Pharmacotherapeutic group: Antiemetic, antihistamines for systemic use.
ATC Code: R06AA59.
Pharmacology: Pharmacodynamics: Mechanism of action: This medicinal product provides the action of two unrelated compounds. Doxylamine hydrogen succinate (an antihistamine) and pyridoxine hydrochloride (vitamin B6) provide anti-nauseant and antiemetic activity.
Doxylamine hydrogen succinate is an ethanolamine derivative, a first generation antihistamine that is competitively, reversibly and non-specifically blocking H1 receptors. It is also a non-specific antagonist that blocks other receptors, such as central or peripheral muscarinic receptors. The antiemetic effect of doxylamine is also associated with the blocking of the central cholinergic and H1 receptors, although the mechanism of action is unknown.
Pyridoxine hydrochloride, a water-soluble vitamin, is converted to pyridoxal, pyridoxamine, pyridoxal 5'-phosphate and pyridoxamine 5'-phosphate. Although pyridoxal 5'-phosphate is the main active antiemetic metabolite, the other metabolites also contribute to the biological activity.
The mechanism of action of the combination of doxylamine hydrogen succinate and pyridoxine hydrochloride to treat nausea and vomiting of pregnancy has not been established.
Clinical efficacy and safety: The safety and efficacy of this medicinal product were compared to placebo in a double-blind, randomised, multi-centre trial in 261 adult women 18 years of age or older. The mean gestational age at enrolment was 9.3 weeks, range 7 to 14 weeks gestation. Two tablets of this medicinal product were administered at bedtime on Day 1. If symptoms of nausea and vomiting persisted into the afternoon hours of Day 2, the woman was directed to her usual dose of two tablets at bedtime that night and, beginning on Day 3, to take one tablet in the morning and two tablets at bedtime. Based upon assessment of remaining symptoms at her clinic visit on Day 4 (± 1 day), the woman may have been directed to take an additional tablet mid-afternoon. A maximum of four tablets (one in the morning, one in the mid-afternoon and two at bedtime) were taken daily.
Over the treatment period, 19% of the medicine-treated patients remained on two tablets daily, 21% three tablets daily, and 60% received four tablets daily.
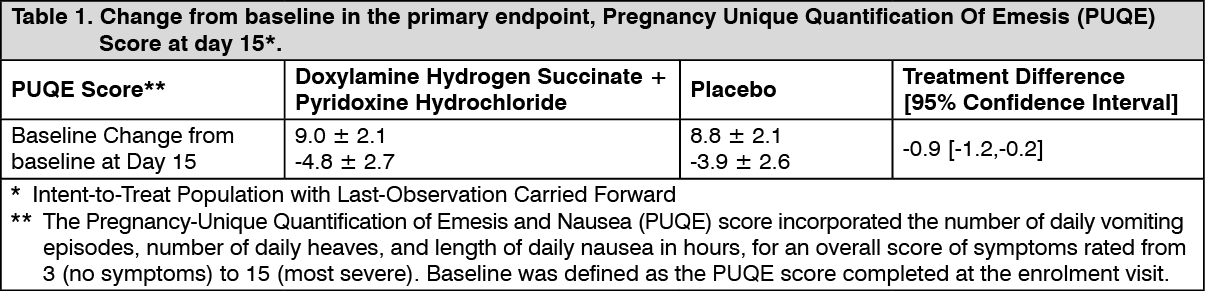
The primary efficacy endpoint was the change from baseline at Day 15 in the Pregnancy Unique-Quantification of Emesis (PUQE) score. The PUQE score incorporates the number of daily vomiting episodes, number of daily heaves, and length of daily nausea in hours, for an overall score of symptoms rated from 3 (no symptoms) to 15 (most severe).
At baseline, the mean PUQE score was 9.0 in the treatment arm and 8.8 in the placebo arm. There was a 0.9 (95% confidence interval 0.2 to 1.2 with p-value 0.006) mean decrease (improvement in nausea and vomiting symptoms) from baseline in PUQE score at Day 15 with this medicinal product compared to placebo (see Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the literature, the safety and effectiveness of Doxylamine succinate + Pyridoxine HCl (Diclegis) has been demonstrated in clinical trials, cohort studies and meta-analysis. The extensive postmarketing experience and numerous publications continue to support the positive benefit risk assessment of this medicinal product in the treatment of NVP in pregnant women.
Paediatric population: The European Medicines Agency has waived the obligation to submit the results of studies with this medicinal product in all subsets of the paediatric population in treatment of nausea and vomiting of pregnancy (see Dosage & Administration for information on paediatric use).
Pharmacokinetics: The pharmacokinetics of this medicinal product has been characterised in healthy non-pregnant adult women. Pharmacokinetic results for doxylamine and pyridoxine, including its vitamin B6 metabolites, pyridoxal, pyridoxal 5'-phosphate, pyridoxamine and pyridoxamine 5'-phosphate, are summarised in tables 2 to 5.
Absorption: A single-dose (two tablets) and multiple-dose (four tablets daily), open-label study was conducted to assess the safety and pharmacokinetic profile of this medicinal product administered in healthy non-pregnant adult women. Single-doses (two tablets at bedtime) were administered on Days 1 and 2. Multiple-doses (one tablet in the morning, one tablet in the afternoon and two tablets at bedtime) were administered on Days 3-18.
Blood samples for pharmacokinetic analysis were collected pre- and post-dose on Days 2 and 18 as well as pre-dose prior to bedtime dose only (trough) on Days 9, 10, 11, 16, 17 and 18.
Doxylamine and pyridoxine are absorbed in the gastrointestinal tract, mainly in the jejunum.
The Cmax of doxylamine and pyridoxine are achieved within 7.5 and 5.5 hours, respectively (see Table 2.)
Click on icon to see table/diagram/image
Multiple-dose administration resulted in increased concentrations of doxylamine as well as increases in doxylamine Cmax and AUC0-last of absorption. The time to reach the maximum concentration is not affected by multiple doses. The mean accumulation index is more than 1.0 suggesting that doxylamine accumulates following multiple dosing (see Table 3).
Although no accumulation was observed for pyridoxine, the mean accumulation index for each metabolite (pyridoxal, pyridoxal 5'-phosphate, pyridoxamine, and pyridoxamine 5'-phosphate) is more than 1.0 following multiple-dose administration. The time to reach the maximum concentration is not affected by multiple doses (see Table 2).
Click on icon to see table/diagram/image
The administration of food delays the absorption of both doxylamine and pyridoxine. This delay is associated with a lower peak concentration of doxylamine, but extent of absorption is not affected (see Table 4).
The effect of food on the peak concentration and the extent of absorption of the pyridoxine component is more complex because the pyridoxal, pyridoxamine, pyridoxal 5'-phosphate and pyridoxamine 5'-phosphate metabolites also contribute to the biological activity. Food significantly reduces the bioavailability of pyridoxine and pyridoxal lowering their Cmax and AUC by approximately 50% compared to fasting conditions. In contrast, food slightly increases pyridoxal 5'-phosphate Cmax and extent of absorption. As for pyridoxamine and pyridoxamine 5-phosphate, the rate and extent of absorption seem to decrease under fed conditions. (See Table 4.)
Click on icon to see table/diagram/image
Distribution: Pyridoxine is highly protein bound, primarily to albumin. Its main active metabolite pyridoxal 5'-phosphate (PLP) accounts for at least 60% of circulating vitamin B6 concentrations.
Biotransformation: Doxylamine is biotransformed in the liver by N-dealkylation to its principle metabolites N-desmethyl-doxylamine and N,N-didesmethyldoxylamine.
Pyridoxine is a prodrug primarily metabolised in the liver.
Elimination: The principle metabolites of doxylamine, N-desmethyl-doxylamine and N,N-didesmethyldoxylamine, are excreted by the kidney.
The terminal elimination half-life of doxylamine and pyridoxine are 12.6 hours and 0.4 hours, respectively (see Table 5.)
Click on icon to see table/diagram/image
Hepatic Impairment: No pharmacokinetic studies have been conducted in hepatic impaired patients.
Renal Impairment: No pharmacokinetic studies have been conducted in renal impaired patients.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on available data of repeated dose toxicity, genotoxicity and carcinogenic potential.
Reproductive toxicity: In a reproductive toxicity study of a drug product containing equal concentrations of doxylamine hydrogen succinate and pyridoxine hydrochloride in rats, maternal toxicity was observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use. Developmental toxicity (including reduced prenatal viability and reduced foetal body weight per litter, reduced foetal ossification in anterior distal limbs) only occurred in the presence of maternal toxicity (at doses from 60 times the maximum human recommended based on mg/m2). No teratogenic effects are reported.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image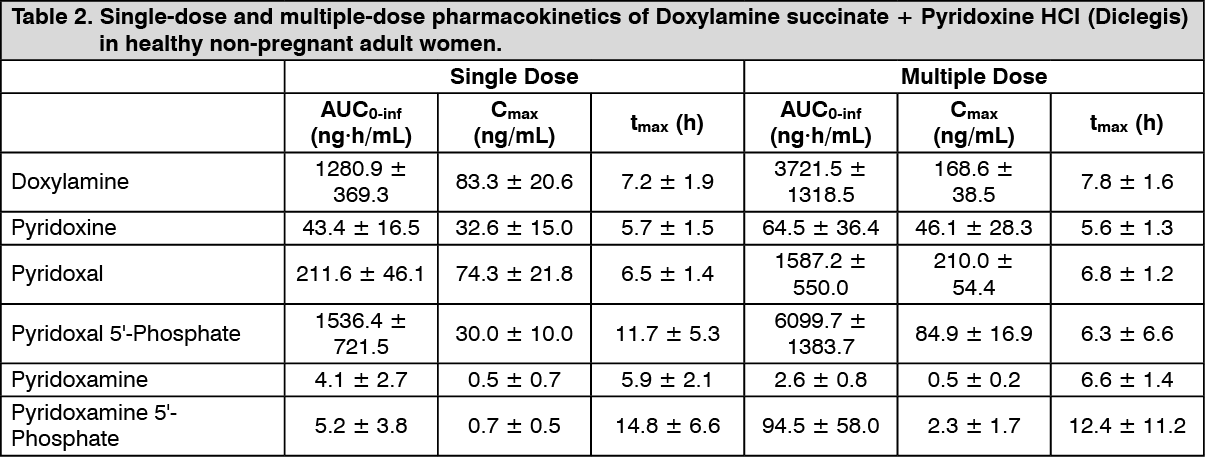 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image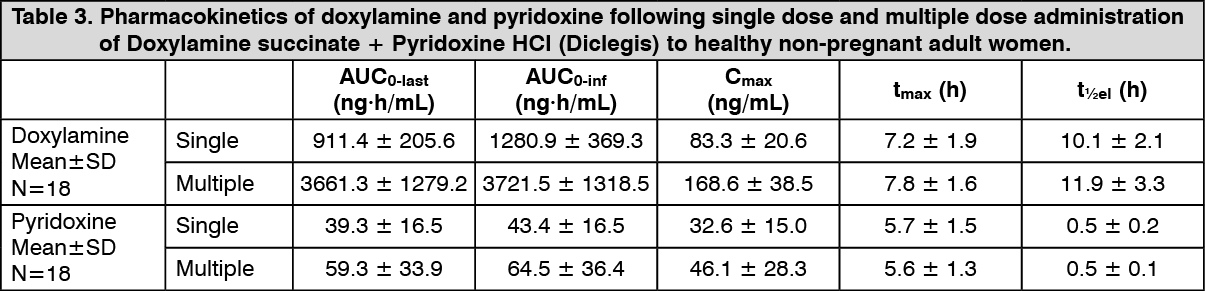 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image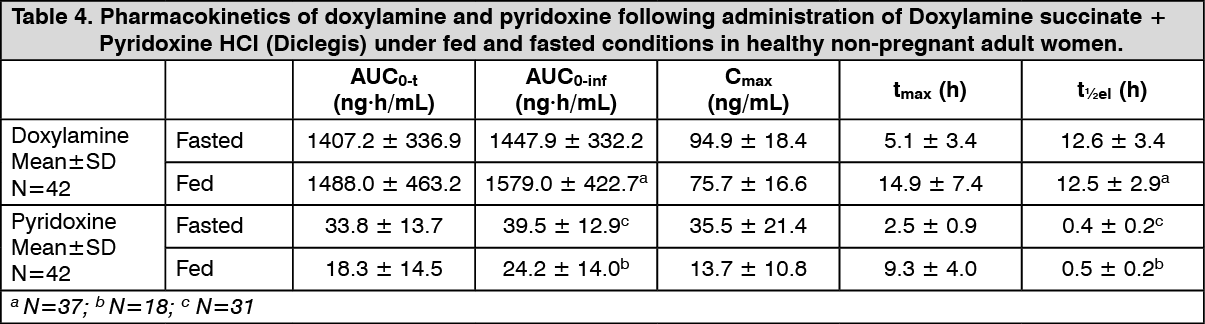 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image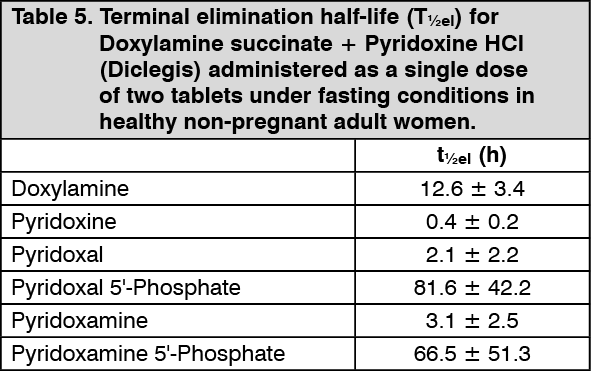 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
