-limiting, sometimes reported as painful and usually reversible after stopping gemcitabine treatment.
Infection: Infections were reported in a few patients. Sepsis was reported rarely.
Neurological Effects: Mild to moderate somnolence, asthenia and paresthesias were reported.
Extravasation: Gemcitabine is well tolerated during infusion, with only a few cases of injection site reaction reported. There have been no reports of injection site necrosis. Gemcitabine is not a vesicant.
Hypersensitivity: Rash and pruritus have been reported. The rash is usually mild, not dose-limiting, and responds to local therapy. Desquamation, vesiculation and ulceration have been reported rarely. Bronchospasm is usually mild and transient, but parenteral therapy may be required.
Cardiovascular Effects: Cardiovascular toxicity, including chest pain, congestive heart failure, myocardial infarction, arrhythmias (predominantly supraventricular), cerebrovascular accident, hypotension, and hypertension have been reported rarely.
Many of these patients had a prior history of cardiovascular disease. Clinical signs of peripheral vasculitis and gangrene have been reported very rarely.
Injury, Poisoning and Procedural Complications: Radiation toxicity and radiation recall reactions have been reported.


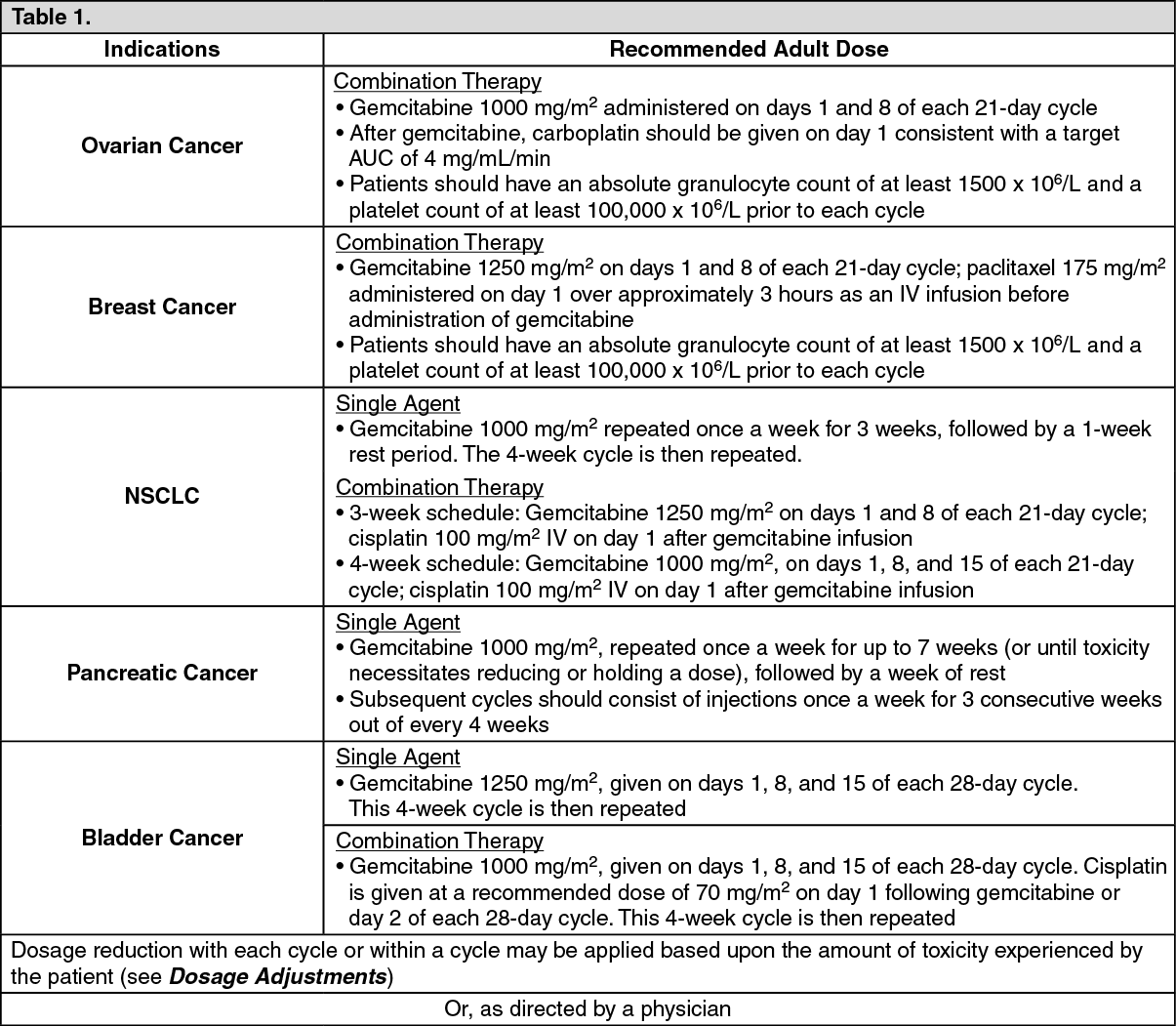 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image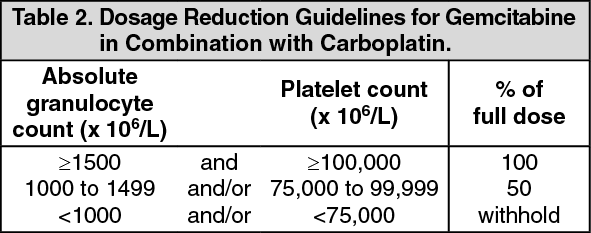 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image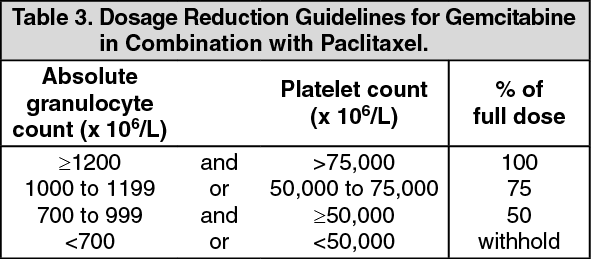 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image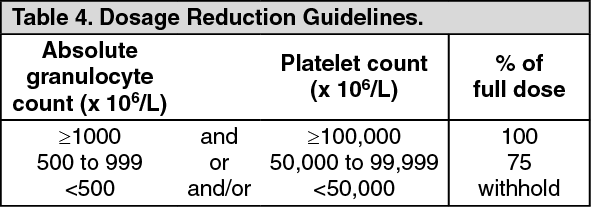 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 200 mgce3f2741-620e-473f-9b89-a799010397f1.GIF)

 Sign Out
Sign Out