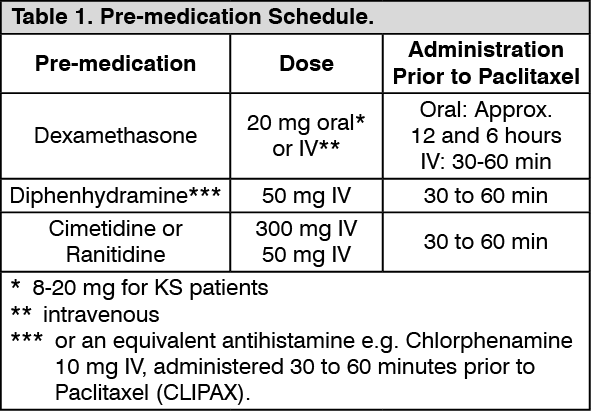
Unless otherwise noted, the following discussion refers to the overall safety database of 812 patients with solid tumors treated with single-agent Paclitaxel in clinical studies.
The frequency and severity of undesirable effects, unless otherwise mentioned, are generally similar between patients receiving Paclitaxel for the treatment of ovarian carcinoma, breast carcinoma, or NSCLC. None of the observed toxicities were clearly influenced by age.
The most frequent significant undesirable effect was bone marrow suppression. Severe neutropenia (<0.5 x 10
9/l) occurred in 28% of patients, but was not associated with febrile episodes. Only 1% of patients experienced severe neutropenia for ≥7 days. Thrombocytopenia was reported in 11% of patients. Three percent of patients had a platelet count nadir <50 x 10
9/l at least once while on study. Anaemia was observed in 64% of patients, but was severe (Hb <8.1 g/dl) in only 6% of patients. Incidence and severity of anaemia is related to baseline haemoglobin status.
Neurotoxicity, mainly peripheral neuropathy, appeared to be more frequent and severe with a 175 mg/m
2 3-hour infusion (85% neurotoxicity, 15% severe) than with a 135 mg/m
2 24-hour infusion (25% peripheral neuropathy, 3% severe) when Paclitaxel was combined with Cisplatin. In NSCLC patients and in ovarian cancer patients treated with Paclitaxel over 3 hours followed by Cisplatin, there is an apparent increase in the incidence of severe neurotoxicity. Peripheral neuropathy can occur following the first course and can worsen with increasing exposure to Paclitaxel. Peripheral neuropathy was the cause of Paclitaxel discontinuation in a few cases. Sensory symptoms have usually improved or resolved within several months of Paclitaxel discontinuation. Pre-existing neuropathies resulting from prior therapies are not a contraindication for Paclitaxel therapy.
Arthralgia or myalgia
affected 60% of patients and was severe in 13% of patients.
A significant hypersensitivity reaction with possible fatal outcome (defined as hypotension requiring therapy, angioedema, respiratory distress requiring bronchodilator therapy, or generalized urticaria) occurred in two (< 1%) patients. Thirty-four percent of patients (17% of all courses) experienced minor hypersensitivity reactions. These minor reactions, mainly flushing and rash, did not require therapeutic intervention nor did they prevent continuation of Paclitaxel therapy.
Injection site reactions during intravenous administration may lead to localized oedema, pain, erythema, and induration; on occasion, extravasation can result in cellulitis. Skin sloughing and/or peeling has been reported, sometimes related to extravasation. Skin discoloration may also occur. Recurrence of skin reactions at a site of previous extravasation following administration of Paclitaxel at a different site, i.e. "recall", has been reported rarely. A specific treatment for extravasation reactions is unknown at this time. In some cases, the onset of the injection site reaction either occurred during a prolonged infusion or was delayed by a week to 10 days.
The data as follows lists undesirable effects regardless of severity associated with the administration of single agent Paclitaxel administered as a three hour infusion in the metastatic setting (812 patients treated in clinical studies) and as reported in the post-marketing surveillance* of Paclitaxel.
The frequency of undesirable effects listed as follows is defined using the following convention: Very common (≥1/10); common (≥1/100, <1/10); uncommon (≥1/1,000, <1/100); rare (≥1/10,000, <1/1,000); very rare (<1/10,000). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Breast cancer patients who received Paclitaxel in the adjuvant setting following AC experienced more neurosensory toxicity, hypersensitivity reactions, arthralgia/myalgia, anaemia, infection, fever, nausea/vomiting and diarrhoea than patients who received AC alone. However, the frequency of these events was consistent with the use of single agent Paclitaxel, as reported previously.
Combination treatment: The following discussion refers to two major trials for the first-line chemotherapy of ovarian carcinoma (Paclitaxel + Cisplatin, over 1050 patients); two phase III trials in the first line treatment of metastatic breast cancer: one investigating the combination with Doxorubicin (Paclitaxel + Doxorubicin: 267 patients), and another investigating the combination with Trastuzumab (planned subgroup analysis, Paclitaxel Trastuzumab: 188 patients) and two phase III trials for the treatment of advanced NSCLC (Paclitaxel + Cisplatin: over 360 patients).
When administered as a three hour infusion for the first-line chemotherapy of ovarian cancer, neurotoxicity, arthralgia/myalgia, and hypersensitivity were reported as more frequent and severe by patients treated with Paclitaxel followed by Cisplatin than patients treated with Cyclophosphamide followed by Cisplatin.
Myelosuppression appeared to be less frequent and severe with Paclitaxel as a three hour infusion followed by Cisplatin compared with Cyclophosphamide followed by Cisplatin.
For the first line chemotherapy of metastatic breast cancer, neutropenia, anaemia, peripheral neuropathy, arthralgia/myalgia, asthenia, fever, and diarrhoea were reported more frequently and with greater severity when Paclitaxel (220 mg/m
2) was administered as a 3-hour infusion 24 hours following Doxorubicin (50 mg/m
2) when compared to standard FAC therapy (5-FU 500 mg/m
2, Doxorubicin 50 mg/m
2, Cyclophosphamide 500 mg/m
2). Nausea and vomiting appeared to be less frequent and severe with the Paclitaxel (220 mg/m
2)/Doxorubicin (50 mg/m
2) regimen as compared to the standard FAC regimen. The use of corticosteroids may have contributed to the lower frequency and severity of nausea and vomiting in the Paclitaxel/Doxorubicin arm.
When Paclitaxel was administered as a 3-hour infusion in combination with Trastuzumab for the first line treatment of patients with metastatic breast cancer, the following events (regardless of relationship to Paclitaxel or Trastuzumab) were reported more frequently than with single agent Paclitaxel: heart failure (8% vs 1%), infection (46% vs 27%), chills (42% vs 4%), fever (47% vs 23%), cough (42% vs 22%), rash (39% vs 18%), arthralgia (37% vs 21%), tachycardia (12% vs 4%), diarrhoea (45% vs 30%), hypertonia (11% vs 3%), epistaxis (18% vs 4%), acne (11% vs 3%), herpes simplex (12% vs 3%), accidental injury (13% vs 3%), insomnia (25% vs 13%), rhinitis (22% vs 5%), sinusitis (21% vs 7%), and injection site reaction (7% vs 1%). Some of these frequency differences may be due to the increased number and duration of treatments with Paclitaxel/Trastuzumab combination vs single agent Paclitaxel. Severe events were reported at similar rates for Paclitaxel/Trastuzumab and single agent Paclitaxel.
When Doxorubicin was administered in combination with Paclitaxel in metastatic breast cancer, cardiac contraction abnormalities (a 20% reduction of left ventricular ejection fraction) were observed in 15% of patients vs. 10% with standard FAC regimen. Congestive heart failure was observed in < 1% in both Paclitaxel/Doxorubicin and standard FAC arms. Administration of Trastuzumab in combination with Paclitaxel in patients previously treated with anthracyclines resulted in an increased frequency and severity of cardiac dysfunction in comparison with patients treated with Paclitaxel single agent (New York Heart Association (NYHA) Class I/II 10% vs. 0%; NYHA Class III/IV 2% vs. 1%) and rarely has been associated with death. In all but these rare cases, patients responded to appropriate medical treatment.
Radiation pneumonitis has been reported in patients receiving concurrent radiotherapy.
AIDS-related Kaposi's sarcoma: Except for haematologic and hepatic undesirable effects, the frequency and severity of undesirable effects are generally similar between KS patients and patients treated with paclitaxel monotherapy for other solid tumours, based on a clinical study including 107 patients.
Blood and the lymphatic system disorders: Bone marrow suppression was the major dose-limiting toxicity. Neutropenia is the most important haematological toxicity. During the first course of treatment, severe neutropenia (<0.5 x 10
9/l) occurred in 20% of patients. During the entire treatment period, severe neutropenia was observed in 39% of patients. Neutropenia was present for >7 days in 41% and for 30-35 days in 8% of patients. It resolved within 35 days in all patients who were followed. The incidence of Grade 4 neutropenia lasting ≥7 days was 22%.
Neutropenic fever related to Paclitaxel was reported in 14% of patients and in 1.3% of treatment cycles. There were 3 septic episodes (2.8%) during Paclitaxel administration related to the medicinal product that proved fatal.
Thrombocytopenia was observed in 50% of patients, and was severe (<50 x 10
9/l) in 9%. Only 14% experienced a drop in their platelet count <75 x 10
9/l, at least once while on treatment. Bleeding episodes related to Paclitaxel were reported in <3% of patients, but the haemorrhagic episodes were localised. Anaemia (Hb <11 g/dl) was observed in 61% of patients and was severe (Hb <8 g/dl) in 10%. Red cell transfusions were required in 21% of patients.
Hepatobiliary disorders: Among patients (>50% on protease inhibitors) with normal baseline liver function, 28%, 43% and 44% had elevations in bilirubin, alkaline phosphatase and AST (SGOT), respectively. For each of these parameters, the increases were severe in 1% of cases.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image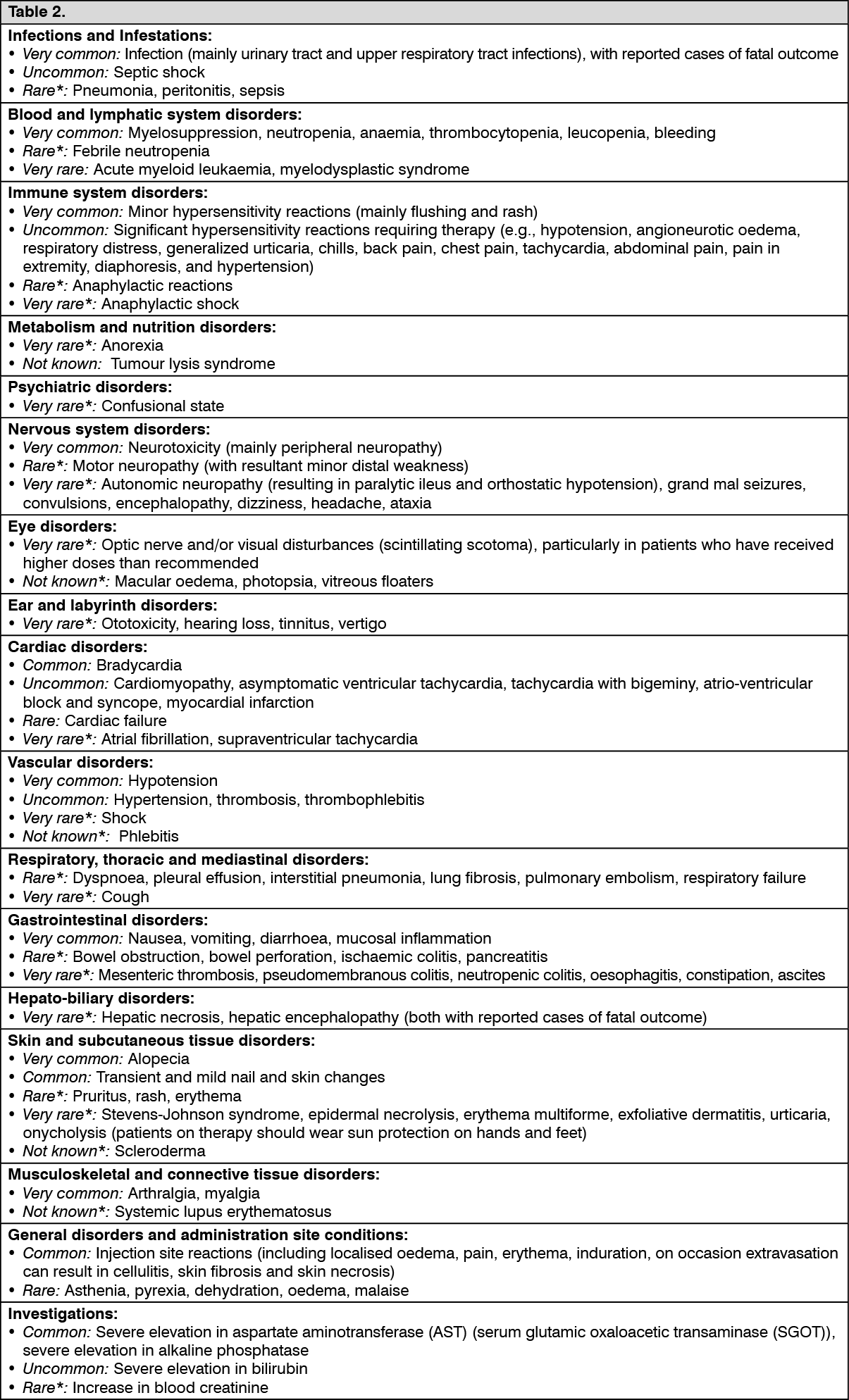 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out