


 Sign Out
Sign Out

The safety data described as follows reflect exposure to Daratumumab (Darzalex) (16 mg/kg) in 2459 patients with multiple myeloma including 2303 patients who received Daratumumab (Darzalex) in combination with background regimens and 156 patients who received Daratumumab (Darzalex) as monotherapy.
Newly Diagnosed Multiple Myeloma: Combination treatment with lenalidomide and dexamethasone (DRd): Adverse reactions described in the table as follows reflect exposure to Daratumumab (Darzalex) for a median treatment duration of 25.3 months (range: 0.1 to 40.44 months) for the daratumumab-lenalidomide-dexamethasone (DRd) group and median treatment duration of 21.3 months (range: 0.03 to 40.64 months) for the lenalidomide-dexamethasone group (Rd) in a Phase 3 active-controlled study (Study MMY3008). The most frequent (≥20%) adverse reactions were infusion reactions, diarrhea, constipation, nausea, peripheral edema, fatigue, back pain, asthenia, pyrexia, upper respiratory tract infection, bronchitis, pneumonia, decreased appetite, muscle spasms, peripheral sensory neuropathy, dyspnea and cough. Serious adverse reactions with a 2% greater incidence in the DRd arm compared to the Rd arm were dehydration (DRd 2% vs Rd <1%), bronchitis (DRd 4% vs Rd 2%) and pneumonia (DRd 15% vs Rd 8%). (See Table 12.)
 Click on icon to see table/diagram/image
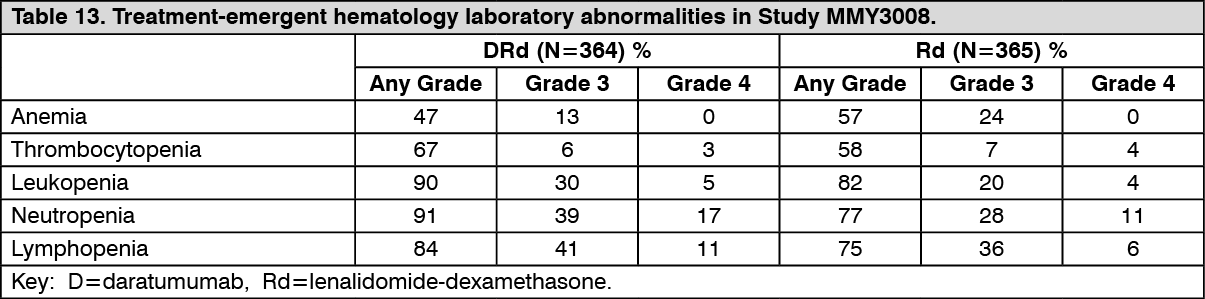
Click on icon to see table/diagram/imageLaboratory abnormalities worsening during treatment from baseline listed in the table as follows. (See Table 13.)
 Click on icon to see table/diagram/image
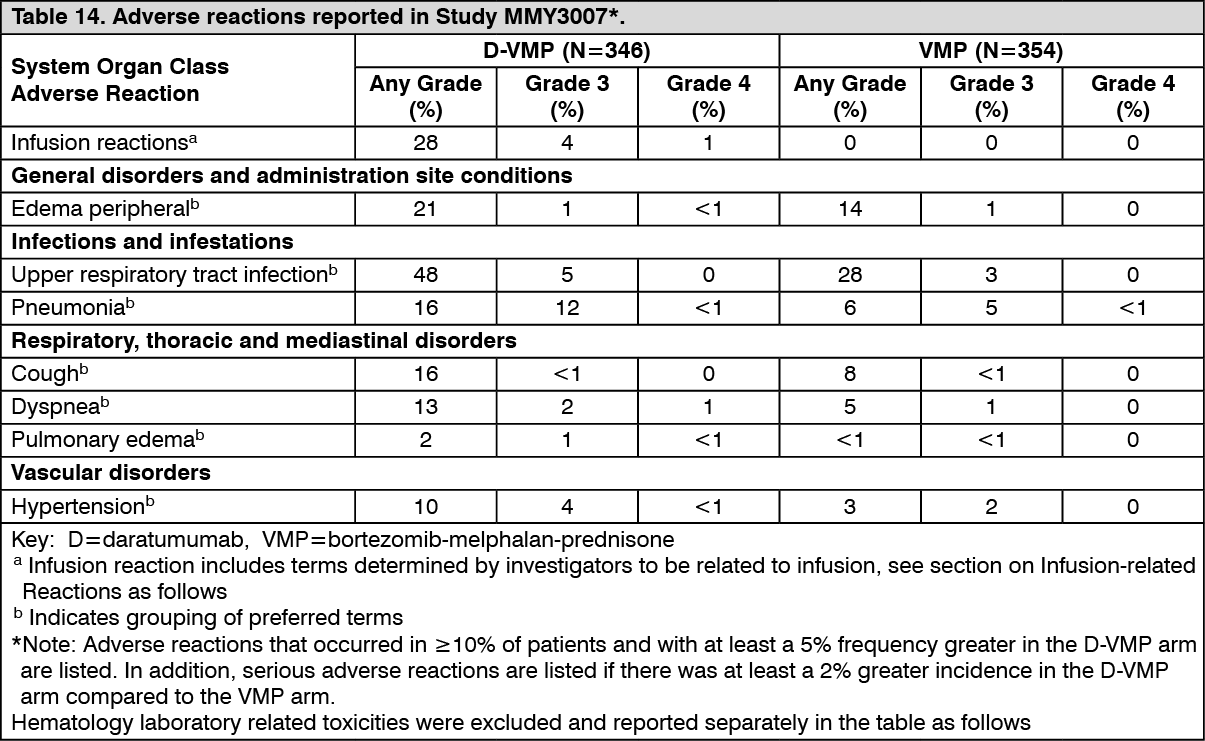
Click on icon to see table/diagram/imageCombination treatment with bortezomib, melphalan and prednisone: Adverse reactions described in the table as follows reflect exposure to Daratumumab (Darzalex) for a median treatment duration of 14.7 months (range: 0 to 25.8 months) for the daratumumab, bortezomib, melphalan and prednisone (D-VMP) group, and median treatment duration of 12 months (range: 0.1 to 14.9 months) for the VMP group in a Phase 3 active-controlled study (Study MMY3007). The most frequent adverse reactions (≥20%) were infusion reactions, upper respiratory tract infection and edema peripheral. Serious adverse reactions with at least a 2% greater incidence in the D-VMP arm compared to the VMP arm were pneumonia (D-VMP 11% vs VMP 4%), upper respiratory tract infection (D-VMP 5% vs VMP 1%), and pulmonary edema (D-VMP 2% vs VMP 0%). (See Table 14.)
 Click on icon to see table/diagram/image
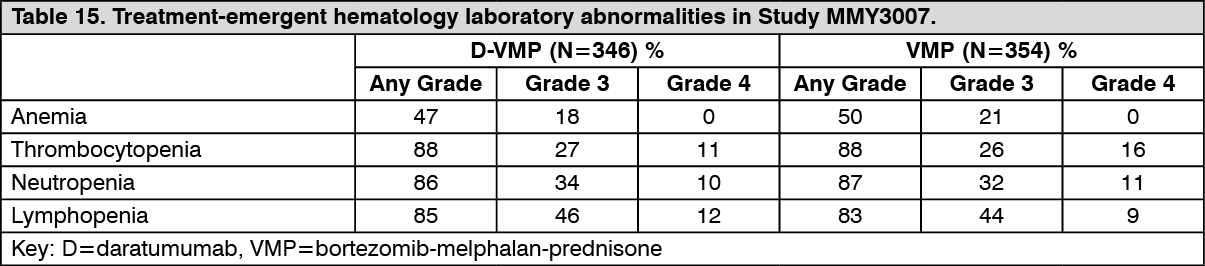
Click on icon to see table/diagram/imageLaboratory abnormalities worsening during treatment from baseline listed in the table as follows. (See Table 15.)
 Click on icon to see table/diagram/image
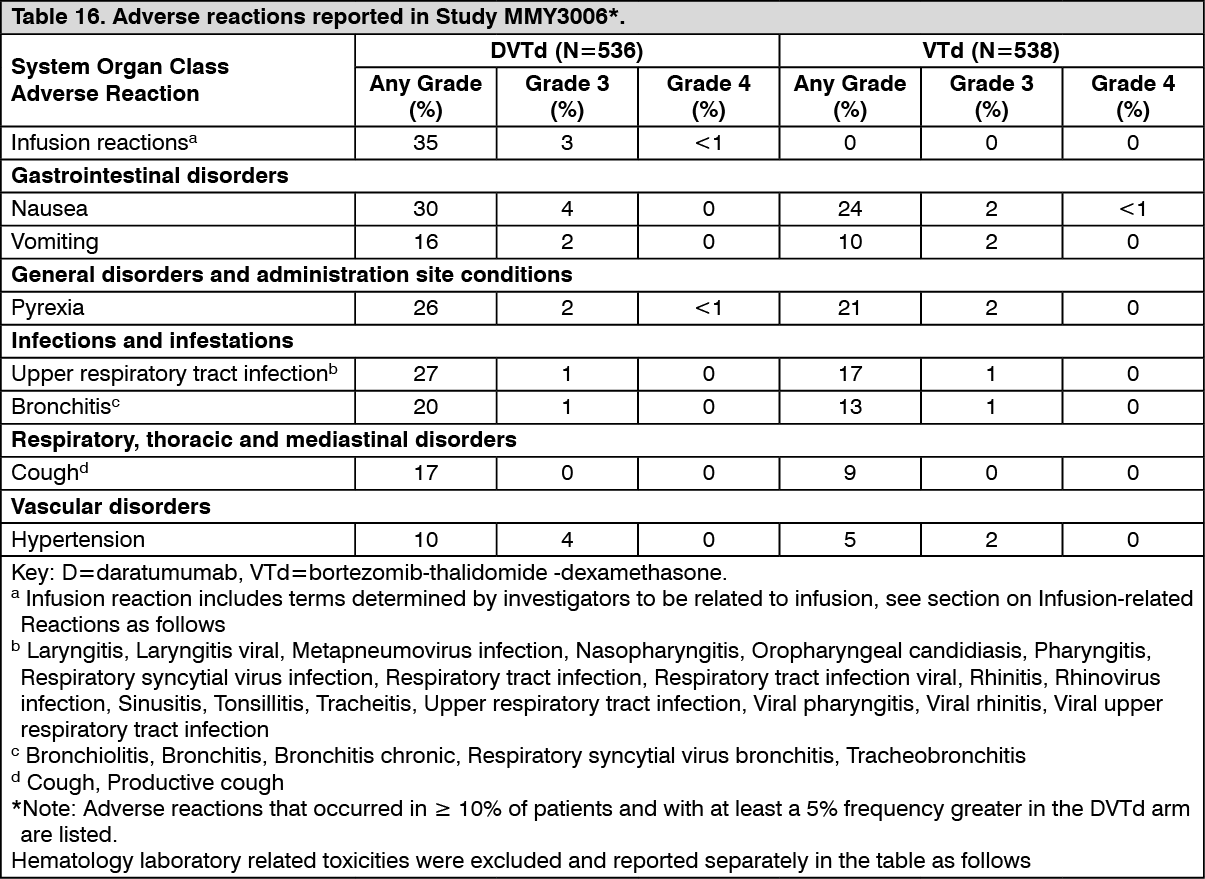
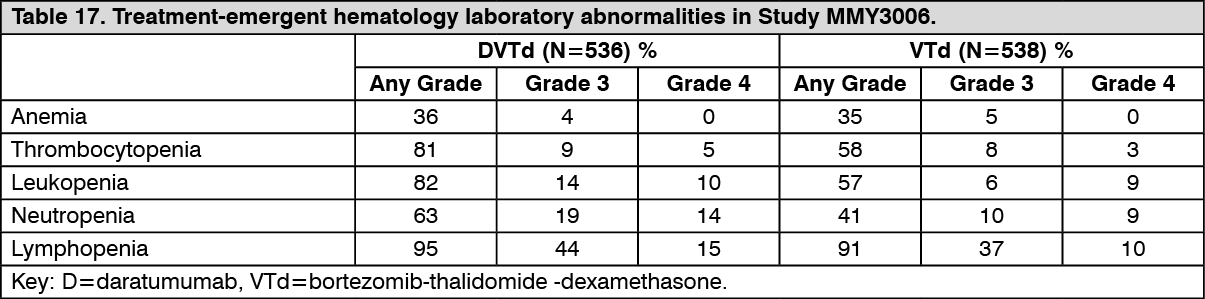
Click on icon to see table/diagram/imageCombination treatment with bortezomib, thalidomide and dexamethasone (DVTd): Adverse reactions described in the table as follows reflect exposure to Daratumumab (Darzalex) up to day 100 post-transplant in a Phase 3 active-controlled study, Study MMY3006 (see Clinical Studies). The median duration of induction/ASCT/consolidation treatment was 8.9 (range: 7.0 to 12.0) months for the DVTd group and 8.7 (range: 6.4 to 11.5) months for the VTd group. The most frequent adverse reactions (>20%) were infusion reactions, nausea, pyrexia, upper respiratory tract infection and bronchitis. Serious adverse reactions with a 2% greater incidence in the DVTd arm compared to the VTd arm were bronchitis (DVTd 2% vs VTd <1%) and pneumonia (DVTd 6% vs VTd 4%). (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLaboratory abnormalities worsening during treatment from baseline listed in the table as follows. (See Table 17.)
 Click on icon to see table/diagram/image
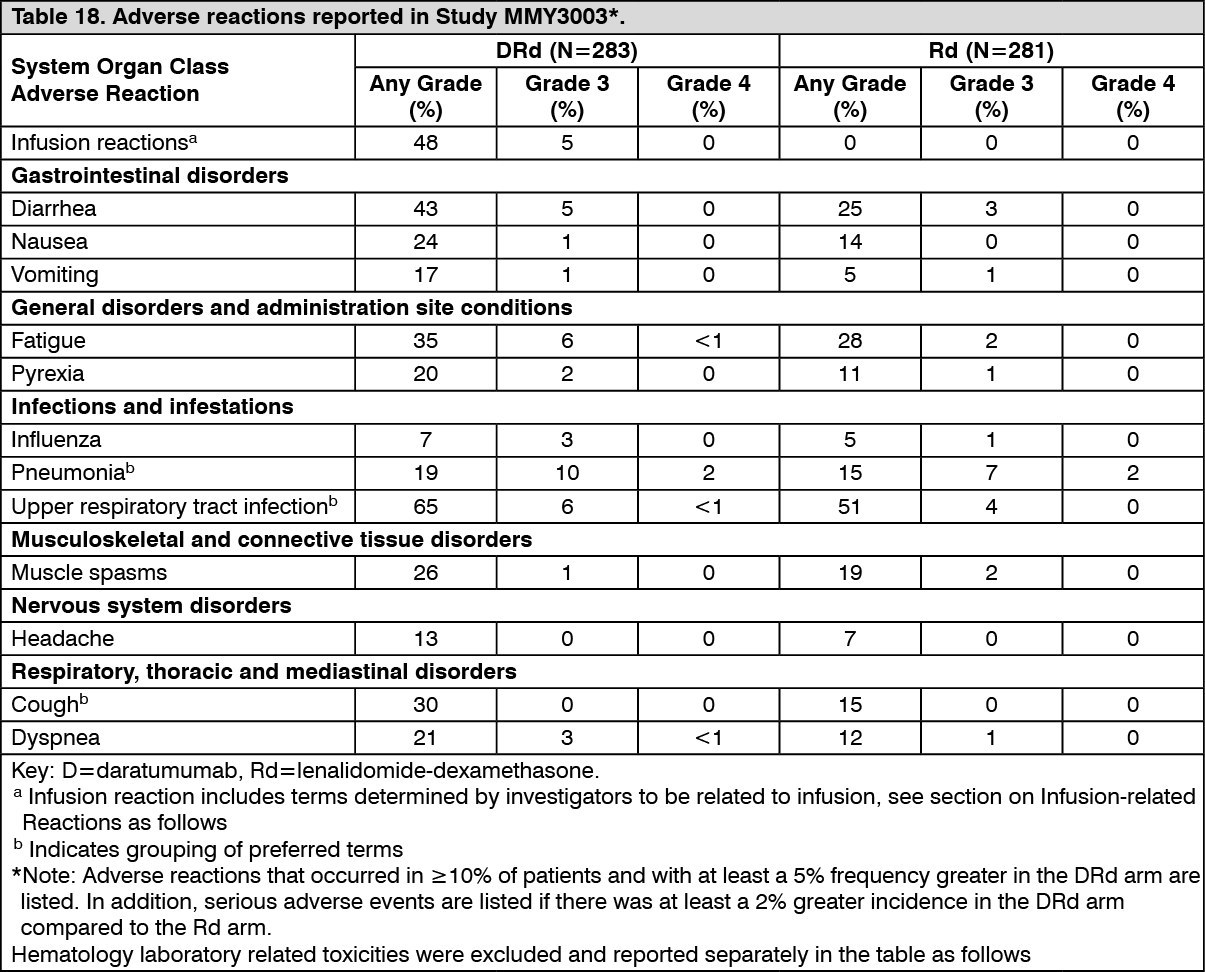
Click on icon to see table/diagram/imageRelapsed/Refractory Multiple Myeloma: Combination treatment with lenalidomide and dexamethasone: Adverse reactions described in the table as follows reflect exposure to Daratumumab (Darzalex) for a median treatment duration of 13.1 months (range: 0 to 20.7 months) for the daratumumab-lenalidomide-dexamethasone (DRd) group and median treatment duration of 12.3 months (range: 0.2 to 20.1 months) for the lenalidomide-dexamethasone group (Rd) in a Phase 3 active-controlled study (Study MMY3003). The most frequent adverse reactions were infusion reactions, diarrhea, nausea, fatigue, pyrexia, upper respiratory tract infection, muscle spasms, cough and dyspnea. Serious adverse reactions were pneumonia, upper respiratory tract infection, influenza and pyrexia. Adverse reactions result in discontinuations for 7% (n=19) of patients in the DRd arm versus 8% (n=22) in the Rd arm. (See Table 18.)
 Click on icon to see table/diagram/image
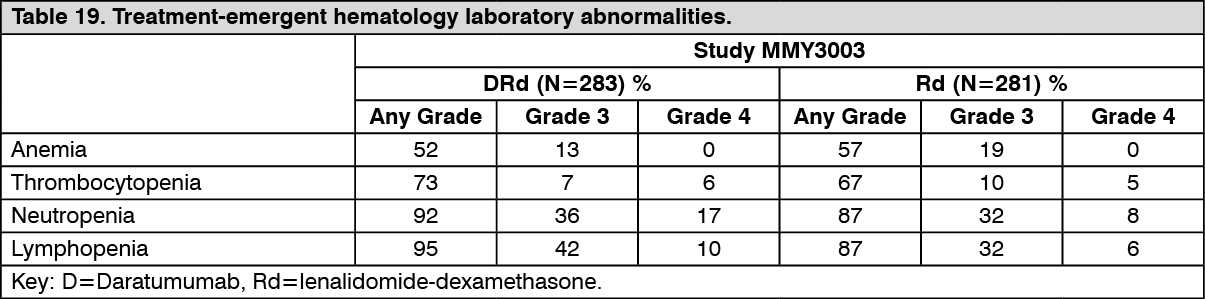
Click on icon to see table/diagram/imageLaboratory abnormalities worsening during treatment from baseline are listed in the table as follows. (See Table 19.)
 Click on icon to see table/diagram/image
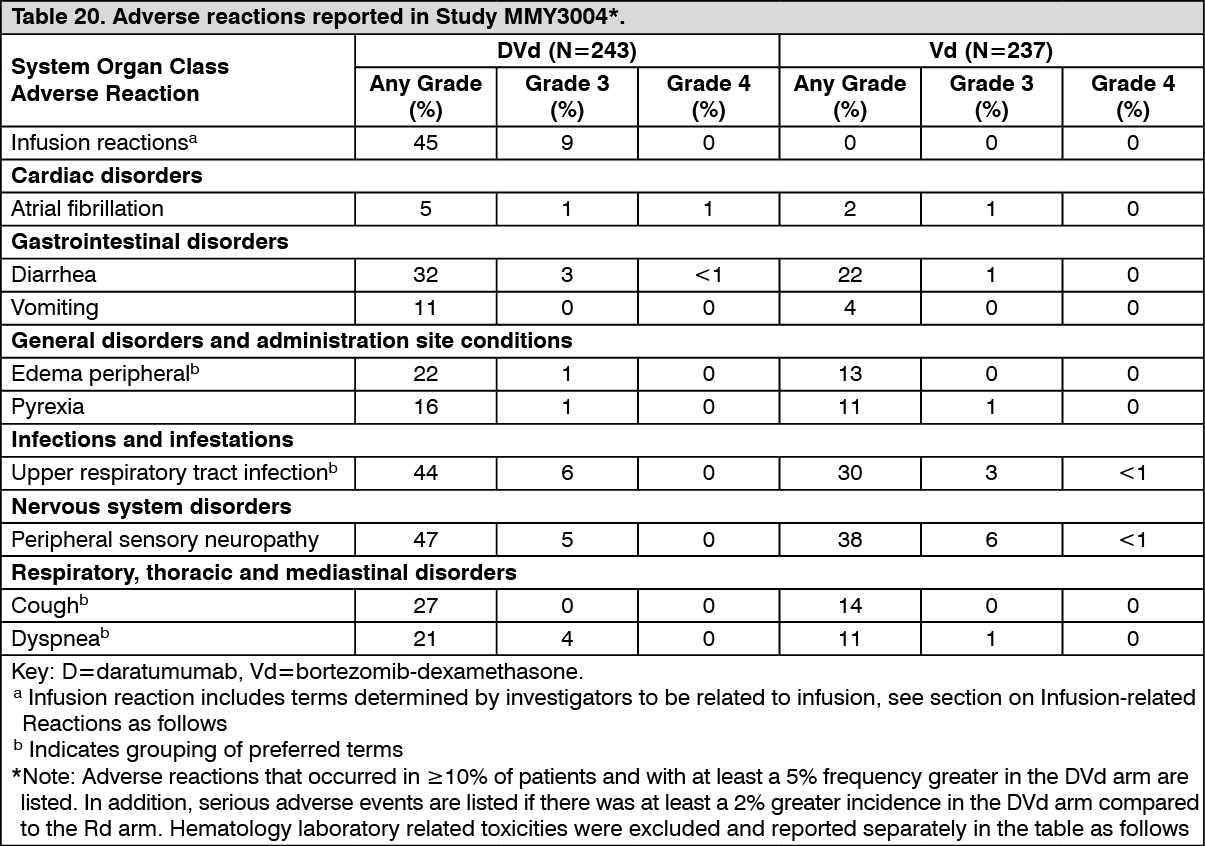
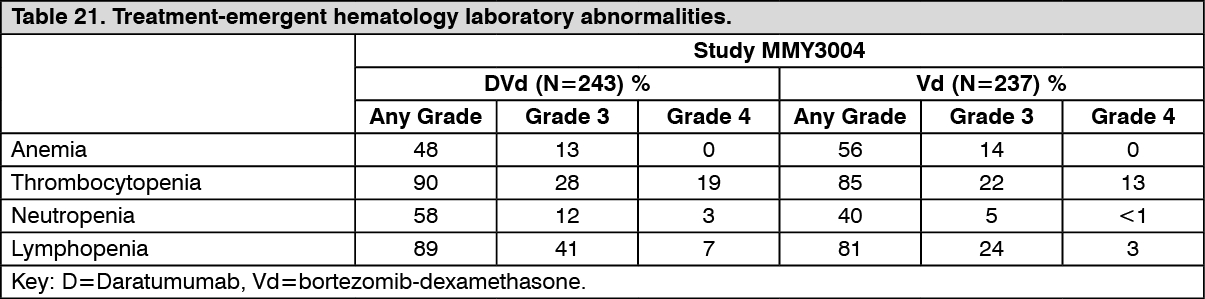
Click on icon to see table/diagram/imageCombination treatment with bortezomib and dexamethasone: Adverse reactions described in Table as follows reflect exposure to Daratumumab (Darzalex) for a median treatment duration of 6.5 months (range: 0 to 14.8 months) for the daratumumab-bortezomib-dexamethasone (DVd) group and median treatment duration of 5.2 months (range: 0.2 to 8.0 months) for bortezomib-dexamethasone group (Vd) in a Phase 3 active-controlled study (Study MMY3004). The most frequent adverse reactions (>20%) were infusion reactions, diarrhea, peripheral edema, upper respiratory tract infection, peripheral sensory neuropathy, cough and dyspnea. Serious adverse reactions included diarrhea, upper respiratory tract infection and atrial fibrillation. Adverse reactions resulted in discontinuations for 7% (n=18) of patients in the DVd arm versus 9% (n=22) in the Vd arm. (See Table 20.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLaboratory abnormalities worsening during treatment are listed in the table as follows. (See Table 21.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdverse Reactions identified from other clinical trials: Sepsis.
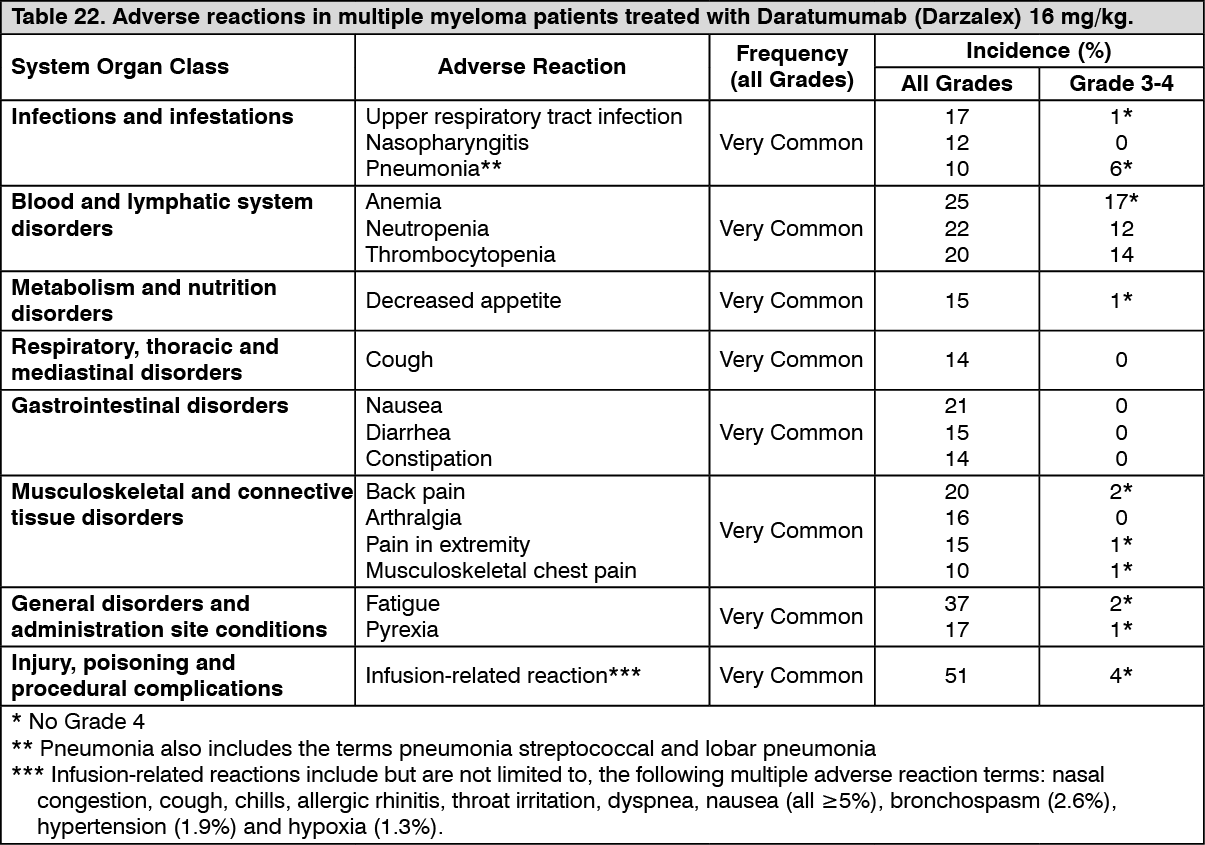
Monotherapy: The data described as follows reflect exposure to Daratumumab (Darzalex) in three pooled open-label clinical studies that included 156 patients with relapsed and refractory multiple myeloma treated with Daratumumab (Darzalex) at 16 mg/kg. The median duration of Daratumumab (Darzalex) treatment was 3.3 months, with the longest duration of treatment being 14.2 months. Adverse reactions occurring at a rate of ≥10% are presented in Table as follows. The most frequently reported adverse reactions (≥20%) were IRRs, fatigue, nausea, back pain, anemia, neutropenia and thrombocytopenia. Four percent of patients discontinued Daratumumab (Darzalex) treatment due to adverse reactions, none of which were considered drug related.
Frequencies are defined as very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10000 to <1/1000) and very rare (<1/10000). (See Table 22.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageInfusion-related reactions: In clinical trials (monotherapy and combination treatment; N=2066) the incidence of any grade infusion-related reactions was 37% with the first (16 mg/kg, Week 1) infusion of Daratumumab (Darzalex), 2% with the Week 2 infusion, and cumulatively 6% with subsequent infusions. Less than 1% of patients had a Grade 3/4 infusion reaction at Week 2 or subsequent infusions.
The median time to onset of a reaction was 1.5 hours (range: 0 to 72.8 hours). The incidence of infusion modifications due to reactions was 36%. Median durations of 16 mg/kg infusions for the 1st, 2nd and subsequent infusions were approximately 7, 4 and 3 hours respectively.
Severe infusion-related reactions included bronchospasms, dyspnea, laryngeal edema, pulmonary edema, hypoxia, and hypertension. Other adverse infusion-related reactions included nasal congestion, cough, chills, throat irritation, vomiting and nausea (see Precautions).
When Daratumumab (Darzalex) dosing was interrupted in the setting of ASCT (Study MMY3006) for a median of 3.75 (range: 2.4; 6.9) months, upon re-initiation of Daratumumab (Darzalex) the incidence of IRRs was 11% at first infusion following ASCT. Infusion rate/dilution volume used upon re-initiation was that used for the last Daratumumab (Darzalex) infusion prior to interruption due to ASCT. IRRs occurring at re-initiation of Daratumumab (Darzalex) following ASCT were consistent in terms of symptoms and severity (Grade 3/4:<1%) with those reported in previous studies at Week 2 or subsequent infusions.
Infections: In patients receiving Daratumumab (Darzalex) combination therapy, Grade 3 or 4 infections were reported as follows: Relapsed/refractory patient studies: DVd: 21%, Vd: 19%; DRd: 28%, Rd: 23%; DPd: 28%; DKda: 36%, Kda: 27%, DKdb: 21%.
a where carfilzomib 20/56 mg/m2 was administered twice-weekly.
b where carfilzomib 20/70 mg/m2 was administered once-weekly.
Newly diagnosed patient studies: D-VMP: 23%, VMP: 15%; DRd: 32%, Rd: 23%; DVTd: 22%, VTd: 20%.
Pneumonia was the most commonly reported severe (Grade 3 or 4) infection across studies.
In the active controlled studies, discontinuations from treatment due to infections occurred in 1-4% of patients. Fatal infections were primarily due to pneumonia and sepsis.
In patients receiving Daratumumab (Darzalex) combination therapy, fatal infections (Grade 5) were reported as follows: Relapsed/refractory patient studies: DVd: 1%, Vd: 2%; DRd: 2%, Rd: 1%; DPd: 2%; DKda: 5%, Kda: 3%; DKdb: 0%.
a where carfilzomib 20/56 mg/m2 was administered twice-weekly.
b where carfilzomib 20/70 mg/m2 was administered once-weekly.
Newly diagnosed patient studies: D-VMP: 1%, VMP: 1%; DRd: 2%, Rd: 2%; DVTd: 0%, VTd: 0%.
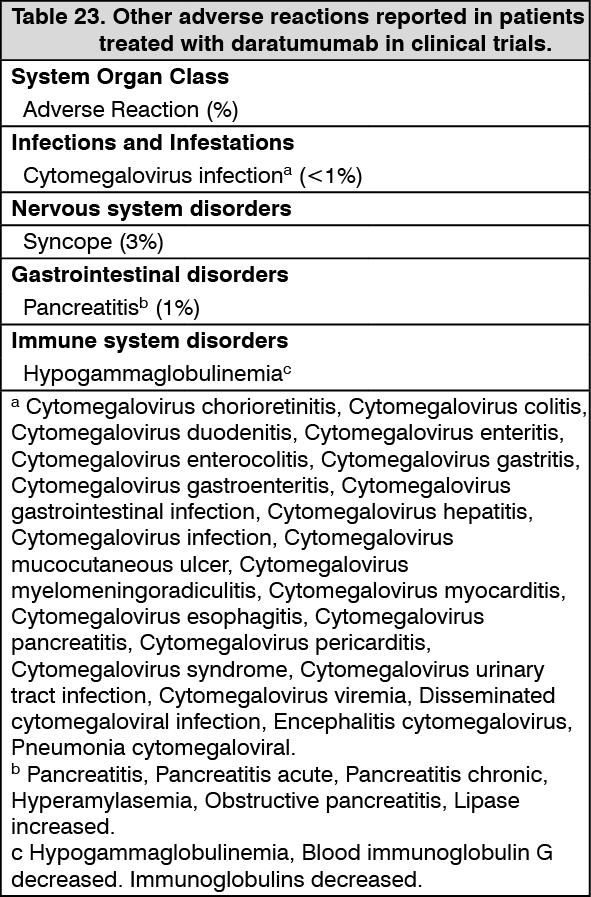
Other Adverse Reactions: Other adverse reactions reported in patients treated with daratumumab in clinical trials are listed in Table 23. (See Table 23.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOther special population: Of the 2459 patients who received Daratumumab (Darzalex) at the recommended dose, 38% were 65 to 75 years of age, and 15% were 75 years of age or older. No overall differences in effectiveness were observed based on age. The incidence of serious adverse reactions was higher in older than in younger patients (see Adverse Reactions and Pharmacology: Pharmacodynamics: Clinical Studies under Actions). Among patients with relapsed and refractory multiple myeloma (n=1213), the most common serious adverse reactions that occurred more frequently in elderly (≥65 years of age) were pneumonia and sepsis. Among patients with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplant (n=710), the most common serious adverse reaction that occurred more frequently in elderly (≥75 years of age) was pneumonia.
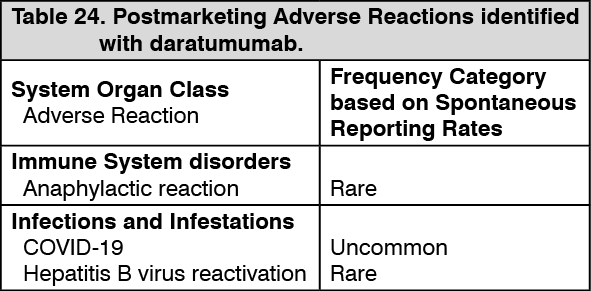
Postmarketing data: Adverse reactions identified during postmarketing experience with Daratumumab are included in Table 24. The frequencies are provided according to the following convention: Very common ≥1/10; Common ≥1/100 to <1/10; Uncommon ≥1/1,000 to <1/100; Rare ≥1/10,000 to <1/1,000; Very rare <1/10,000, including isolated reports, Not known (frequency cannot be estimated from the available data).
In Table 24, adverse reactions are presented by frequency category based on spontaneous reporting rates. (See Table 24.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form