Valsartan, hydrochlorothiazide.
One tablet contains 80 mg valsartan and 12.5 mg hydrochlorothiazide, or 160 mg valsartan and 12.5 mg hydrochlorothiazide, or 160 mg valsartan and 25 mg hydrochlorothiazide, or 320 mg valsartan and 12.5 mg hydrochlorothiazide, or 320 mg valsartan and 25 mg hydrochlorothiazide.
Co-Diovan FCT cannot be divided into equal doses.
Excipients/Inactive Ingredients: 80/12.5 mg: Colloidal silicon dioxide; crospovidone; hydroxypropyl methylcellulose; magnesium stearate; microcrystalline cellulose; polyethylene glycol; talc; titanium dioxide (E171); red iron oxide (E172); yellow iron oxide (E172).
160/12.5 mg: Colloidal silicon dioxide; crospovidone; hydroxypropyl-methylcellulose; magnesium stearate; microcrystalline cellulose; polyethylene glycol; talc; titanium dioxide (E171); red iron oxide (E172).
160/25 mg: Colloidal silicon dioxide; crospovidone; hydroxypropyl methylcellulose; magnesium stearate; microcrystalline cellulose; polyethylene glycol; talc; titanium dioxide (E171), red iron oxide (E172), yellow iron oxide (E172), black iron oxide (E172).
320/12.5 mg: Colloidal silicon dioxide; crospovidone; hydroxypropyl-methylcellulose; magnesium stearate; microcrystalline cellulose; polyethylene glycol; talc; black iron oxide (E172), titanium dioxide (E171); red iron oxide (E172).
320/25 mg: Colloidal silicon dioxide; crospovidone; hydroxypropyl-methylcellulose; magnesium stearate; microcrystalline cellulose; polyethylene glycol; talc; titanium dioxide (E171); yellow iron oxide (E172).
Pharmacotherapeutic group: Angiotensin II antagonists combination (valsartan) with diuretics (hydrochlorothiazide). ATC code: C09D A03.
Pharmacology: Pharmacodynamics: The active hormone of the RAAS is angiotensin II, which is formed from angiotensin I through ACE. Angiotensin II binds to specific receptors located in the cell membranes of various tissues. It has a wide variety of physiological effects, including in particular both direct and indirect involvement in the regulation of blood pressure. As a potent vasoconstrictor, angiotensin II exerts a direct pressor response. In addition, it promotes sodium retention and stimulation of aldosterone secretion.
Valsartan is an orally active and specific angiotensin II (Ang II) receptor antagonist. It acts selectively on the AT1 receptor subtype, which is responsible for the known actions of angiotensin II. The increased plasma levels of Ang II following AT1 receptor blockade with valsartan may stimulate the unblocked AT2 receptor, which appears to counterbalance the effect of the AT1 receptor. Valsartan does not exhibit any partial agonist activity at the AT1 receptor and has much (about 20,000 fold) greater affinity for the AT1 receptor than for the AT2 receptor.
Valsartan does not inhibit ACE, also known as kininase II, which converts Ang I to Ang II and degrades bradykinin. No potentiation of bradykinin-related side effects should be expected. In clinical trials where valsartan was compared with an ACE inhibitor, the incidence of dry cough was significantly (P < 0.05) less in patients treated with valsartan than in those treated with an ACE inhibitor (2.6% versus 7.9% respectively). In a clinical trial of patients with a history of dry cough during ACE inhibitor therapy, 19.5% of trial subjects receiving valsartan and 19.0% of those receiving a thiazide diuretic experienced cough, compared to 68.5% of those treated with an ACE inhibitor (P < 0.05). Valsartan does not bind to or block other hormone receptors or ion channels known to be important in cardiovascular regulation.
The site of action of thiazide diuretics is primarily in the renal distal convoluted tubule. It has been shown that there is a high affinity receptor in the renal cortex with the primary binding site for the thiazide diuretic action and inhibition of NaCl transport in the distal convoluted tubule. The mode of action of thiazides is through inhibition of the Na+Cl- symporter perhaps by competing for the Cl--site affecting mechanisms of electrolyte reabsorption: - directly increasing excretion of sodium and chloride in approximately equivalent amounts, - indirectly, diuretic action reducing plasma volume, with consequent increases in plasma renin activity, increases in aldosterone secretion, increases in urinary potassium loss, and decreases in serum potassium. The renin-aldosterone link is mediated by angiotensin II, so co-administration of an angiotensin II receptor antagonist tends to reverse the potassium loss associated with these diuretics.
Non-melanoma skin cancer: Based on available data from epidemiological studies, cumulative dose-dependent association between HCTZ and NMSC has been observed. One study included a population comprised of 71,533 cases of BCC and of 8,629 cases of SCC matched to 1,430,833 and 172,462 population controls, respectively. High HCTZ use (≥50,000 mg cumulative) was associated with an adjusted OR of 1.29 (95% CI: 1.23-1.35) for BCC and 3.98 (95% CI: 3.68-4.31) for SCC. A clear cumulative dose response relationship was observed for both BCC and SCC. Another study showed a possible association between lip cancer (SCC) and exposure to HCTZ: 633 cases of lip-cancer were matched with 63,067 population controls, using a risk-set sampling strategy. A clear cumulative dose-response relationship was demonstrated with an adjusted OR 2.1 (95% CI: 1.7-2.6) increasing to OR 3.9 (3.0-4.9) for high use (~25,000 mg) and OR 7.7 (5.7-10.5) for the highest cumulative dose (~100,000 mg). For example: A 100,000 mg cumulative dose corresponds to more than 10 years' daily use with a defined daily dose of 25 mg (see PRECAUTIONS and ADVERSE REACTIONS).
CLINICAL STUDIES: Administration of valsartan to patients with hypertension results in reduction of blood pressure without affecting pulse rate.
In most patients, after administration of a single oral dose, onset of antihypertensive activity occurs within 2 hours, and the peak reduction of blood pressure is achieved within 4 to 6 hours. The antihypertensive effect persists over 24 hours after dosing. During repeated dosing, the maximum reduction in blood pressure with any dose is generally attained within 2 to 4 weeks and is sustained during long-term therapy. Combined with hydrochlorothiazide, a significant additional reduction in blood pressure is achieved.
Initial therapy with valsartan/HCTZ combination starting with a dose of 160/12.5 mg produced significantly greater reductions in blood pressure compared to valsartan monotherapy starting with a dose of 160 mg after 4 weeks in patients with severe hypertension (sitting diastolic blood pressure 110 mmHg and systolic blood pressure 140 mmHg). In other studies, the probability of achieving systolic or diastolic blood pressure control was greater with initial combination therapy than valsartan and HCTZ monotherapy at all levels of baseline blood pressure.
Pharmacokinetics: Valsartan: Absorption: Following oral administration of valsartan alone, peak plasma concentrations of valsartan are reached in 2-4 hours. Mean absolute bioavailability is 23%. When valsartan is given with food, the area under the plasma concentration curve (AUC) of valsartan is reduced by 48%, although from about 8 hours post dosing plasma valsartan concentrations are similar for the fed and fasted group. This reduction in AUC is not, however, accompanied by a clinically significant reduction in the therapeutic effect, and valsartan can therefore be given either with or without food.
Distribution: The steady-state volume of distribution of valsartan after intravenous administration is about 17 liters, indicating that valsartan is not distributed into tissues extensively. Valsartan is highly bound to serum proteins (94-97%), mainly serum albumin.
Biotransformation/Metabolism: Valsartan is not bio-transformed to a high extent as only about 20% of dose is recovered as metabolites. A hydroxy metabolite has been identified in plasma at low concentrations (less than 10% of the valsartan AUC). This metabolite is pharmacologically inactive.
Elimination: Valsartan shows multi-exponential decay kinetics (t½ α < 1 h and t½ β about 9 h). Valsartan is primarily eliminated in feces (about 83% of dose) and urine (about 13% of dose), mainly as unchanged drug. Following intravenous administration, plasma clearance of valsartan is about 2 L/h and its renal clearance is 0.62 L/h (about 30% of total clearance). The half-life of valsartan is 6 hours.
The pharmacokinetics of valsartan is linear in the dose range tested. There is no change in the kinetics of valsartan on repeated administration, and little accumulation when dosed once daily. Plasma concentrations were observed to be similar in males and females.
Hydrochlorothiazide: Absorption: The absorption of hydrochlorothiazide, after an oral dose, is rapid (Tmax about 2 h). The increase in mean AUC is linear and dose proportional in the therapeutic range. Concomitant administration with food has been reported to both increase and decrease the systemic availability of hydrochlorothiazide compared with the fasted state. The magnitude of these effects is small and has little clinical importance. Absolute bioavailability of hydrochlorothiazide is 70% after oral administration.
Distribution: The distribution and elimination kinetics have generally been described as a bi-exponential decay function. The apparent volume of distribution is 4-8 L/kg. Circulating hydrochlorothiazide is bound to serum proteins (40-70%), mainly serum albumin. Hydrochlorothiazide also accumulates in erythrocytes at approximately 3 times the level in plasma.
Biotransformation: Hydrochlorothiazide is eliminated predominantly as unchanged drug.
Elimination: Hydrochlorothiazide is eliminated from plasma with a half-life averaging 6 to 15 hours in the terminal elimination phase. There is no change in the kinetics of hydrochlorothiazide on repeated dosing, and accumulation is minimal when dosed once daily. More than 95% of the absorbed dose is excreted as unchanged compound in the urine.
Valsartan/hydrochlorothiazide: The systemic availability of hydrochlorothiazide is reduced by about 30% when co-administered with valsartan. The kinetics of valsartan is not markedly affected by the co-administration of hydrochlorothiazide. This observed interaction has no impact on the combined use of valsartan and hydrochlorothiazide, since controlled clinical trials have shown a clear antihypertensive effect, greater than that obtained with drug given alone, or placebo.
Special Populations: Geriatric patients (aged 65 years or above): A somewhat higher systemic exposure to valsartan was observed in some elderly subjects than in young subjects; however, this has not been shown to have any clinical significance.
Limited data suggest that the systemic clearance of hydrochlorothiazide is reduced in both healthy and hypertensive elderly subjects compared to young healthy volunteers.
Renal Impairment: No dose adjustment is required for patients with a Glomerular Filtration Rate (GFR) of 30 to 70 mL/min.
In patients with severe renal impairment (GFR < 30 mL/min) and patients undergoing dialysis, no data are available for valsartan + hydrochlorothiazide (Co-Diovan). Valsartan is highly bound to plasma protein, and is not to be removed by dialysis, whereas clearance of hydrochlorothiazide will be achieved by dialysis.
In the presence of renal impairment, mean peak plasma levels and AUC values of hydrochlorothiazide are increased and the urinary excretion rate is reduced. In patients with mild to moderate renal impairment, the mean elimination half-life is almost doubled. The renal clearance of hydrochlorothiazide is also reduced to a great extent compared with the renal clearance of around 300 mL/min in patients with normal renal function. Therefore, use with caution in patients with severe renal impairment (GFR < 30 mL/min) (see PRECAUTIONS).
Hepatic impairment: In a pharmacokinetics trial in patients with mild (n=6) to moderate (n=5) hepatic dysfunction, exposure to valsartan was increased approximately twofold compared with healthy volunteers. There is no data available on the use of valsartan in patients with severe hepatic dysfunction.
Hepatic disease does not significantly affect the pharmacokinetics of hydrochlorothiazide, and no dose reduction is considered necessary.
Use with particular caution in patients with biliary obstructive disorders and severe hepatic impairment (see PRECAUTIONS).
Toxicology: NON-CLINICAL SAFETY DATA: Valsartan: hydrochlorothiazide: In a variety of preclinical safety studies conducted in several animal species, there were no findings that would exclude the use of therapeutic doses of valsartan:hydrochlorothiazide in humans. High doses of valsartan:hydrochlorothiazide (100:31.25 to 600:187.5 mg/kg body weight) caused, in rats, a reduction of red blood cell parameters (erythrocytes, hemoglobin, hematocrit) and evidence of changes in renal hemodynamics (moderate to severe raised plasma urea, increases in plasma potassium and magnesium and mild increases in urinary volume and electrolytes, minimal to slight tubular basophilia, and afferent arteriolar hypertrophy at the highest dose level). In marmosets (30:9.375 to 400:125 mg/kg), the changes were fairly similar though more severe, particularly at the higher dose levels and in the kidney, where the changes developed to a nephropathy, which included raised urea and creatinine. Marmosets also had gastrointestinal mucosal changes at 30:9.373 to 400:125 mg/kg.
Hypertrophy of the renal juxtaglomerular cells was also seen in rats and marmosets. All changes were considered to be caused by the pharmacological action of valsartan:hydrochlorothiazide which is synergistic (potentiation is about tenfold compared to valsartan alone) rather than additive, producing prolonged hypotension particularly in marmosets. For therapeutic doses of valsartan:hydrochlorothiazide in humans, the hypertrophy of the renal juxtaglomerular cells does not seem to have any relevance. The main preclinical safety findings are attributed to the pharmacological action of the compounds which appear to act synergistically with no evidence of any interaction between the two compounds. In the clinic, the actions of the two compounds are additive, and the preclinical findings have not been demonstrated to have any clinical significance. The combination valsartan:hydrochlorothiazide was not tested for mutagenicity, clastogenicity or carcinogenicity as there was no evidence for any interaction between the two compounds.
Valsartan: Preclinical data revealed no special hazard for humans based on conventional studies of safety pharmacology, genotoxicity, carcinogenic potential and effects on fertility.
Safety pharmacology and Long term toxicity: In a variety of preclinical safety studies conducted in several animal species, there were no findings that would exclude the use of therapeutic doses of valsartan in humans.
In preclinical safety studies, high doses of valsartan (200 to 600 mg/kg/day body weight) caused in rats a reduction of red blood cell parameters (erythrocytes, hemoglobin, hematocrit) and evidence of changes in renal hemodynamics (slightly raised blood urea nitrogen, and renal tubular hyperplasia and basophilia in males). These doses in rats (200 and 600 mg/kg/day) are approximately 6 and 18 times the maximum recommended human dose on a mg/m2 basis (calculations assume an oral dose of 320 mg/day and a 60-kg patient). In marmosets at comparable doses, the changes were similar though more severe, particularly in the kidney where the changes developed to a nephropathy including raised blood urea nitrogen and creatinine. Hypertrophy of the renal juxtaglomerular cells was also seen in both species. All changes were considered to be caused by the pharmacological action of valsartan which produces prolonged hypotension, particularly in marmosets. For therapeutic doses of valsartan in humans, the hypertrophy of the renal juxtaglomerular cells does not seem to have any relevance.
Reproductive toxicity: Valsartan had no adverse effects on the reproductive performance of male or female rats at oral doses up to 200 mg/kg/day, approximately 6 times the maximum recommended human dose on a mg/m2 basis (calculations assume an oral dose of 320 mg/day and a 60-kg patient).
Mutagenicity: Valsartan was devoid of mutagenic potential at either the gene or chromosome level when investigated in various standard in vitro and in vivo genotoxicity studies.
Carcinogenicity: There was no evidence of carcinogenicity when valsartan was administered in the diet to mice and rats for 2 years at doses up to 160 and 200 mg/kg/day, respectively.
Hydrochlorothiazide: Hydrochlorothiazide has been tested for mutagenicity, clastogenicity, reproductive performance and carcinogenicity with negative results.
According to the experimental data available, hydrochlorothiazide did not reveal evidence of carcinogenic activity in rats and mice (hepatocellular tumors in mice were only seen in the high-dosed males; the incidence did not exceed those levels historically found in controls).
The mutagenic potential was assessed in a series of in vitro and in vivo test systems. While some positive results were obtained in vitro, all in vivo studies provided negative results. Hydrochlorothiazide enhanced the UVA-induced formation of pyrimidine dimers in vitro and in the skin of mice following oral treatment. It is therefore concluded that there is no relevant mutagenic potential in vivo, although hydrochlorothiazide could enhance the genotoxic effects of UVA light.
Treatment of hypertension in adults, 18 years of age and older.
Treatment of hypertension in patients whose blood pressure is not adequately controlled by monotherapy.
As initial therapy in patients who are likely to need multiple drugs to achieve blood pressure goals. The choice as initial therapy for hypertension should be based on an assessment of potential benefits and risks.
Dosage regimen: The recommended dose is 1 coated tablet per day. When clinically appropriate either 80 mg valsartan and 12.5 mg hydrochlorothiazide or 160 mg valsartan and 12.5 mg hydrochlorothiazide or 320 mg valsartan and 12.5 mg hydrochlorothiazide may be used. When necessary 160 mg valsartan and 25 mg hydrochlorothiazide or 320 mg valsartan and 25 mg hydrochlorothiazide may be used.
For initial therapy, the usual starting dose is 160/12.5 mg once daily. The dosage can be increased after 1 to 2 weeks of therapy to a maximum of one 320/25 mg tablet once daily as needed to control blood pressure. The medication is not recommended as initial therapy in patients with intravascular volume depletion (see PRECAUTIONS).
The maximum daily dose is 320 mg/25 mg.
The maximum antihypertensive effect is seen within 2 to 4 weeks.
Renal impairment: No dosage adjustment is required for patients with mild to moderate renal impairment (Glomerular Filtration Rate (GFR) ≥30 mL/min). Due to the hydrochlorothiazide component, use is contraindicated in patients with anuria (see CONTRAINDICATIONS) and should be used with caution in patients with severe renal impairment (GFR < 30 mL/min) (see PRECAUTIONS and PHARMACOLOGY under ACTIONS). Thiazide diuretics are ineffective as monotherapy in severe renal impairment (GFR < 30 mL/min) but may be useful in these patients, when used with due caution in combination with a loop diuretic even in patients with GFR < 30 mL/min.
Hepatic impairment: No dosage adjustment is required in patients with mild to moderate hepatic impairment. Due to the hydrochlorothiazide component, use with particular caution in patients with severe hepatic impairment. Due to the valsartan component, use with particular caution in patients with biliary obstructive disorders (see PRECAUTIONS).
Pediatrics Patients (below 18 years): Safety and efficacy have not been established in children below the age of 18 years.
Overdose with valsartan may result in marked hypotension, which could lead to depressed level of consciousness, circulatory collapse and/or shock. If the ingestion is recent, vomiting should be induced. Otherwise, the usual treatment would be i.v. infusion of normal saline solution.
Valsartan cannot be eliminated by means of hemodialysis because of its strong plasma binding behavior, whereas clearance of hydrochlorothiazide will be achieved by dialysis.
Known hypersensitivity to valsartan, hydrochlorothiazide, other sulphonamide derived medicinal products or to any of the excipients.
Pregnancy (see USE IN PREGNANCY & LACTATION).
Because of hydrochlorothiazide, use is contraindicated in patients with anuria.
Concomitant use of angiotensin receptor antagonists (ARBs)-including valsartan- or of angiotensin-converting enzyme inhibitors (ACEIs) with aliskiren in patients with Type 2 diabetes (see Dual RAS blockade under INTERACTIONS).
Serum electrolyte changes: Concomitant use with potassium supplements, potassium-sparing diuretics, salt substitutes containing potassium, or other drugs that may increase potassium levels (heparin, etc.) should be used with caution. Thiazide diuretics can precipitate new onset hypokalemia or exacerbate pre-existing hypokalemia. Thiazide diuretics should be administered with caution in patients with conditions involving enhanced potassium loss, for example salt-losing nephropathies and prerenal (cardiogenic) impairment of kidney function. If hypokalemia is accompanied by clinical signs (e.g. muscular weakness, paresis, or ECG alterations), use should be discontinued. Correction of hypokalemia and any coexisting hypomagnesemia is recommended prior to the initiation of thiazides. Potassium and magnesium serum concentrations should be checked periodically. All patients receiving thiazide diuretics should be monitored for imbalances in electrolytes, particularly potassium.
Thiazide diuretics can precipitate new onset hyponatremia and hypochloremic alkalosis or exacerbate pre-existing hyponatremia. Hyponatremia, accompanied by neurological symptoms (nausea, progressive disorientation, apathy) has been observed in isolated cases. Regular monitoring of serum sodium concentrations is recommended.
Patients with sodium- and/or volume-depletion: In severely sodium-depleted and/or volume-depleted patients, such as those receiving high doses of diuretics, symptomatic hypotension may occur in rare cases after initiation of therapy. Valsartan + hydrochlorothiazide (Co-Diovan) should be used only after correction of any pre-existing sodium and/or volume depletion otherwise the treatment should start under close medical supervision.
If hypotension occurs, the patient should be placed in the supine position and, if necessary, given an i.v. infusion of normal saline. Treatment can be continued once the blood pressure has stabilized.
Patients with renal artery stenosis: Valsartan + hydrochlorothiazide (Co-Diovan) should be used with caution to treat hypertension in patients with unilateral or bilateral renal artery stenosis or stenosis to a solitary kidney, since blood urea and serum creatinine may increase in such patients.
Patients with renal impairment: No dosage adjustment is required for patients with mild to moderate renal impairment (GFR ≥ 30 mL/min). Due to the hydrochlorothiazide component, use with caution in severe renal impairment (GFR < 30 mL/min). Thiazide diuretics may precipitate azotemia in patients with chronic kidney disease. They are ineffective as monotherapy in severe renal impairment (GFR < 30 mL/min) but may be useful, when used with due caution in combination with loop diuretics even in patients with GFR < 30 mL/min (see DOSAGE & ADMINISTRATION and PHARMACOLOGY: PHARMACOKINETICS under ACTIONS).
The use of ARBs-including valsartan- or of ACEIs with aliskiren should be avoided in patients with severe renal impairment (GFR < 30 mL/min) (see Dual blockade of the RAS under INTERACTIONS).
Patients with hepatic impairment: In patients with mild to moderate hepatic impairment no dosage adjustment is required. Use with particular caution in patients with biliary obstructive disorders and in patients with severe hepatic impairment (see DOSAGE & ADMINISTRATION and PHARMACOLOGY: PHARMACOKINETICS under ACTIONS).
Angioedema: Angioedema, including swelling of the larynx and glottis, causing airway obstruction and/or swelling of the face, lips, pharynx, and/or tongue has been reported in patients treated with valsartan; some of these patients previously experienced angioedema with other drugs including ACE inhibitors. Treatment should be immediately discontinued in patients who develop angioedema, and should not be re-administered.
Systemic lupus erythematosus: Thiazide diuretics, including hydrochlorothiazide, have been reported to exacerbate or activate systemic lupus erythematosus.
Other metabolic disturbances: Thiazide diuretics, including hydrochlorothiazide, may alter glucose tolerance and raise serum levels of cholesterol and triglycerides.
Like other diuretics, hydrochlorothiazide may raise the serum uric acid level due to reduced clearance of uric acid and may cause or exacerbate hyperuricemia and precipitate gout in susceptible patients.
Thiazides decrease urinary calcium excretion and may cause mild elevation of serum calcium in the absence of known disorders of calcium metabolism. Since hydrochlorothiazide can increase serum calcium concentrations, it should be used with caution in patients with hypercalcemia. Marked hypercalcemia unresponsive to thiazide withdrawal or ≥12 mg/dL may be evidence of an underlying thiazide independent hypercalcemic process.
Pathological changes in the parathyroid gland of patients with hypercalcemia and hypophosphatemia have been observed in a few patients on prolonged thiazide therapy. If hypercalcemia occurs, further diagnostic clarification is necessary.
General: Hypersensitivity reactions to hydrochlorothiazide are more likely in patients with allergy and asthma.
Acute Angle-Closure Glaucoma: Hydrochlorothiazide, a sulfonamide, has been associated with an idiosyncratic reaction resulting in acute transient myopia and acute angle-closure glaucoma. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of a drug initiation. Untreated acute-angle closure glaucoma can lead to permanent vision loss.
The primary treatment is to discontinue hydrochlorothiazide as rapidly as possible. Prompt medical or surgical treatment may need to be considered if the intraocular pressure remains uncontrolled. Risk factors for developing acute angle closure glaucoma may include a history of sulfonamide or penicillin allergy.
Patients with heart failure/post-myocardial infarction: In patients whose renal function may depend on the activity of the renin-angiotensin-aldosterone system (e.g. patients with severe congestive heart failure), treatment with angiotensin converting enzyme inhibitors or angiotensin receptor antagonists has been associated with oliguria and/or progressive azotemia, and in rare cases with acute renal failure and/or death. Evaluation of patients with heart failure or post-myocardial infarction should always include assessment of renal function.
Dual Blockade of the Renin-Angiotensin System (RAS): Caution is required while co-administering ARBs, including valsartan, with other agents blocking the RAS such as ACEIs or aliskiren (see Dual blockade of the RAS under INTERACTIONS).
Non-melanoma skin cancer: An increased risk of non-melanoma skin cancer (NMSC) [basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)] with increasing cumulative dose of hydrochlorothiazide exposure has been observed in two epidemiological studies based on Danish National cancer registry. The risk for NMSC appears to increase with long-term use (see PHARMACOLOGY under ACTIONS). Photosensitizing actions of hydrochlorothiazide could act as a possible mechanism for NMSC.
Patients taking hydrochlorothiazide should be informed of the risk of NMSC and advised to regularly check their skin for any new lesions and promptly report any suspicious skin lesions. Possible preventive measures such as limited exposure to sunlight and adequate protection when exposed to sunlight should be advised to the patients in order to minimize the risk of skin cancer. Suspicious skin lesions should be promptly examined, potentially including histological examination of biopsies. The use of hydrochlorothiazide may also need to be reconsidered in patients who have previously experienced NMSC (see ADVERSE REACTIONS).
Pregnancy: Risk summary: As for any drug that also acts directly on the RAAS, valsartan + hydrochlorothiazide (Co-Diovan) must not be used during pregnancy (see CONTRAINDICATIONS).
Due to the mechanism of action of angiotensin II antagonists, a risk for the fetus cannot be excluded. In utero exposure to angiotensin converting enzyme (ACE) inhibitors (a specific class of drugs acting on the renin-angiotensin-aldosterone system-RAAS) given to pregnant women during the second and third trimesters has been reported to cause injury and death to the developing foetus. In addition, in retrospective data, first trimester use of ACE inhibitors has been associated with a potential risk of birth defects. There have been reports of spontaneous abortion, oligohydramnios and new born renal dysfunction, when pregnant women have inadvertently taken valsartan.
Intrauterine exposure to thiazide diuretics, including hydrochlorothiazide, is associated with fetal or neonatal jaundice or thrombocytopenia, and may be associated with other adverse reactions that have occurred in adults.
If pregnancy is detected during therapy, treatment should be discontinued as soon as possible (see PHARMACOLOGY: TOXICOLOGY: NON-CLINICAL SAFETY DATA under ACTIONS).
Clinical considerations: Disease-associated maternal and/or embryo/fetal risk: Hypertension in pregnancy increases the maternal risk for pre-eclampsia, gestational diabetes, premature delivery, and delivery complications (e.g., need for cesarean section, and post-partum hemorrhage). Hypertension increases the fetal risk for intrauterine growth restriction and intrauterine death.
Fetal/Neonatal Risk: Oligohydramnios in pregnant women who use drugs affecting the renin-angiotensin system in the second and third trimesters of pregnancy can result in the following: reduced fetal renal function leading to anuria and renal failure, fetal lung hypoplasia, skeletal deformations, including skull hypoplasia, hypotension and death.
In case of accidental exposure to ARB therapy, appropriate fetal monitoring should be considered.
Infants whose mothers have taken ARB therapy should be closely observed for hypotension.
Animal data: Valsartan: In embryofetal development studies in mice, rats and rabbits, fetotoxicity was observed in association with maternal toxicity in rats at valsartan doses of 600 mg/kg/day approximately 18 times the maximum recommended human dose on a mg/m2 basis (calculations assume an oral dose of 320 mg/day and a 60-kg patient) and in rabbits at doses of 10 mg/kg/day approximately 0.6 times the maximum recommended human dose on a mg/m2 basis (calculations assume an oral dose of 320 mg/day and a 60-kg patient). There was no evidence of maternal toxicity or fetotoxicity in mice up to a dose level of 600 mg/kg/day approximately 9 times the maximum recommended human dose on a mg/m2 basis (calculations assume an oral dose of 320 mg/day and a 60-kg patient).
Hydrochlorothiazide: Hydrochlorothiazide was not teratogenic and had no effects on fertility and conception. No teratogenic potential was revealed in 3 animal species tested. There was no dose-related fetotoxicity at oral dose levels of 0, 100, 300 and 1000 mg/kg in rats. A decrease in weight gain in suckling rat pups was attributed to the high dose and diuretic effects of hydrochlorothiazide, with subsequent effects on milk production.
Lactation: Risk summary: It is not known whether valsartan is transferred into human milk. Valsartan was transferred into the milk of lactating rats. Hydrochlorothiazide crosses the placenta and is transferred into human milk. Thus, use is not advisable in breast-feeding mothers.
Females and males of reproductive potential: As for any drug that acts directly on the RAAS, Co-Diovan should not be used in women planning to become pregnant. Healthcare professionals prescribing any agents acting on the RAAS should counsel women of childbearing potential about the potential risk of these agents during pregnancy.
Infertility: There is no information on the effects of valsartan or hydrochlorothiazide on human fertility. Studies in rats did not show any effects of valsartan or hydrochlorothiazide on fertility (see PHARMACOLOGY: TOXICOLOGY: NON-CLINICAL SAFETY DATA under ACTIONS).
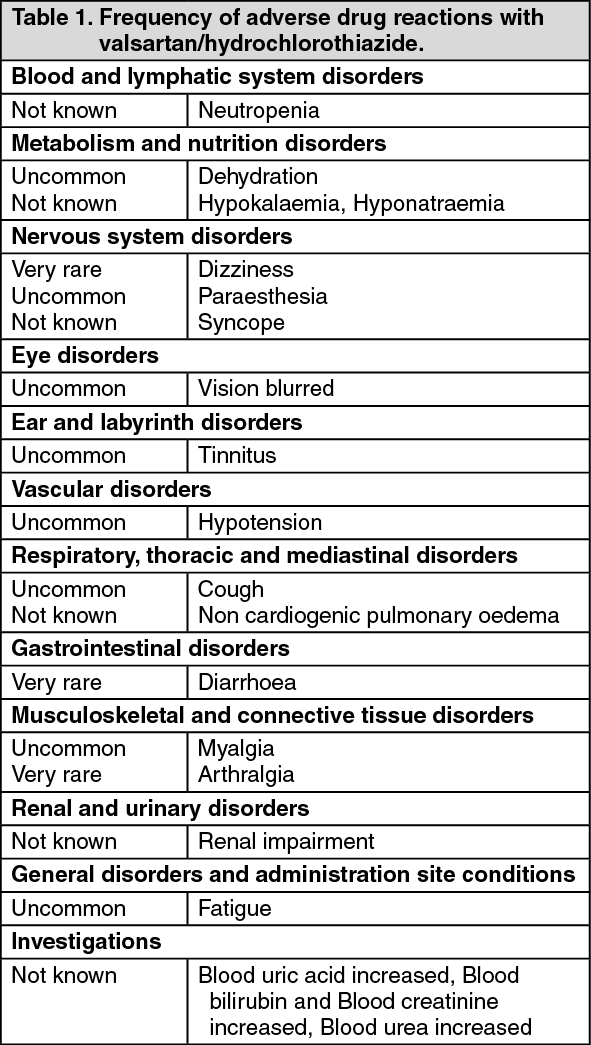
Adverse drug reactions reported in clinical trials and laboratory findings occurring more frequently with valsartan plus hydrochlorothiazide versus placebo and individual post-marketing reports are presented as follows according to system organ class. Adverse reactions known to occur with each component given individually but which have not been seen in clinical trials may occur during treatment with valsartan/hydrochlorothiazide.
Adverse drug reactions are ranked by frequency, the most frequent first, using the following convention: very common (> 1/10); common (> 1/100 to < 1/10); uncommon (> 1/1,000 to < 1/100); rare (> 1/10,000 to < 1/1,000); very rare (< 1/10,000), not known (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are ranked in order of decreasing seriousness. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The following events have also been observed during clinical trials in hypertensive patients irrespective of their causal association with the study drug: Abdominal pain, abdominal pain upper, anxiety, arthritis, asthenia, back pain, bronchitis, bronchitis acute, chest pain, dizziness postural, dyspepsia, dyspnea, dry mouth, epistaxis, erectile dysfunction, gastroenteritis, headache, hyperhydrosis, hypoesthesia, influenza, insomnia, ligament sprain, muscle spasms, muscle strain, nasal congestion, nasopharyngitis, nausea, neck pain, oedema, oedema peripheral, otitis media, pain in extremity, palpitations, pharyngolaryngeal pain, pollakiuria, pyrexia, sinusitis, sinus congestion, somnolence, tachycardia, upper respiratory tract infections, urinary tract infections, vertigo, viral infections, vision disturbance.
Additional information on the individual components: Adverse reactions previously reported with one of the individual components may be potential undesirable effects with valsartan + hydrochlorothiazide (Co-Diovan) as well, even if not observed in clinical trials or during post-marketing period.
Valsartan: (See Table 2.)
Click on icon to see table/diagram/image
The following events have also been observed during clinical trials in hypertensive patients irrespective of their causal association with the study drug: Arthralgia, asthenia, back pain, diarrhoea, dizziness, headache, insomnia, libido decrease, nausea, oedema, pharyngitis, rhinitis, sinusitis, upper respiratory tract infection, viral infections.
Hydrochlorothiazide: (See Table 3.)
Click on icon to see table/diagram/image
Valsartan-hydrochlorothiazide: The following drug interactions may occur due to both components (valsartan and/or hydrochlorothiazide): Lithium: Reversible increases in serum lithium concentrations and toxicity have been reported during concomitant administration of lithium with ACE inhibitors, angiotensin II receptor antagonists or thiazides. Since renal clearance of lithium is reduced by thiazides, the risk of lithium toxicity may presumably be increased further with Valsartan + Hydrochlorothiazide (Co-Diovan). Therefore, careful monitoring of serum lithium concentrations is recommended during concomitant use.
Valsartan: The following potential drug interactions may occur due to the valsartan component: Dual blockade of the Renin-Angiotensin-System (RAS) with ARBs, ACEIs, or aliskiren: The concomitant use of ARBs, including valsartan, with other agents acting on the RAS is associated with an increased incidence of hypotension, hyperkalemia, and changes in renal function compared to monotherapy. It is recommended to monitor blood pressure, renal function and electrolytes in patients on valsartan + hydrochlorothiazide (Co-Diovan) and other agents that affect the RAS (see PRECAUTIONS).
The concomitant use of ARBs-including valsartan- or of ACEIs with aliskiren, should be avoided in patients with severe renal impairment (GFR < 30 mL/min) (see PRECAUTIONS).
The concomitant use of ARBs-including valsartan- or of ACEIs with aliskiren is contraindicated in patients with Type 2 diabetes (see CONTRAINDICATIONS).
Potassium: Concomitant use with potassium supplements, potassium-sparing diuretics, salt substitutes containing potassium, or other drugs that may alter potassium levels (heparin, etc.) should be used with caution and with frequent monitoring of potassium.
Non-Steroidal Anti-Inflammatory Agents (NSAIDs) including Selective Cyclooxygenase-2 Inhibitors (COX-2 Inhibitors): When angiotensin II antagonists are administered simultaneously with NSAIDs, attenuation of the antihypertensive effect may occur. Furthermore, in patients who are elderly, volume-depleted (including those on diuretic therapy), or have compromised renal function, concomitant use of angiotensin II antagonists and NSAIDs may lead to an increased risk of worsening of renal function. Therefore, monitoring of renal function is recommended when initiating or modifying the treatment in patients on valsartan who are taking NSAIDs concomitantly.
Transporters: The results from an in vitro study with human liver tissue indicate that valsartan is a substrate of the hepatic uptake transporter OATP1B1 and the hepatic efflux transporter MRP2. Co-administration of inhibitors of the uptake transporter (rifampin, ciclosporin) or efflux transporter (ritonavir) may increase the systemic exposure to valsartan.
In monotherapy with valsartan, no drug interactions of clinical significance have been found with the following drugs: cimetidine, warfarin, furosemide, digoxin, atenolol, indomethacin, hydrochlorothiazide, amlodipine, glibenclamide.
Hydrochlorothiazide: The following potential drug interactions may occur due to the thiazide component: Other anti-hypertensive drugs: Thiazides potentiate the antihypertensive action of other antihypertensive drugs (e.g. guanethidine, methyldopa, beta-blockers, vasodilators, calcium channel blockers, ACE inhibitors, Angiotensin Receptor Blockers (ARBs) and Direct Renin Inhibitors (DRIs)).
Skeletal muscle relaxants: Thiazides, including hydrochlorothiazide, potentiate the action of skeletal muscle relaxants such as curare derivatives.
Medicinal products affecting serum potassium levels: The hypokalemic effect of diuretics may be increased by concomitant administration of kaliuretic diuretics, corticosteroids, ACTH, amphotericin, carbenoxolone, penicillin G, salicylic acid derivatives or antiarrhythmics (see PRECAUTIONS).
Medicinal products affecting serum sodium levels: The hyponatremic effect of diuretics may be intensified by concomitant administration of drugs such as antidepressants, antipsychotics, antiepileptics, etc. Caution is advised in long-term administration of these drugs (see PRECAUTIONS).
Antidiabetic agents: Thiazides may alter glucose tolerance. It may be necessary to adjust the dosage of insulin and of oral antidiabetic agents.
Digitalis glycosides: Thiazide-induced hypokalemia or hypomagnesemia may occur as unwanted effects, favoring the onset of digitalis-induced cardiac arrhythmias (see PRECAUTIONS).
NSAIDs and Cox-2 selective inhibitors: Concomitant administration of NSAIDs (e.g. salicylic acid derivative, indomethacin) may weaken the diuretic and antihypertensive activity of the thiazide component. Concurrent hypovolemia may induce acute renal failure.
Allopurinol: Co-administration of thiazide diuretics (including hydrochlorothiazide) may increase the incidence of hypersensitivity reactions to allopurinol.
Amantadine: Co-administration of thiazide diuretics (including hydrochlorothiazide) may increase the risk of adverse effects caused by amantadine.
Antineoplastic agents (e.g. cyclophosphamide, methotrexate): Concomitant use of thiazide diuretics may reduce renal excretion of cytotoxic agents and enhance their myelosuppressive effects.
Anticholinergic agents: The bioavailability of thiazide-type diuretics may be increased by anticholinergic agents (e.g. atropine, biperiden), apparently due to a decrease in gastrointestinal motility and the stomach emptying rate. Conversely prokinetic drugs such as cisapride may decrease the bioavailability of thiazide-type diuretics.
Ion exchange resins: Absorption of thiazide diuretics, including hydrochlorothiazide, is decreased by cholestyramine or colestipol. However, staggering the dosage of hydrochlorothiazide and resin such that hydrochlorothiazide is administered at least 4 h before or 4-6 h after the administration of resins would potentially minimize the interaction.
Vitamin D: Administration of thiazide diuretics, including hydrochlorothiazide, with vitamin D or with calcium salts may potentiate the rise in serum calcium.
Ciclosporin: Concomitant treatment with ciclosporin may increase the risk of hyperuricemia and gout-type complications.
Calcium salts: Concomitant use of thiazide type diuretics may lead to hypercalcemia by increasing tubular calcium reabsorption.
Diazoxide: Thiazide diuretics may enhance the hyperglycemic effect of diazoxide.
Methyldopa: There have been reports in the literature of hemolytic anemia occurring with concomitant use of hydrochlorothiazide and methyldopa.
Alcohol, barbiturates or narcotics: Concomitant administration of thiazide diuretics with alcohol, barbiturates, or narcotics may potentiate orthostatic hypotension.
Pressor amines: Hydrochlorothiazide may reduce the response to pressor amines such as noradrenaline. The clinical significance of this effect is uncertain and not sufficient to preclude their use.
INCOMPATIBILITIES: Not applicable.
Store at temperatures not exceeding 30°C.
C09DA03 - valsartan and diuretics ; Belongs to the class of angiotensin II receptor blockers (ARBs) in combination with diuretics. Used in the treatment of cardiovascular disease.
Co-Diovan 160/12.5 mg tab
14's;28's
Co-Diovan 160/25 mg tab
28's
Co-Diovan 320/12.5 mg tab
7's
Co-Diovan 320/25 mg tab
7's
Co-Diovan 80/12.5 mg tab
28's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image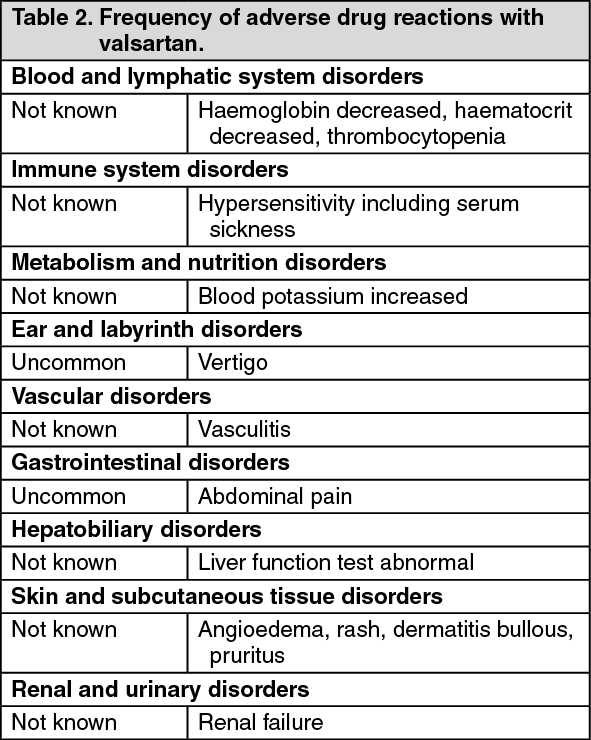 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image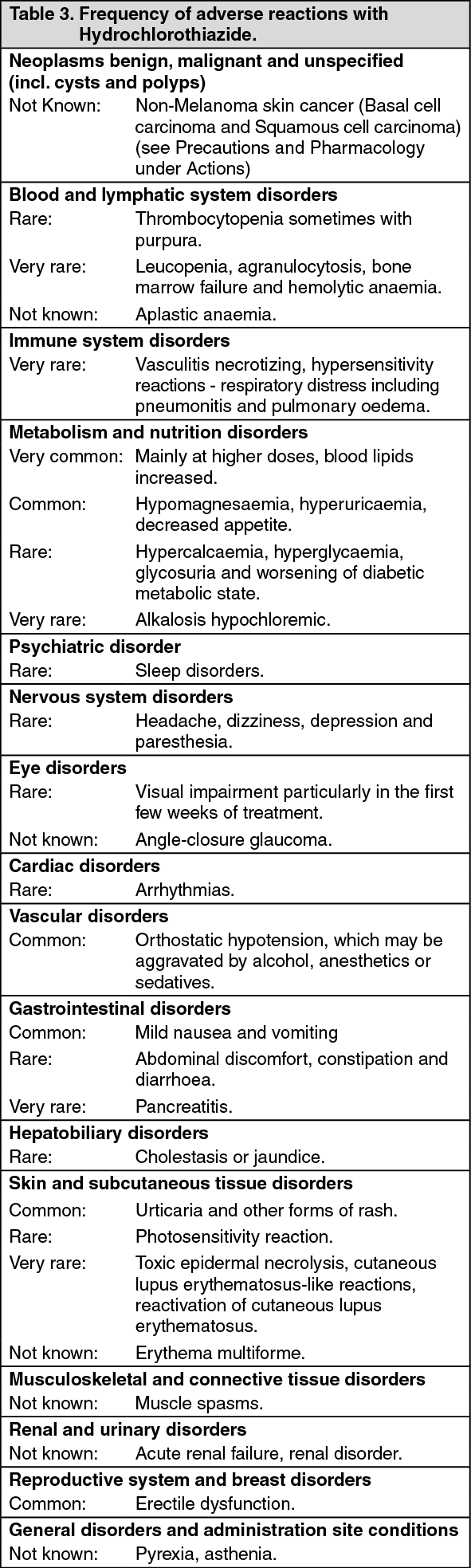 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image





 Sign Out
Sign Out