Tadalafil, tamsulosin hydrochloride.
Each capsule contains: Tadalafil, USP 5mg, Tamsulosin hydrochloride, USP 400 mcg.
Pharmacology: Pharmacodynamics: Tadalafil: Tadalafil is a selective, reversible inhibitor of cyclic guanosine monophosphate (cGMP)-specific phosphodiesterase type 5 (PDE5).
The effect of PDE5 inhibition on cGMP concentration in the corpus cavernosum is also observed in the smooth muscle of the prostate, the bladder and their vascular supply. The resulting vascular relaxation increases blood perfusion, which may be the mechanism by which symptoms of benign prostatic hyperplasia are reduced. These vascular effects may be complemented by inhibition of bladder afferent nerve activity and smooth muscle relaxation of the prostate and bladder.
Tamsulosin: Tamsulosin binds selectively and competitively to postsynaptic alpha1-receptors, in particular to the subtype alpha1A, which bring about relaxation of the smooth muscle of the prostate, whereby tension is reduced.
Tamsulosin increases maximum urinary flow rate by reducing smooth muscle tension in the prostate and urethra, thereby relieving obstruction.
It also improves the complex of irritative and obstructive symptoms in which bladder instability and tension of the smooth muscles of the lower urinary tract play an important role. Alpha1-blockers can reduce blood pressure by lowering peripheral resistance. No reduction in blood pressure of any clinical significance was observed during studies with Tamsulosin.
Pharmacokinetics: Tadalafil: Absorption: Tadalafil is readily absorbed after oral administration and the mean maximum observed plasma concentration (Cmax) is achieved at a median time of 2 hours after dosing. Absolute bioavailability of Tadalafil following oral dosing has not been determined.
The rate and extent of absorption of Tadalafil are not influenced by food, thus Tadalafil may be taken with or without food. The time of dosing (morning versus evening) had no clinically relevant effects on the rate and extent of absorption.
Distribution: The mean volume of distribution is approximately 63 liters, indicating that Tadalafil is distributed into tissues. At therapeutic concentrations, 94% of Tadalafil in plasma is bound to proteins. Protein binding is not affected by impaired renal function.
Less than 0.0005% of the administered dose appeared in the semen of healthy subjects.
Biotransformation: Tadalafil is predominantly metabolized by the cytochrome P450 (CYP) 3A4 isoform. The major circulating metabolite is the methylcatechol glucuronide. This metabolite is at least 13,000-fold less potent than Tadalafil for PDE5. Consequently, it is not expected to be clinically active at observed metabolite concentrations.
Elimination: The mean oral clearance for Tadalafil is 2.5 l/h and the mean half-life is 17.5 hours in healthy subjects. Tadalafil is excreted predominantly as inactive metabolites, mainly in the feces (approximately 61% of the dose) and to a lesser extent in the urine (approximately 36% of the dose).
Tamsulosin: Absorption: Tamsulosin hydrochloride administered as prolonged release tablets is absorbed from the intestine. Under fasting conditions, approximately 57% of the administered dose is estimated to be absorbed. A consistent slow release of tamsulosin is maintained over the whole pH range encountered in the gastro-intestinal tract with little fluctuation over 24 hours. The extent of absorption is increased by 64% and 149% (AUC and Cmax respectively) by a high fat meal compared to fasted. After a single dose of Tamsulosin in the fasted state, plasma levels of tamsulosin peak at a median time of 6 hours. In steady state, which is reached by day 4 of multiple dosing, plasma levels of tamsulosin peak at 4 to 6 hours in the fasted and fed state. Peak plasma levels increase from approximately 6 ng/ml after the first dose to 11 ng/ml in steady state.
As a result of the prolonged release characteristics of Tamsulosin, the trough concentration of tamsulosin in plasma amounts to 40% of the peak plasma concentration under fasted and fed conditions.
There is a considerable inter-patient variation in plasma levels, both after single and after multiple dosing.
Distribution: In man, tamsulosin is about 99% bound to plasma proteins and volume of distribution is small (about 0.2 l/kg).
Metabolism: Tamsulosin has a low first pass effect, being metabolized slowly.
Most tamsulosin is present in plasma in the form of unchanged drug. It is metabolized in the liver.
In rats, hardly any induction of microsomal liver enzymes was seen to be caused by tamsulosin.
In vitro results suggest that CYP3A4 and also CYP2D6 are involved in metabolism, with possible minor contributions to tamsulosin hydrochloride metabolism by other CYP isozymes. Inhibition of CYP3A4 and CYP2D6 drug metabolizing enzymes may lead to increased exposure to tamsulosin hydrochloride.
No dose adjustment is warranted in hepatic insufficiency.
None of the metabolites are more active than the original compound.
Elimination: Tamsulosin and its metabolites are mainly excreted in the urine. The amount excreted as unchanged drug is estimated to be about 4-6% of the dose, administered as Tamsulosin.
After a single dose of Tamsulosin, and in steady state, elimination half-lives of about 19 and 15 hours, respectively, have been measured.
No dose adjustment is necessary in patients with renal impairment.
Toxicology: Preclinical Safety Data: Tadalafil: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, and toxicity to reproduction.
There was no evidence of teratogenicity, embryotoxicity or fetotoxicity in rats or mice that received up to 1000 mg/kg/day Tadalafil. In a rat prenatal and postnatal development study, the no observed effect dose was 30 mg/kg/day.
In the pregnant rat, the AUC for calculated free drug at this dose was approximately 18 times the human AUC at a 20 mg dose.
There was no impairment of fertility in male and female rats. In dogs given Tadalafil daily for 6 to 12 months at doses of 25 mg/kg/day (resulting in at least a 3-fold greater exposure [range 3.7-18.6] than seen in humans given a single 20 mg dose) and above, there was regression of the seminiferous tubular epithelium that resulted in a decrease in spermatogenesis in some dogs.
Tamsulosin: Single and repeat dose toxicity studies were performed in mice, rats and dogs. In addition, reproduction toxicity studies were performed in rats, carcinogenicity in mice and rats, and in vivo and in vitro genotoxicity were examined. The general toxicity profile, as seen with high doses of tamsulosin, is consistent with the known pharmacological actions of the alpha-adrenergic blocking agents. At very high dose levels, the ECG was altered in dogs. This response is considered to be not clinically relevant. Tamsulosin showed no relevant genotoxic properties.
Increased incidences of proliferative changes of mammary glands of female rats and mice have been reported. These findings, which are probably mediated by hyperprolactinaemia and only occurred at high dose levels, are regarded as irrelevant.
Indicated for the treatment of lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH).
Recommended dose is one capsule daily can be taken independently of food. Should be swallowed whole. Do not crush or chew. Or as prescribed by the physician.
Special populations: Renal Impairment: No dose adjustment is required in patients with mild to moderate renal impairment.
Hepatic Impairment: No dose adjustment is required in patients with mild to moderate hepatic impairment.
Pediatric Population: The safety and efficacy of Tamsulosin/Tadalafil combination in children <18 years have not been established.
Tadalafil: Single doses of up to 500 mg have been given to healthy subjects, and multiple daily doses up to 100 mg have been given to patients. Adverse events were similar to those seen at lower doses. In cases of overdose, standard supportive measures should be adopted as required. Hemodialysis contributes negligibly to Tadalafil elimination.
Tamsulosin: Symptoms: Overdosage with tamsulosin hydrochloride can potentially result in severe hypotensive effects, dizziness and malaise. Severe hypotensive effects have been observed at different levels of overdosing.
Treatment: In case of acute hypotension occurring after overdose, cardiovascular support should be given. Blood pressure can be restored and heart rate brought back to normal by lying the patient down. If this does not help, then volume expanders, and when necessary, vasopressors could be employed. Renal function should be monitored and general supportive measures applied. Dialysis is unlikely to be of help, as tamsulosin is very highly bound to plasma proteins.
Measures, such as emesis, can be taken to impede absorption. When large quantities are involved, gastric lavage can be applied and activated charcoal and an osmotic laxative, such as sodium sulfate, can be administered.
Hypersensitivity to Tamsulosin, or Tadalafil, or to any of the excipients.
A history of orthostatic hypotension.
Severe hepatic insufficiency.
In clinical studies, Tadalafil was shown to augment the hypotensive effects of nitrates. This is thought to result from the combined effects of nitrates and Tadalafil on the nitric oxide/cGMP pathway. Therefore, administration of Tadalafil to patients who are using any form of organic nitrate is contraindicated.
The following groups of patients with cardiovascular disease were not included in clinical trials and the use of Tadalafil is therefore contraindicated: Patients with myocardial infarction within the last 90 days; Patients with unstable angina or angina occurring during sexual intercourse; Patients with New York Heart Association Class 2 or greater heart failure in the last 6 months; Patients with uncontrolled arrhythmias, hypotension (< 90/50 mmHg), or uncontrolled hypertension; Patients with a stroke within the last 6 months.
Tadalafil is contraindicated in patients who have loss of vision in one eye because of non-arteritic anterior ischemic optic neuropathy (NAION), regardless of whether this episode was in connection or not with previous PDE5 inhibitor exposure.
The co-administration of PDE5 inhibitors, including Tadalafil, with guanylate cyclase stimulators, such as riociguat, is contraindicated as it may potentially lead to symptomatic hypotension.
Tadalafil: Before treatment with Tadalafil: A medical history and physical examination should be undertaken to diagnose benign prostatic hyperplasia and determine potential underlying causes, before pharmacological treatment is considered.
Tadalafil has vasodilator properties, resulting in mild and transient decreases in blood pressure and as such potentiates the hypotensive effect of nitrates.
Prior to initiating treatment with Tadalafil for benign prostatic hyperplasia patients should be examined to rule out the presence of carcinoma of the prostate and carefully assessed for cardiovascular conditions.
Cardiovascular: In patients receiving concomitant antihypertensive medicinal products, Tadalafil may induce a blood pressure decrease. When initiating daily treatment with Tadalafil, appropriate clinical considerations should be given to a possible dose adjustment of the antihypertensive therapy.
In patients who are taking alpha1 blockers, concomitant administration of Tadalafil may lead to symptomatic hypotension in some patients. The combination of Tadalafil and Doxazosin is not recommended.
Vision: Visual defects and cases of NAION have been reported in connection with the intake of Tadalafil and other PDE5 inhibitors. The patient should be advised that in case of sudden visual defect, should stop taking Tadalafil and consult a physician immediately.
Renal and hepatic impairment: Due to increased Tadalafil exposure (AUC), limited clinical experience and the lack of ability to influence clearance by dialysis, once-a-day dosing of Tadalafil is not recommended in patients with severe renal impairment. There is limited clinical data on the safety of single-dose administration of Tadalafil in patients with severe hepatic insufficiency (Child-Pugh Class C). Once-a-day administration for the treatment of benign prostatic hyperplasia has not been evaluated in patients with hepatic insufficiency. If Tadalafil is prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician.
Priapism and anatomical deformation of the penis: Patients who experience erections lasting 4 hours or more should be instructed to seek immediate medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of potency may result.
Tadalafil, should be used with caution in patients with anatomical deformation of the penis (such as angulation, cavernosal fibrosis or Peyronie's disease), or in patients who have conditions which may predispose them to priapism (such as sickle cell anemia, multiple myeloma or leukemia).
Use with CYP3A4 inhibitors: Caution should be exercised when prescribing Tadalafil to patients using potent CYP3A4 inhibitors (ritonavir, saquinavir, ketoconazole, itraconazole, and erythromycin) as increased Tadalafil exposure (AUC) has been observed if the medicinal products are combined.
Tamsulosin: As with other alpha1 blockers, a reduction in blood pressure can occur in individual cases during treatment with Tamsulosin, as a result of which, rarely, syncope can occur. At the first signs of orthostatic hypotension (dizziness, weakness), the patient should sit or lie down until the symptoms have disappeared.
Before therapy with Tamsulosin is initiated, the patient should be examined in order to exclude the presence of other conditions, which can cause the same symptoms as benign prostatic hyperplasia. Digital rectal examination and, when necessary, determination of prostate specific antigen (PSA) should be performed before treatment and at regular intervals afterwards.
The treatment of severely renally impaired patients (creatinine clearance of less than 10 ml/min) should be approached with caution, as these patients have not been studied.
The 'Intraoperative Floppy Iris Syndrome' (IFIS, a variant of small pupil syndrome) has been observed during cataract and glaucoma surgery in some patients on or previously treated with tamsulosin hydrochloride. IFIS may increase the risk of eye complications during and after the operation.
Discontinuing tamsulosin hydrochloride 1-2 weeks prior to cataract or glaucoma surgery is anecdotally considered helpful, but the benefit of treatment discontinuation has not been established. IFIS has also been reported in patients who had discontinued tamsulosin for a longer period prior to the surgery.
The initiation of therapy with tamsulosin hydrochloride in patients for whom cataract or glaucoma surgery is scheduled is not recommended. During pre-operative assessment, surgeons and ophthalmic teams should consider whether patients scheduled for cataract or glaucoma surgery are being or have been treated with tamsulosin in order to ensure that appropriate measures will be in place to manage the IFIS during surgery.
Tamsulosin hydrochloride should not be given in combination with strong inhibitors of CYP3A4 (e.g. ketoconazole) in patients with poor metabolizer CYP2D6 phenotype.
Tamsulosin hydrochloride should be used with caution in combination with strong (e.g. ketoconazole) and moderate (e.g. erythromycin) inhibitors of CYP3A4.
Effects on Ability to Drive and Use Machine: No studies on the effects on the ability to drive and use machines have been performed. However, patients should be aware of the fact that drowsiness, blurred vision, dizziness and syncope can occur.
Tamsulosin/Tadalafil combination is not indicated for use in women.
Pregnancy: There are limited data from the use of Tadalafil in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/fetal development, parturition or postnatal development.
As a precautionary measure, it is preferable to avoid the use of Tamsulosin/Tadalafil combination during pregnancy.
Breastfeeding: Available Pharmacodynamic/Toxicological data in animals have shown excretion of Tadalafil in milk. A risk to the suckling child cannot be excluded. Tamsulosin/Tadalafil combination should not be used during breast-feeding.
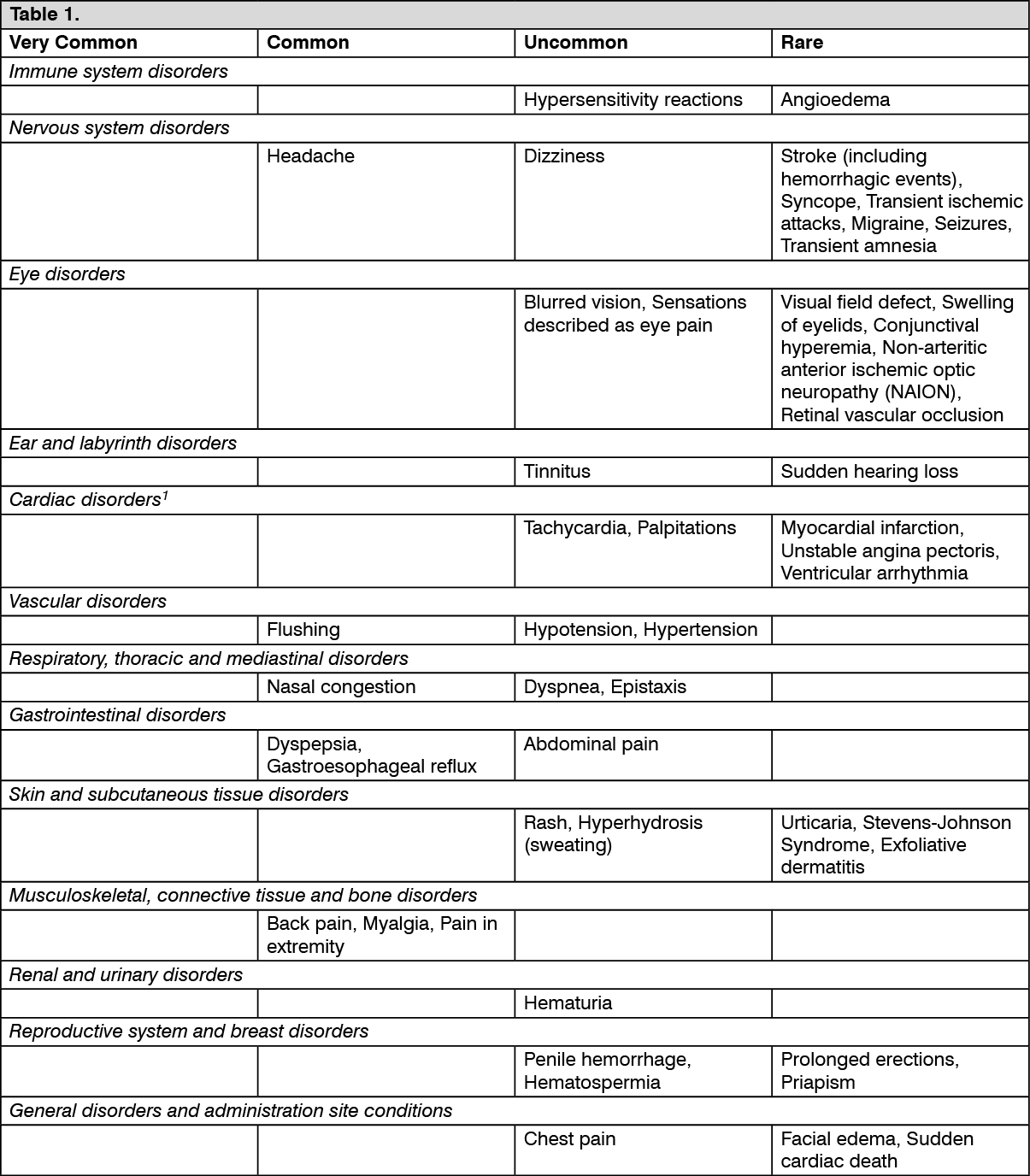
Tadalafil: The most commonly reported adverse reactions in patients taking Tadalafil for the treatment of benign prostatic hyperplasia were headache, dyspepsia, back pain and myalgia, in which the incidences increase with increasing dose of Tadalafil. The adverse reactions reported were transient, and generally mild or moderate. The majority of headaches reported with Tadalafil once-day dosing are experienced within the first 10 to 30 days of starting treatment.
Tabulated summary of adverse reactions: The table as follows lists the adverse reactions observed from spontaneous reporting and in placebo controlled clinical trials (comprising a total of 7116 patients on Tadalafil and 3718 patients on placebo) for on-demand and once-a-day treatment of erectile dysfunction and the once-a-day treatment of benign prostatic hyperplasia.
Frequency convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10,000 to <1/1,000) and very rare (<1/10,000) and not known (cannot be estimated from the available data). (See Table 1.)
 Click on icon to see table/diagram/image
Tamsulosin: Tabulated list of adverse reactions:
Click on icon to see table/diagram/image
Tamsulosin: Tabulated list of adverse reactions: See Table 2.
Click on icon to see table/diagram/image
As with other alpha-blockers, drowsiness, blurred vision or edema can occur.
During cataract and glaucoma surgery a small pupil situation, known as Intraoperative Floppy Iris Syndrome (IFIS), has been associated with therapy of tamsulosin during post-marketing surveillance.
Post-marketing experience: In addition to the adverse events listed previously, atrial fibrillation, arrhythmia, tachycardia and dyspnea have been reported in association with tamsulosin use. Because these spontaneously reported events are from the worldwide post marketing experience, the frequency of events and the role of tamsulosin in their causation cannot be reliably determined.
Tadalafil: Effects of other substances on Tadalafil: Cytochrome P450 inhibitors: Tadalafil is principally metabolized by CYP3A4. A selective inhibitor of CYP3A4, Ketoconazole (200 mg daily), increased Tadalafil (10 mg) exposure (AUC) 2-fold and Cmax by 15%, relative to the AUC and Cmax values for Tadalafil alone. Ketoconazole (400 mg daily) increased Tadalafil (20 mg) exposure (AUC) 4-fold and Cmax by 22%. Ritonavir, a protease inhibitor (200 mg twice daily), which is an inhibitor of CYP3A4, CYP2C9, CYP2C19, and CYP2D6, increased Tadalafil (20 mg) exposure (AUC) 2-fold with no change in Cmax. Although specific interactions have not been studied, other protease inhibitors, such as saquinavir, and other CYP3A4 inhibitors, such as Erythromycin, Clarithromycin, Itraconazole and grapefruit juice should be co-administered with caution as they would be expected to increase plasma concentrations of Tadalafil.
Transporters: The role of transporters (for example p-glycoprotein) in the disposition of Tadalafil is not known. Therefore, there is the potential of drug interactions mediated by inhibition of transporters.
Cytochrome P450 inducers: A CYP3A4 inducer, Rifampicin, reduced Tadalafil AUC by 88%, relative to the AUC values for Tadalafil alone (10 mg). This reduced exposure can be anticipated to decrease the efficacy of Tadalafil; the magnitude of decreased efficacy is unknown. Other inducers of CYP3A4 such as phenobarbital, phenytoin and carbamazepine, may also decrease plasma concentrations of Tadalafil.
Effects of Tadalafil on other medicinal products: Nitrates: In a patient prescribed any dose of Tadalafil (2.5 mg-20 mg), where nitrate administration is deemed medically necessary in a life-threatening situation, at least 48 hours should have elapsed after the last dose of Tadalafil before nitrate administration is considered. In such circumstances, nitrates should only be administered under close medical supervision with appropriate hemodynamic monitoring.
Anti-hypertensives (including calcium channel blockers): The co-administration of doxazosin (4 and 8 mg daily) and Tadalafil (5 mg daily dose and 20 mg as a single dose) increases the blood pressure-lowering effect of this alpha-blocker in a significant manner. This effect lasts at least twelve hours and may be symptomatic, including syncope. Therefore, this combination is not recommended.
Caution should be exercised when using Tadalafil in patients treated with any alpha-blockers, and notably in the elderly. Treatments should be initiated at minimal dosage and progressively adjusted.
However, appropriate clinical advice should be given to patients regarding a possible decrease in blood pressure when they are treated with antihypertensive medicinal products.
Riociguat: Preclinical studies showed an additive systemic blood pressure lowering effect when PDE5 inhibitors were combined with riociguat. In clinical studies, riociguat has been shown to augment the hypotensive effects of PDE5 inhibitors. There was no evidence of favorable clinical effect of the combination in the population studied.
Concomitant use of riociguat with PDE5 inhibitors, including Tadalafil, is contraindicated.
5-alpha reductase inhibitors: In a clinical trial that compared Tadalafil 5 mg co-administered with Finasteride 5 mg to placebo plus Finasteride 5 mg in the relief of BPH symptoms, no new adverse reactions were identified. However, as a formal drug-drug interaction study evaluating the effects of Tadalafil and 5-alpha reductase inhibitors (5-ARIs) has not been performed, caution should be exercised when Tadalafil is co-administered with 5-ARIs.
CYP1A2 substrates (e.g. theophylline): When Tadalafil 10 mg was administered with Theophylline (a non-selective phosphodiesterase inhibitor) in a clinical pharmacology study, there was no pharmacokinetic interaction. The only pharmacodynamic effect was a small (3.5 bpm) increase in heart rate. Although this effect is minor and was of no clinical significance in this study, it should be considered when co-administering these medicinal products.
Ethinylestradiol and Terbutaline: Tadalafil has been demonstrated to produce an increase in the oral bioavailability of ethinylestradiol; a similar increase may be expected with oral administration of terbutaline, although the clinical consequence of this is uncertain.
Cytochrome P450 metabolized medicinal products: Tadalafil is not expected to cause clinically significant inhibition or induction of the clearance of medicinal products metabolized by CYP450 isoforms. Studies have confirmed that Tadalafil does not inhibit or induce CYP450 isoforms, including CYP3A4, CYP1A2, CYP2D6, CYP2E1, CYP2C9 and CYP2C19.
Antidiabetic medicinal products: Specific interaction studies with antidiabetic medicinal products were not conducted.
Tamsulosin: No interactions have been seen when tamsulosin was given concomitantly with atenolol, enalapril, or theophylline. Concomitant cimetidine brings about a rise in plasma levels of tamsulosin, and furosemide a fall, but as levels remain within the normal range, posology need not be changed.
In vitro, neither diazepam nor propranolol, trichlormethiazide, chlormadinon, amitriptyline, diclofenac, glibenclamide, simvastatin and warfarin change the free fraction of tamsulosin in human plasma. Neither does tamsulosin change the free fractions of diazepam, propranolol, trichlormethiazide, and chlormadinon.
Diclofenac and warfarin, however, may increase the elimination rate of tamsulosin.
Concomitant administration of tamsulosin hydrochloride with strong inhibitors of CYP3A4 may lead to increased exposure to tamsulosin hydrochloride. Concomitant administration with ketoconazole (a known strong CYP3A4 inhibitor) resulted in an increase in AUC and Cmax of tamsulosin hydrochloride by a factor of 2.8 and 2.2, respectively.
Tamsulosin hydrochloride should not be given in combination with strong inhibitors of CYP3A4 (e.g. ketoconazole) in patients with poor metabolizer CYP2D6 phenotype.
Tamsulosin hydrochloride should be used with caution in combination with strong (e.g. ketoconazole) and moderate inhibitors (e.g. erythromycin) of CYP3A4.
Concomitant administration of tamsulosin hydrochloride with paroxetine, a strong inhibitor of CYP2D6, resulted in a Cmax and AUC of tamsulosin that had increased by a factor of 1.3 and 1.6, respectively, but these increases are not considered clinically relevant.
There is a theoretical risk of enhanced hypotensive effect when given concurrently with drugs, which may reduce blood pressure, including anesthetic agents and other α1-adrenoceptor antagonists.
Store at temperatures not exceeding 30°C.
G04CA54 - tamsulosin and tadalafil ; Belongs to the class of alpha-adrenoceptor antagonist and other urological drug. Used in the treatment of benign prostatic hypertrophy and other urological disease.
Duactam cap
30's (P51.5/cap)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image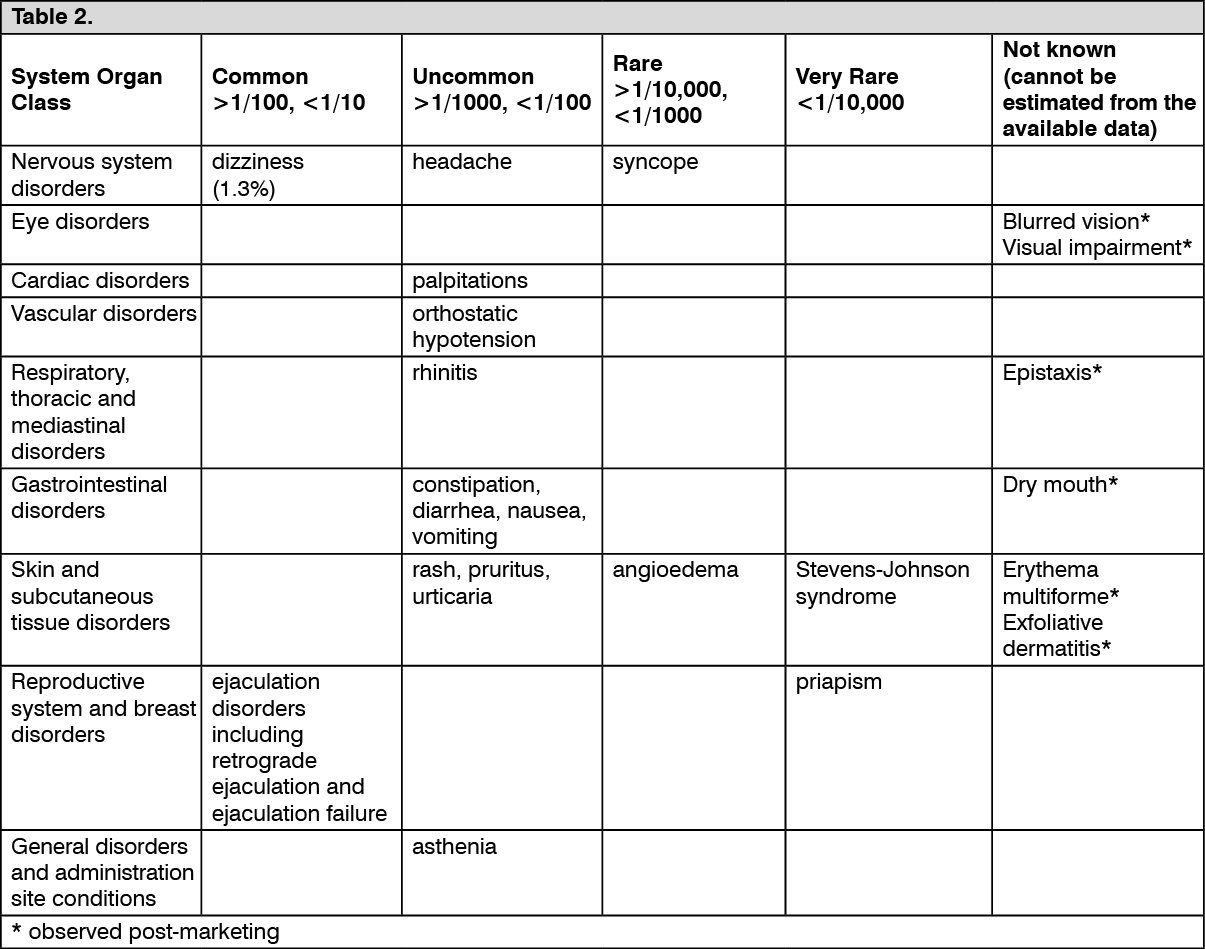 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out