The most common adverse effects of docetaxel are infection, neutropenia, anemia, febrile neutropenia, hypersensitivity, thrombocytopenia, neuropathy, dysgeusia, dyspnea, constipation, anorexia, nail disorders, fluid retention, asthenia, pain, nausea, diarrhea, vomiting, mucositis, alopecia, skin reactions, and myalgia.
Infections and infestations: Sepsis, bronchopneumonia, lower respiratory tract infection, conjunctivitis, otitis media.
Neoplasms benign, malignant and unspecified (incl cysts and polyps): Cancer pain, acute myeloid leukemia, myelodysplastic syndrome.
Blood and lymphatic system disorders: Lymphedema, lower limb edema, neutropenic infection, peripheral lymphedema, neutropenic enterocolitis, leukopenia, disseminated intravascular coagulation (DIC), jaundice, myelosuppression.
Immune system disorders: Allergic reaction, erythema multiforme, Stevens-Johnson syndrome, bronchospasm, fatal anaphylaxis.
Endocrine disorders: Amenorrhea, irregular menstruation.
Metabolism and nutrition disorders: Edema, hyponatremia, dehydration, respiratory failure, peripheral edema.
Psychiatric disorders: Confusion, insomnia, somnolence.
Nervous system disorders: Paresthesia, dysesthesia, burning sensation, dizziness, seizure, transient loss of consciousness, headache, hypoesthesia, peripheral sensory neuropathy, peripheral motor neuropathy.
Eye disorders: Lacrimation disorder, tearing which may be attributable to lacrimal duct obstruction, visual disturbances (flashes, flashing lights, scotomata).
Ear and labyrinth disorders: Hearing disorders, hearing loss.
Cardiac disorders: Chest pain, congestive heart failure, tachycardia, sinus tachycardia, supraventricular tachycardia, atrial flutter, dysrhythmia, unstable angina, pulmonary edema, myocardial ischemia, atrial fibrillation, palpitations, chest tightness, dyspnea, myocardial infarction, arrhythmia, cardiac failure, dilated cardiomyopathy.
Vascular disorders: Hypotension, postural hypotension, hypertension, syncope, vasodilation, superficial and deep vein thrombosis, thrombophlebitis, hot flashes, ischemic colitis, hemorrhoids, hemorrhage, flushing, anaphylactic shock, epistaxis, venous thromboembolic event.
Respiratory, thoracic and mediastinal disorders: Pulmonary embolism, cough, pharyngitis, acute respiratory distress syndrome, interstitial lung disease, pulmonary fibrosis, rhinitis, lung infiltration, altered sense of smell, pleural effusion, radiation pneumonitis, non-cardiac chest pain.
Gastrointestinal disorders: Oral candidiasis, dry mouth, stomatitis, abdominal pain, esophagitis, esophageal ulcer, dysphagia, odynophagia, gastrointestinal pain/cramping, heartburn, gastrointestinal bleeding, gastrointestinal perforation, colitis, intestinal obstruction, ileus, duodenal ulcer, sore throat, abdominal distention, enteritis, ulceration of lips, tongue and oral cavity, dyspepsia.
Hepatobiliary disorders: Hepatitis, hepatic failure, hepatic coma, hepatotoxicity.
Skin and subcutaneous tissue disorders: Bullous eruptions, hand and foot syndrome, nail discoloration, onycholysis, rash/desquamation, dermatitis, dry skin, rash with or without pruritus, hyperpigmentation, erythema, dryness of skin, erythrodysesthesia.
Musculoskeletal and connective tissue disorders: Pain in limb, bone pain, chills, cutaneous lupus erythematosus, scleroderma-like changes, back pain, arthralgia.
Renal and urinary disorders: Renal failure, renal insufficiency.
Reproductive system and breast disorders: Amenorrhea.
General disorders and administration site conditions: Fever, treatment related mortality, fatigue, multi-organ failure, drug fever, inflammation, extravasation, lethargy, septic death, non-septic death, fever in absence of infection.
Investigations: ECG abnormalities, weight loss, weight gain, increased serum creatinine, decreased hemoglobin, prothrombin level decreased, increased serum levels of AST, ALT, bilirubin and alkaline phosphatase, left ventricular ejection fraction (LVEF) deterioration, abnormal liver function test.
Injury, poisoning and procedural complications: Radiation recall phenomenon, phlebitis, toxic epidermal necrolysis, skin toxicity, cystoid macular edema, ototoxicity, hematologic toxicity, neuromotor toxicity, neurocortical toxicity, neurocerebellar toxicity, infusion site reaction.


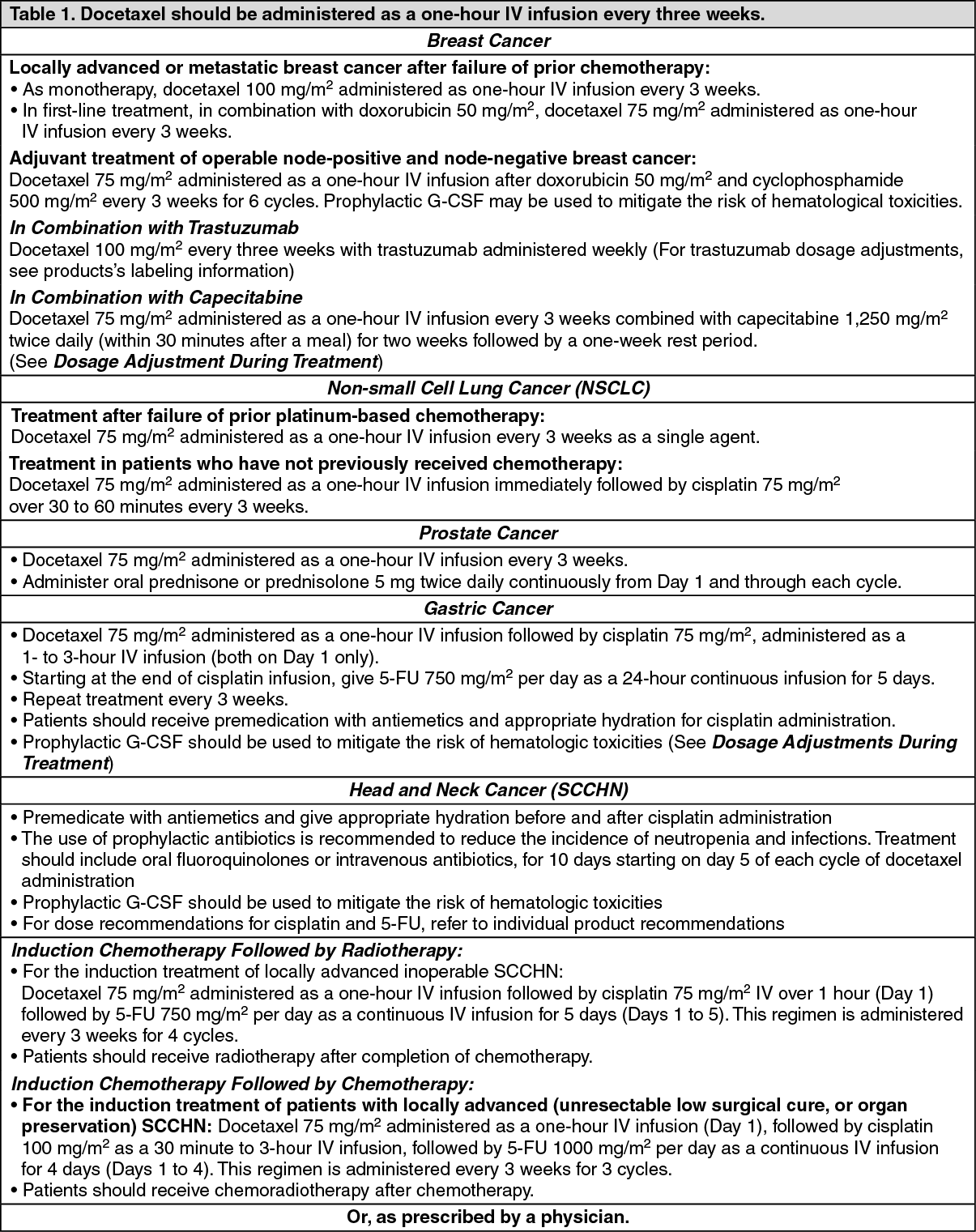 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image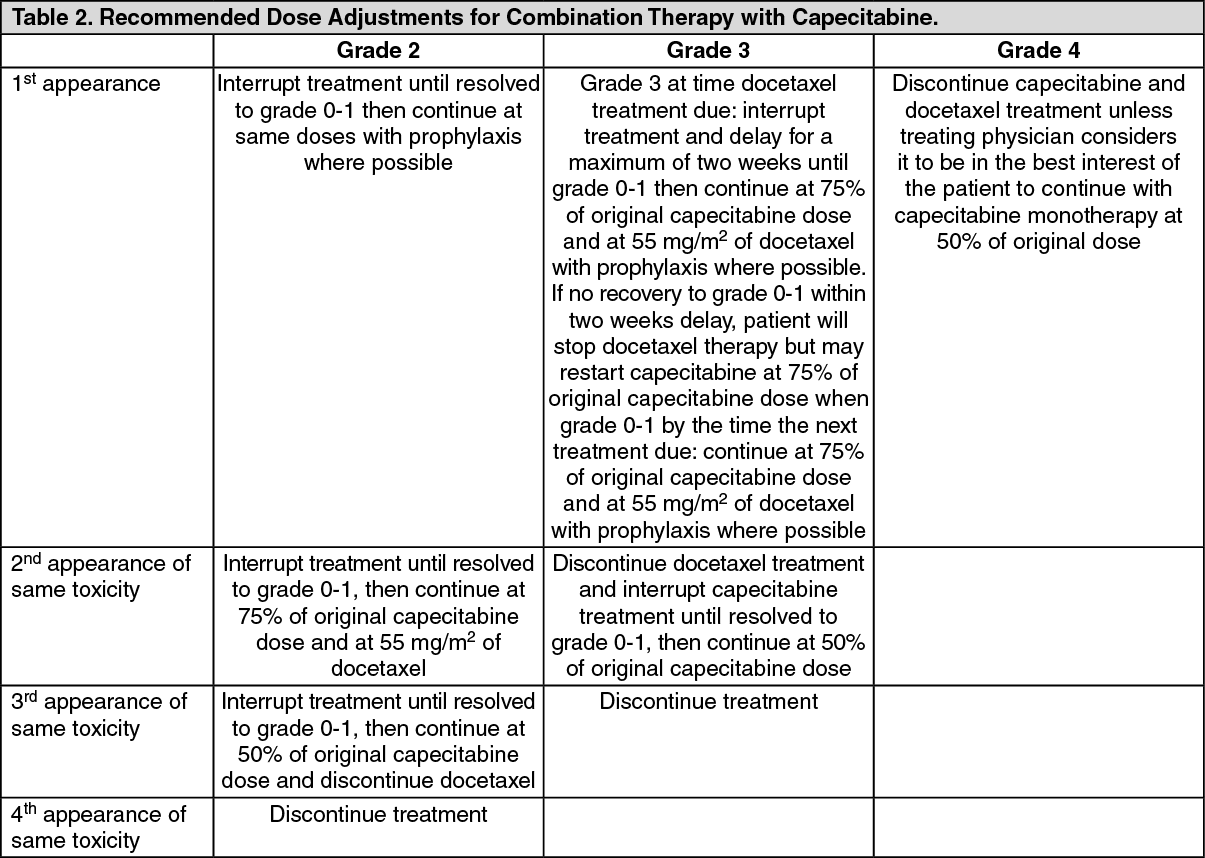 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image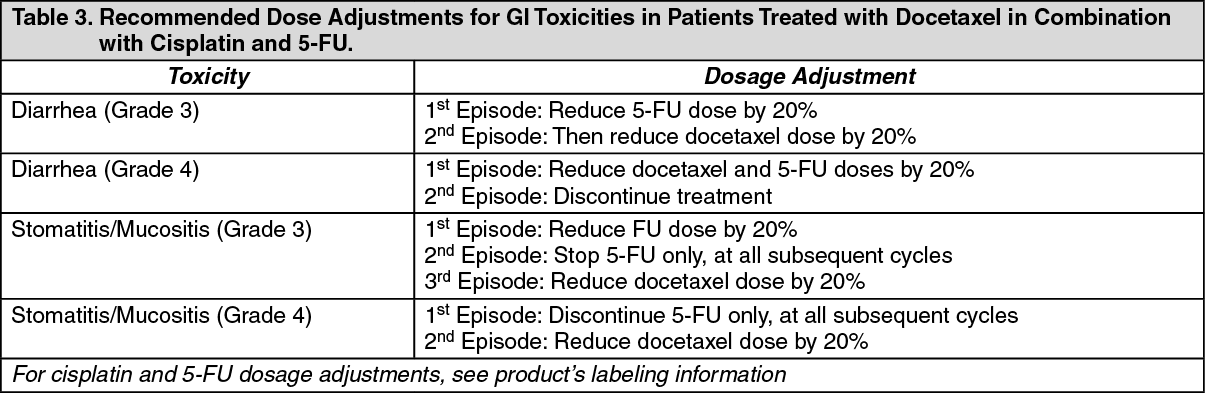 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image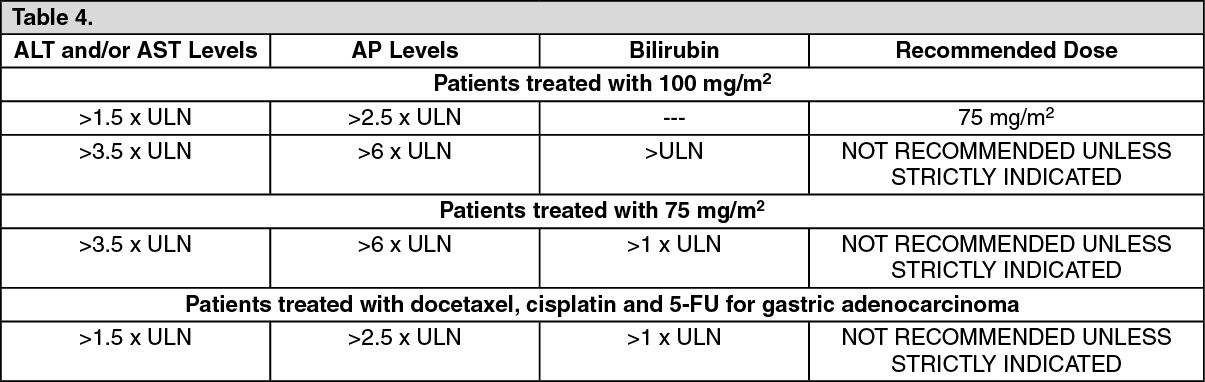 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out