The dose to be administered and the treatment duration should take into account the severity of the infection as well as the clinical response. Therapeutic guidelines should be adhered too. The dose is expressed in international units (IU) of colistimethate sodium (CMS). A conversion table from CMS in IU to mg of CMS as well as to mg of colistin base activity (CBA) is included at the end of this section.
Posology: The following dose recommendations are made based on limited population-pharmacokinetic data in critically ill patients.
Adults and adolescents: Maintenance dose 9 MIU/day in 2-3 divided doses in patients who are critically ill, a loading dose of 9 MIU should be administered. The most appropriate time interval to the first maintenance dose has not been established. Modelling suggests that loading and maintenance doses of up to 12 MIU may be required in patients with good renal function in some cases. Clinical experience with such doses is however extremely limited and safety has not been established. The loading dose applies to patients with normal and impaired renal functions including those on renal replacement therapy.
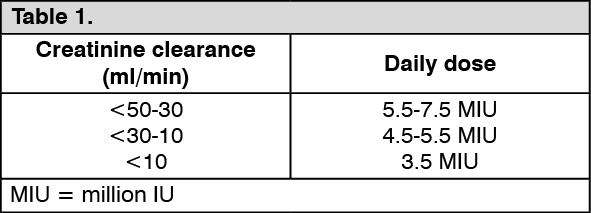
Renal impairment: Dose adjustments in renal impairment are necessary, but pharmacokinetic data available for patients with impaired renal function is very limited. The following dose adjustments are suggested as guidance.
Dose reductions are recommended for patients with creatinine clearance <50 mL/min: Twice daily dosing is recommended. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Haemodialysis and continuous haemo(dia) filtration Colistin appears to be dialyzable through conventional haemodialysis and continuous venovenous haemo(dia)filtration (CVVHF, CVVHDF). There are extremely limited data from population PK studies from very small numbers of patients on renal replacement therapy. Firm dose recommendations cannot be made. The following regimes could be considered.
Haemodialysis: No-HD days: 2.25 MIU/day (2.2-2.3 MIU/day). HD days: 3 MIU/day on haemodialysis days, to be given after the HD session. Twice daily dosing is recommended.
CVVHF/CVVHDF: As in patients with normal renal function. Three times daily dosing is recommended.
Hepatic impairment: There are no data in patients with hepatic impairment. Caution is advised when administering colistimethate sodium in these patients.
Older people: No dose adjustments in older patients with normal renal function are considered necessary.
Paediatric population: The data supporting the dose regimen in paediatric patients are very limited. Renal maturity should be taken into consideration when selecting the dose. The dose should be based on lean body weight. Children ≤40 kg 75,000-150,000 IU/kg/day divided into 3 doses. For children with a body weight above 40 kg, use of the dosing recommendation for adults should be considered. The use of doses >150,000 IU/kg/day has been reported in children with cystic fibrosis. There are no data regarding the use or magnitude of a loading dose in critically ill children. No dose recommendations have been established in children with impaired renal function.
Intrathecal and intraventricular administration: Based on limited data, the following dose is recommended in adults.
Intraventricular route: 125,000 IU/day Intrathecally administered doses should not exceed those recommended for intraventricular use.
No specific dosing recommendation can be made in children for intrathecal and intraventricular routes of administration.
Method of Administration: Colistimethate Sodium is administered intravenously as a slow infusion over 30-60 minutes. Colistimethate sodium undergoes hydrolysis to the active substance colistin in aqueous solution. For dose preparation, particularly where combination of multiple vials is needed, reconstitution of the required dose must be performed using strict aseptic technique.
Reconstitution: The 160 mg (equivalent to 2,000,000 IU) vial should be reconstituted with 25 mL Sterile Water for Injection, USP. The reconstituted solution provides colistimethate sodium at a concentration equivalent to 6.4 mg/mL (80,000 IU/mL) colistin base activity.
During reconstitution, swirl gently to avoid frothing.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. If these conditions are observed, the product should not be used.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out