


 Sign Out
Sign Out



In men with osteoporosis, similar patterns in bone turnover marker changes were observed.
After discontinuation of romosozumab (EVENITY) therapy in postmenopausal women with osteoporosis, P1NP levels returned to baseline within 12 months; CTX increased above baseline levels within 3 months and returned toward baseline levels by month 12, reflecting reversibility of effect. Upon retreatment with romosozumab (EVENITY) after 12 months off treatment, the level of increase in P1NP and decrease in CTX by romosozumab (EVENITY) was similar to that observed during the initial treatment.
In women transitioning from oral alendronate, romosozumab (EVENITY) also increased bone formation and decreased bone resorption.
Mechanism of action: Romosozumab is a humanised monoclonal antibody (IgG2) that binds and inhibits sclerostin, a negative regulator of bone formation predominantly secreted by mature osteocytes. Romosozumab has a dual effect on bone, increasing bone formation and decreasing bone resorption. Romosozumab increases trabecular and cortical bone mass and improves bone structure and strength.
Clinical trials: In post-menopausal women with primary osteoporosis, romosozumab (EVENITY) reduces the risk of vertebral and clinical fractures. Romosozumab (EVENITY) increases bone mass in men and post-menopausal women with primary osteoporosis.
The primary evidence for the efficacy and safety of romosozumab for the treatment of osteoporosis in postmenopausal women was derived from 2 pivotal fracture studies (Study 20110142; ARCH and Study 20070337; FRAME). In addition, a phase 3b study (Study 20080289; STRUCTURE) in women with osteoporosis transitioning from oral bisphosphonate therapy to romosozumab or teriparatide was conducted to provide supportive efficacy and safety. The primary evidence for the efficacy and safety of romosozumab for the treatment of osteoporosis in men was from a 12-month primary analysis of a pivotal, double-blind, placebo-controlled, phase 3 Study 20110174 (BRIDGE). These studies are described in further detail as follows.
Treatment of osteoporosis in postmenopausal women: Study 1 (alendronate-controlled): Active-controlled fracture study in postmenopausal women with osteoporosis at High risk of fracture (ARCH): The efficacy and safety of romosozumab (EVENITY) in the treatment of osteoporosis in postmenopausal women was demonstrated in a multicentre, multinational, randomised, double-blind, alendronate-controlled, superiority study of 4093 postmenopausal women aged 55 to 90 years (mean age of 74.3 years). The mean years since menopause was 26.9 years. Prior use of osteoporosis medications was reported in 9% of patients, with oral bisphosphonates the most frequently reported (6.2%). Baseline characteristics were similar between treatment groups. The mean 10-year probabilities of major osteoporotic fractures and of hip fractures calculated with femoral neck BMD were 20.1% and 9.8% respectively. Enrolled women had either: BMD T-score at the total hip or femoral neck of ≤-2.50, and either at least 1 moderate or severe vertebral fracture; or at least 2 mild vertebral fractures OR; BMD T-score at the total hip or femoral neck of ≤-2.00, and either at least 2 moderate or severe vertebral fractures; or a fracture of the proximal femur that occurred within 3 to 24 months prior to randomisation.
The mean baseline lumbar spine, total hip, and femoral neck BMD T-scores were -2.96, -2.80, and -2.90, respectively, 96.1% of women had a vertebral fracture at baseline, and 99.8% of women had a previous fracture. Women were randomised (1:1) to receive either monthly subcutaneous injections of romosozumab (EVENITY) (N=2046) or oral weekly alendronate (N=2047) in a blinded fashion for 12 months. After the 12-month double-blind study period, women in both arms transitioned to alendronate while remaining blinded to their initial treatment. The primary analysis was performed when all women had completed the month 24 study visit and clinical fracture events were confirmed for at least 330 women and occurred after a median follow-up time of 2.7 years on study. Women received at least 500 mg calcium and 600 IU vitamin D supplementation daily and could have received a loading dose of 50,000 to 60,000 IU of vitamin D after randomisation. 89.3% of randomised women completed the 12-month double-blind period and 77% completed the primary analysis period.
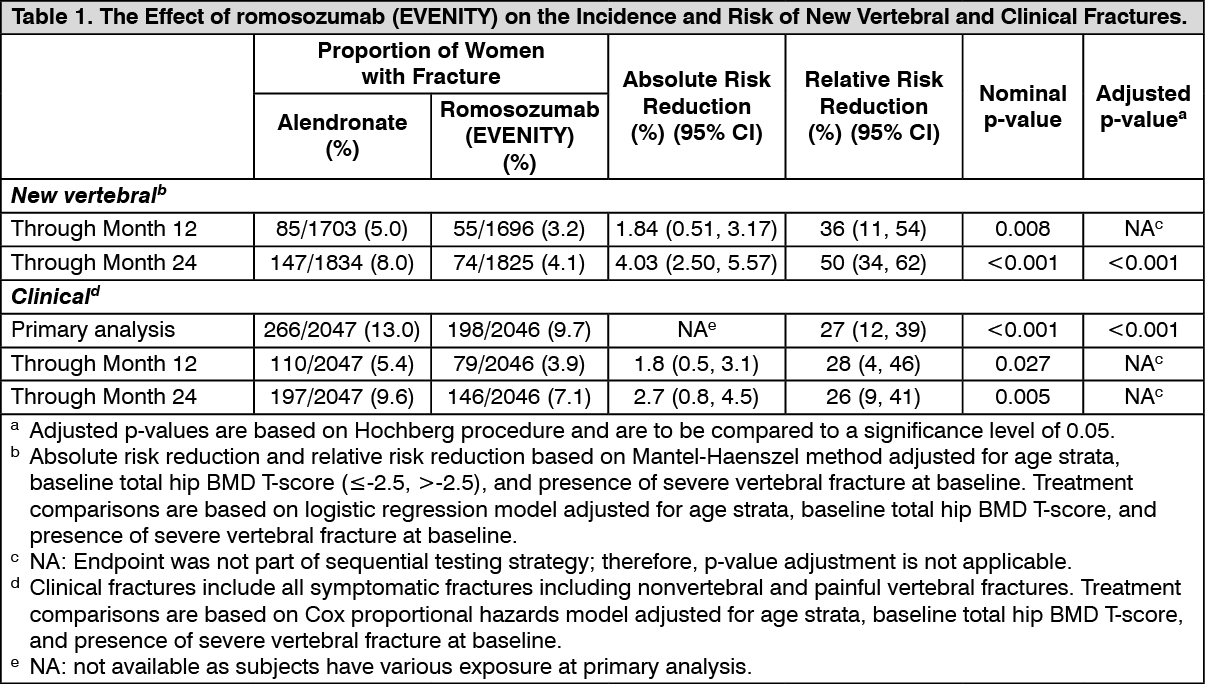
The primary efficacy endpoints were the incidence of new vertebral fracture through month 24 and the incidence of clinical fracture (nonvertebral fracture and clinical vertebral fracture) at primary analysis. Vertebral fractures were diagnosed based on lateral spine radiographs (T4-L4) using a semiquantitative scoring method. Secondary efficacy endpoints included the incidence of nonvertebral fractures, hip fractures, and major nonvertebral fractures at the primary analysis, and percent change from baseline in BMD at the lumbar spine, total hip, and femoral neck at month 12 and month 24.
Effect on new vertebral and clinical fractures: As shown in Table 1, romosozumab (EVENITY) significantly reduced the incidence of new vertebral fracture through month 24 and the incidence of clinical fracture at primary analysis. The fracture risk was reduced as early as month 12. (See Table 1, Figures 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image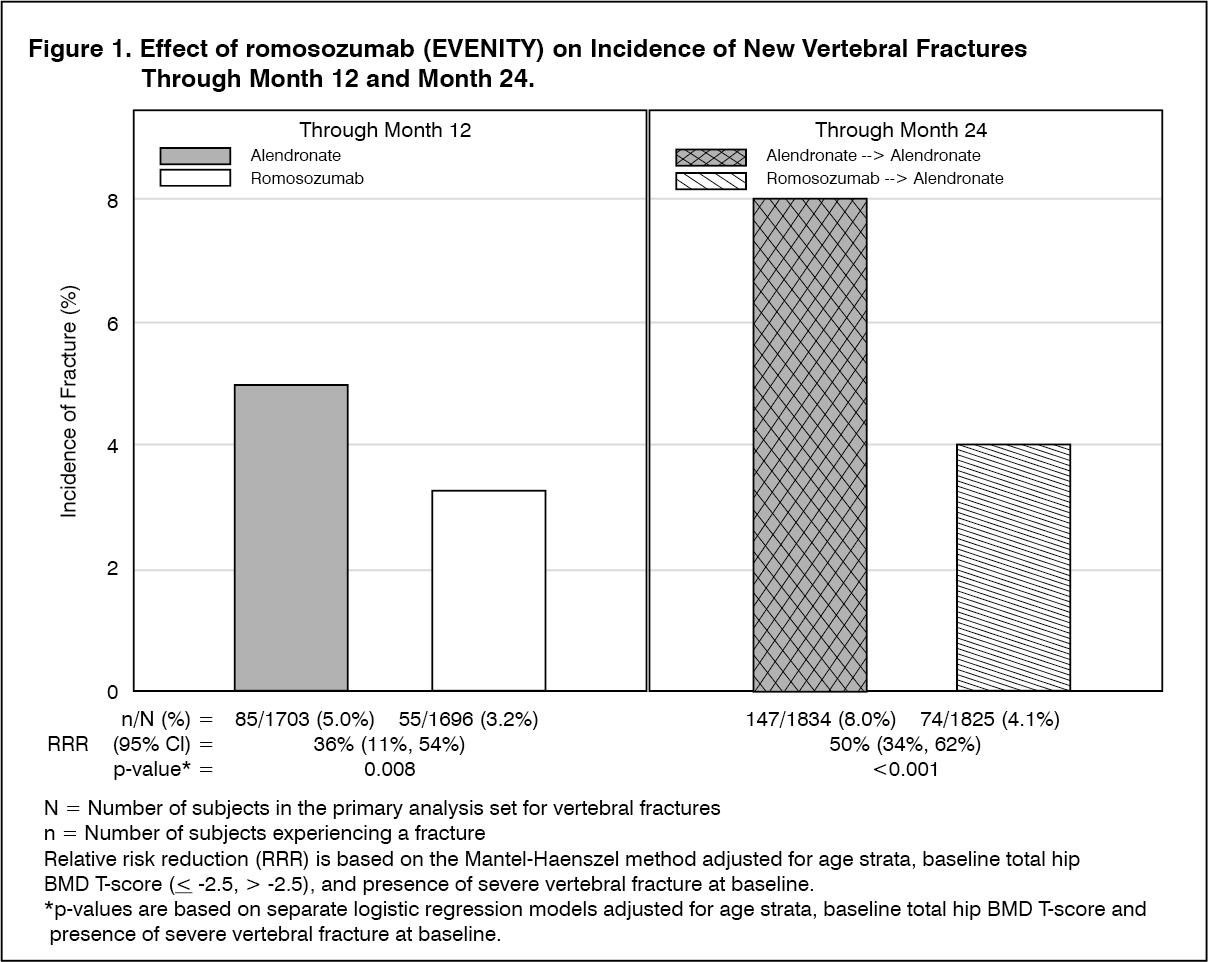 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image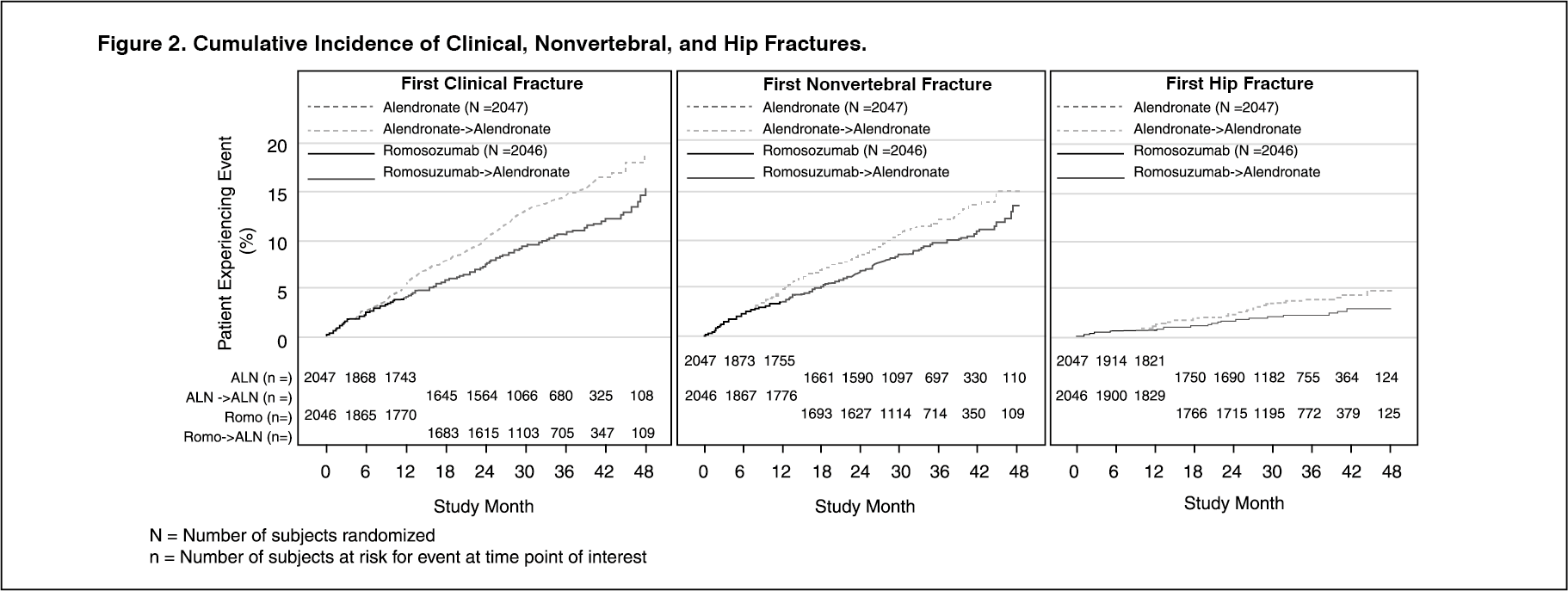 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSubgroup analyses of the primary endpoints showed that romosozumab for 12 months followed by alendronate for 12 months demonstrated a consistent treatment effect, as shown by odds ratios that favoured romosozumab/alendronate over alendronate/alendronate in all subgroups of baseline characteristics examined including age, presence or absence of severe vertebral fracture at baseline, number of prevalent vertebral fractures at baseline, race, geographic region, baseline lumbar spine BMD T-score, baseline total hip/femoral neck BMD T-score, baseline BMI, FRAX score, and history of nonvertebral fracture at or after age 55.
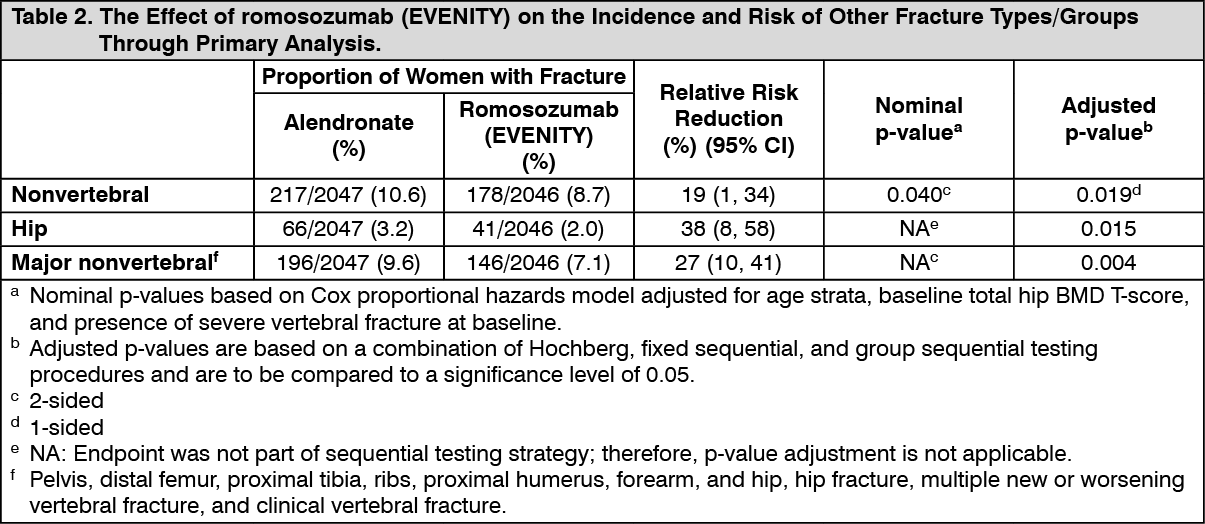
Effect on other fracture types/groups: see Table 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRomosozumab (EVENITY) reduced the incidence of major nonvertebral fractures compared to alendronate as early as Month 12 and through Month 24.
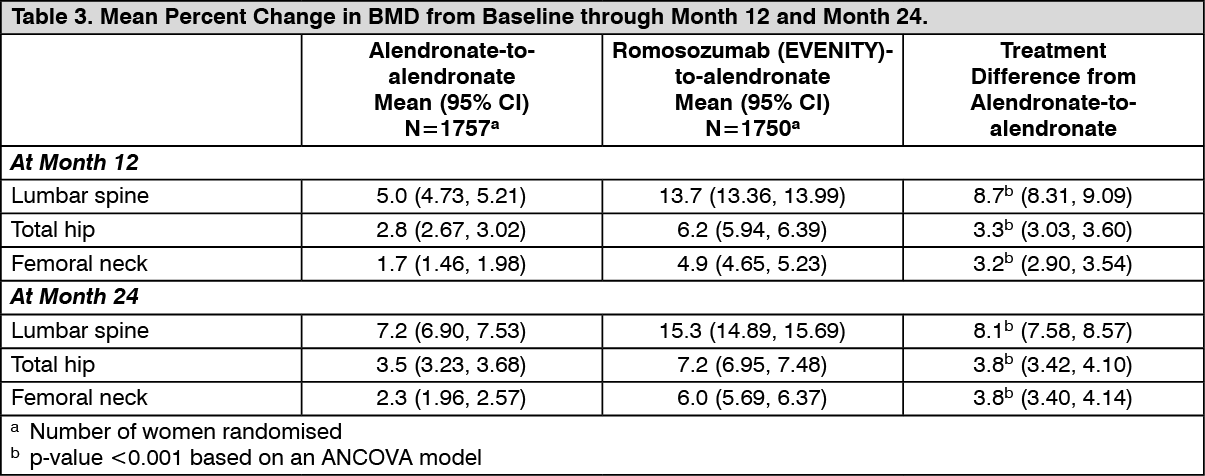
Effect on bone mineral density (BMD): In postmenopausal women with osteoporosis, romosozumab (EVENITY) significantly increased BMD at the lumbar spine, total hip, and femoral neck compared with alendronate at month 12. At month 24, romosozumab (EVENITY) for 12 months followed by alendronate for 12 months, significantly increased BMD compared with alendronate alone at the lumbar spine, total hip, and femoral neck.
Consistent effects on BMD were observed regardless of baseline age, baseline BMD, and geographic region at the lumbar spine and total hip. (See Table 3.)
 Click on icon to see table/diagram/image
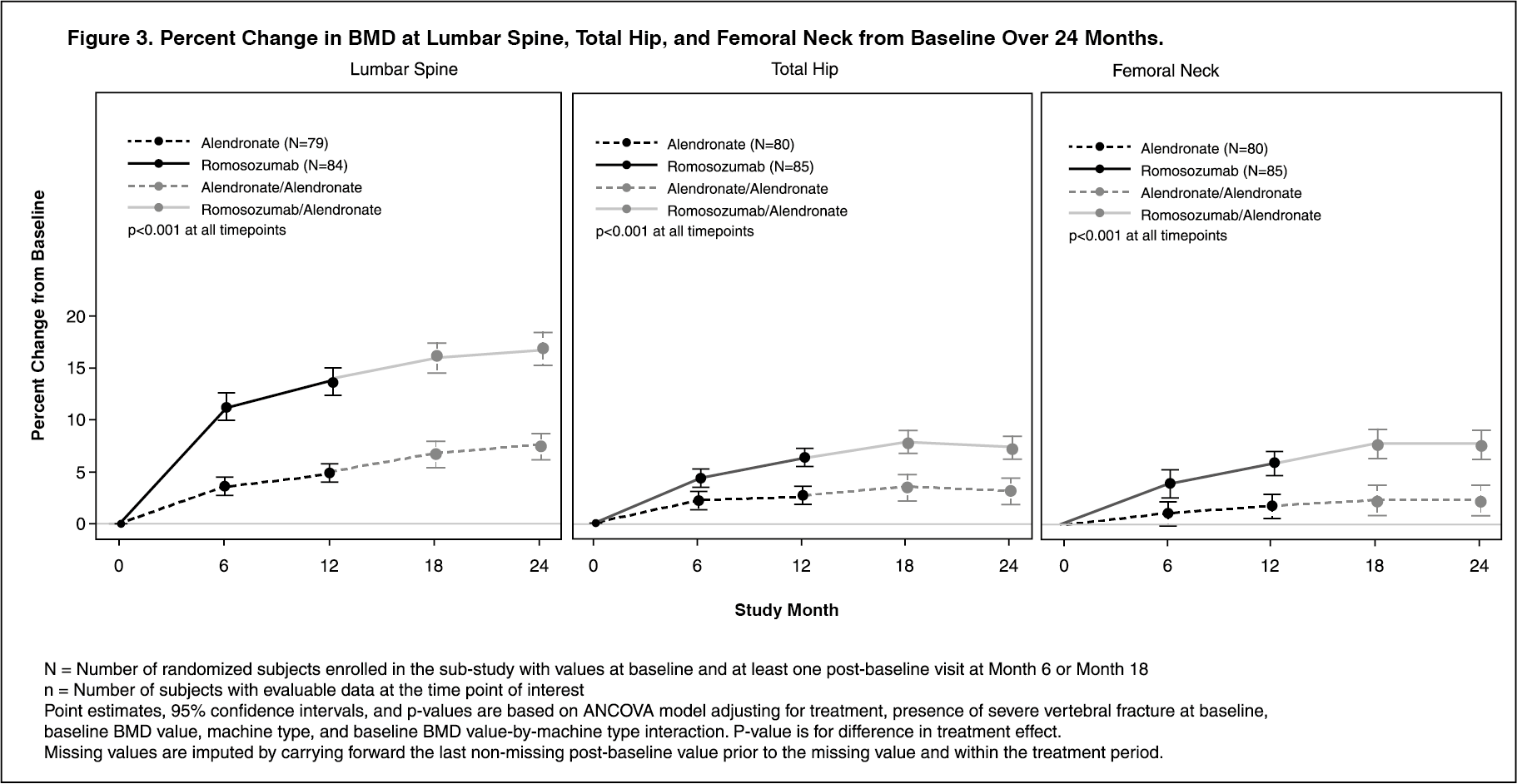
Click on icon to see table/diagram/imageAmong women with BMD assessed at baseline and every 6 months, romosozumab (EVENITY) significantly increased BMD at the lumbar spine, total hip, and femoral neck compared to alendronate alone through month 24. Following the double-blind period, in patients who transitioned from romosozumab (EVENITY) to alendronate and in patients who continued on alendronate, BMD continued to increase through month 24. The differences in BMD achieved at month 12 between patients who initially received romosozumab (EVENITY) or alendronate were maintained at month 24 (Figure 3).
Treatment differences in BMD at 6 months were 7.6% at the lumbar spine, 2.2% at the total hip, and 2.9% at the femoral neck. After 12 months, the treatment differences were 8.9% at the lumbar spine, 3.7% at the total hip, and 4.1% at the femoral neck. At 18 months, women who received romosozumab (EVENITY) followed by alendronate maintained gains in BMD compared to women who continued on alendronate, with treatment differences of 9.3% at the lumbar spine, 4.3% at the total hip, and 5.4% at the femoral neck. At 24 months, women who received romosozumab (EVENITY) followed by alendronate maintained gains in BMD compared to women who continued on alendronate, with treatment differences of 9.4% at the lumbar spine, 4.3% at the total hip, and 5.3% at the femoral neck. (See Figure 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageStudy 2 (placebo-controlled): Placebo-controlled Fracture study in postmenopausal women with osteoporosis (FRAME): The efficacy and safety of romosozumab (EVENITY) in the treatment of postmenopausal osteoporosis was demonstrated in a multicentre, multinational, randomised, double-blind, placebo-controlled, parallel-group study of 7180 postmenopausal women aged 55 to 90 years (mean age of 70.9 years), with a mean of 23.0 years since menopause. Prior use of osteoporosis medications was reported in 6.8% of women, with oral bisphosphonates the most frequently reported (4.9%). Enrolled women had a baseline bone mineral density (BMD) T-score at the total hip or femoral neck of ≤-2.50 to >-3.5. The mean baseline lumbar spine, total hip, and femoral neck BMD T-scores were -2.72, -2.47, and -2.75, respectively, and 18.3% of women had a vertebral fracture at baseline. The mean 10-year probabilities of major osteoporotic fractures and hip fractures calculated with femoral neck BMD were 13.2% and 5.7% respectively. Women were randomised to receive subcutaneous injections of either romosozumab (EVENITY) (N=3589) or placebo (N=3591) once every month in a blinded fashion for 12 months. After the 12-month double-blind study period, women in both arms transitioned to open-label denosumab 60 mg subcutaneous every 6 months for 12 months while remaining blinded to initial treatment. Women received at least 500 mg calcium and 600 IU vitamin D supplementation daily and could have received a loading dose of 50,000 to 60,000 IU of vitamin D after randomisation. Eighty-nine percent of randomised women completed the 12-month double-blind period and 83.9% completed the 24-month study period.
The co-primary efficacy endpoints were the incidence of new vertebral fractures through month 12 and through month 24. Vertebral fractures were diagnosed based on lateral spine radiographs (T4-L4) using a semi-quantitative scoring method. Secondary efficacy endpoints included the incidence of clinical fractures (all symptomatic fractures including nonvertebral and painful vertebral fractures), nonvertebral fractures, new or worsening vertebral fractures, major nonvertebral fractures, hip fractures, and percent change from baseline in BMD at the lumbar spine, total hip, and femoral neck, and were evaluated through 24 months.
Subgroup analyses of the primary endpoints indicated that the efficacy of romosozumab was consistent regardless of baseline characteristics examined, including age, race, geographic region, baseline lumbar spine BMD T-score, baseline total hip/femoral neck BMD T-score, baseline BMI, fracture history, and FRAX score.
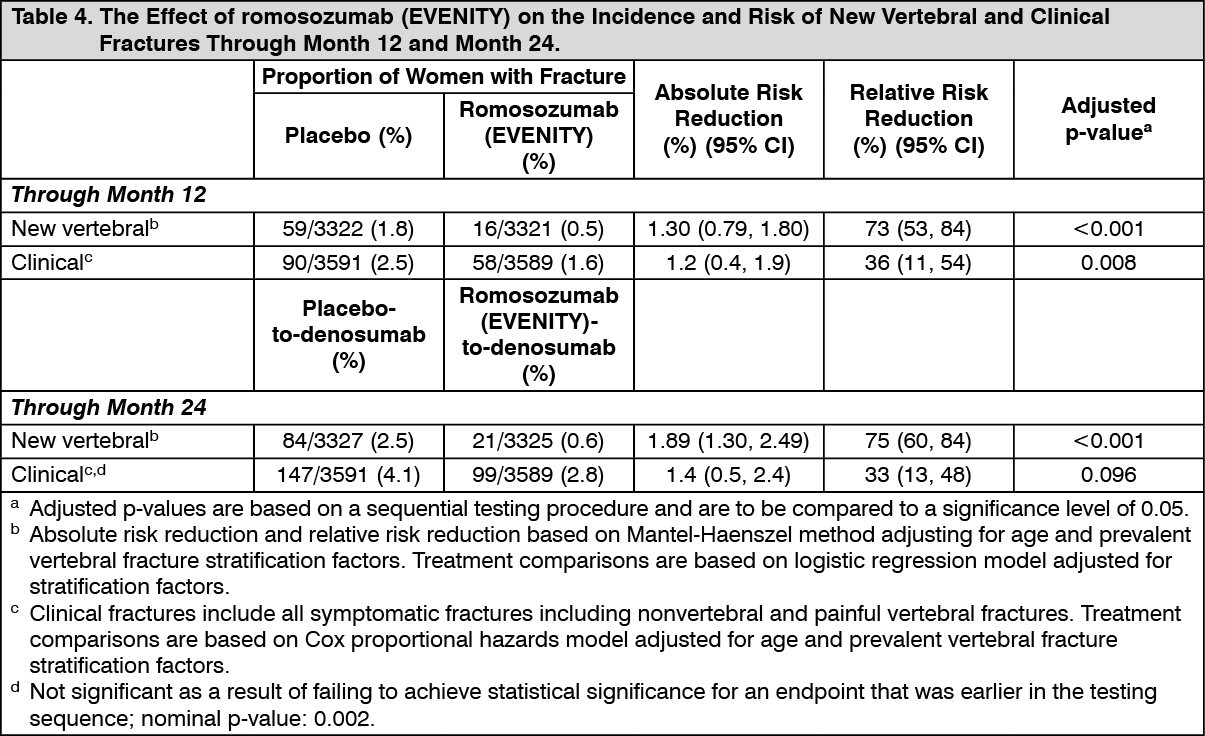
Effect on new vertebral and clinical fractures: Romosozumab (EVENITY) reduced the incidence of new vertebral fractures by 73% (adjusted p-value <0.001) through month 12, as shown in Table 4. Additionally, in those women who received romosozumab (EVENITY) during the first year, the reduction in fracture risk persisted through the second year in women who transitioned from romosozumab (EVENITY) to denosumab compared to those who transitioned from placebo to denosumab (month 24; p <0.001). Romosozumab (EVENITY) reduced the risk of new vertebral fracture by 75% (adjusted p-value <0.001) through month 24.
Romosozumab (EVENITY) also reduced the incidence of clinical fractures by 36% (p-value=0.008) through month 12 and by 33% (adjusted p-value=0.096) through month 24 (see Table 4 and Figure 4 for time to first clinical fracture). (See Table 4, Figures 4 and 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image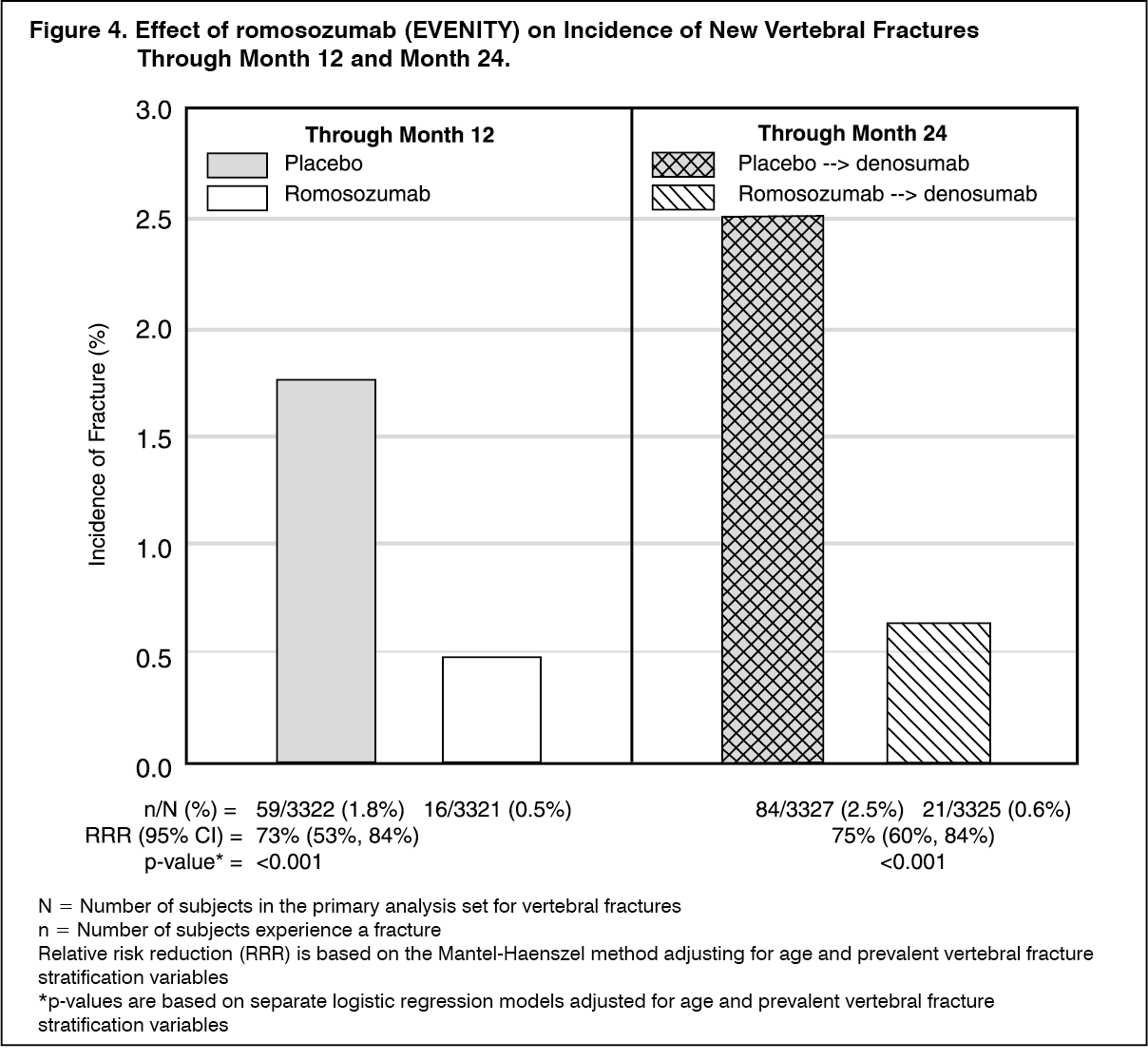 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image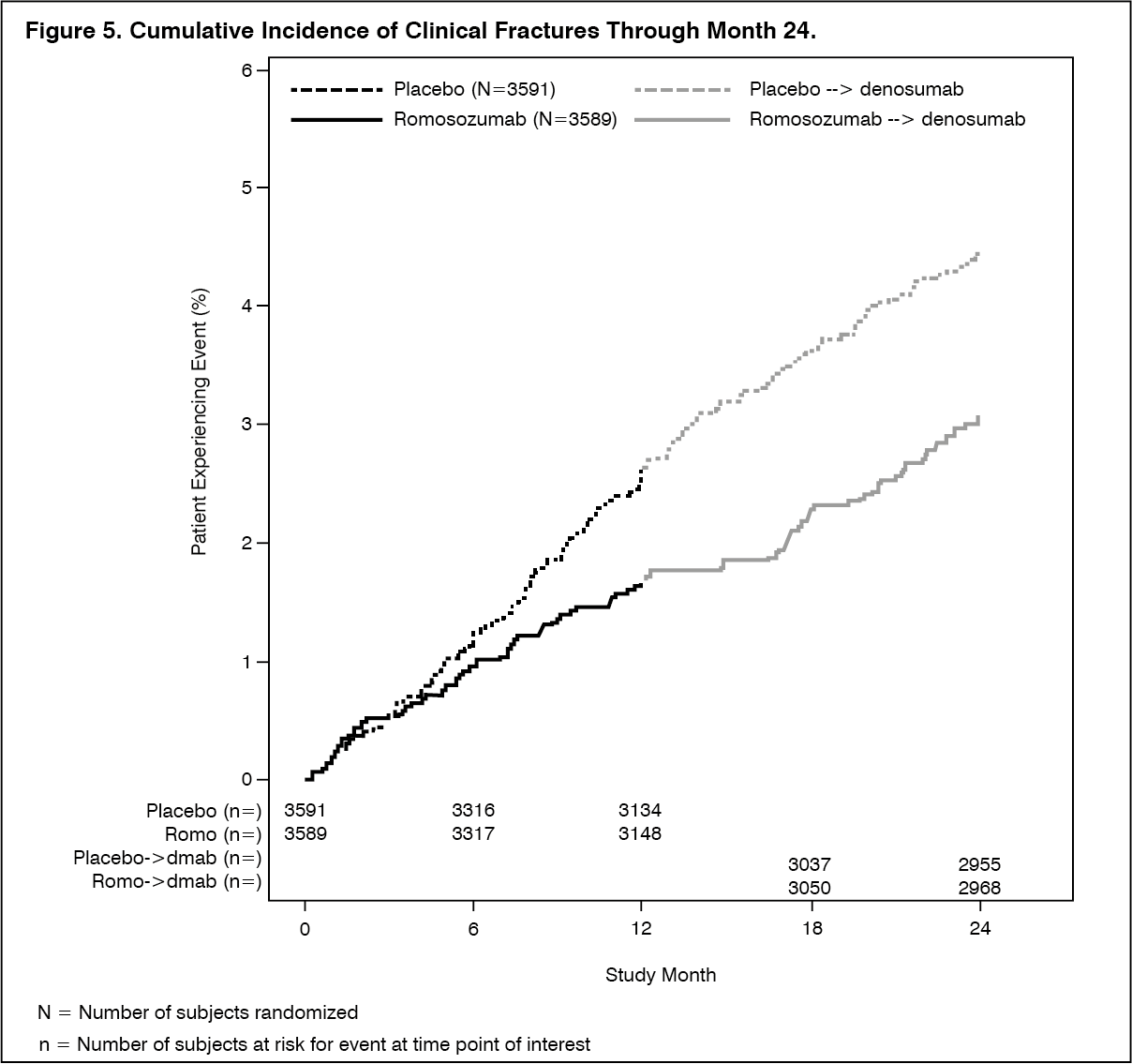 Click on icon to see table/diagram/image
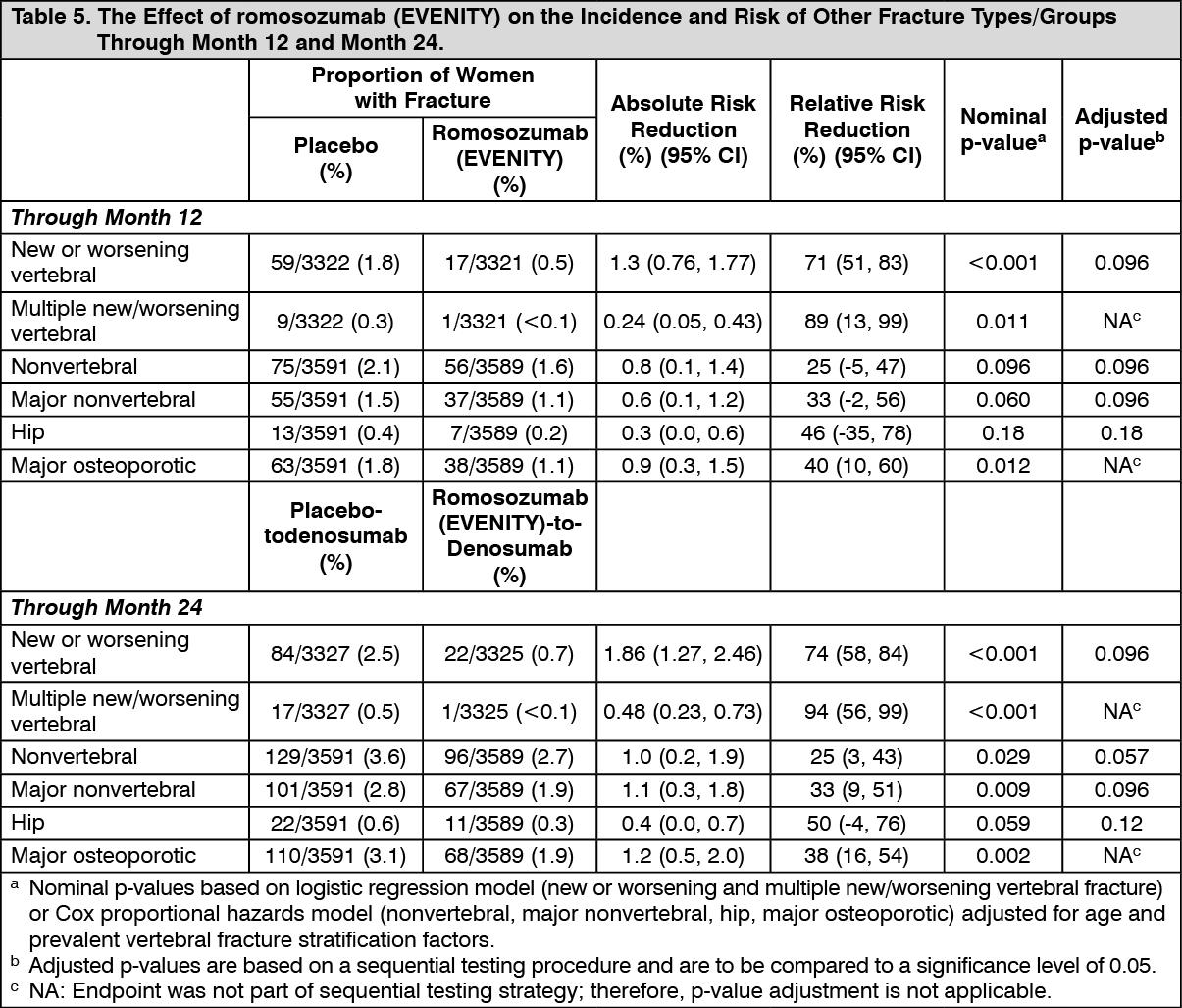
Click on icon to see table/diagram/imageEffect on other fracture types/groups: see Table 5 for effect of romosozumab (EVENITY) on other Fracture Types/Groups through Month 24. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe secondary endpoint of nonvertebral fracture did not reach statistical significance at month 12 (p=0.096) or month 24 (p=0.057) with romosozumab (EVENITY) treatment. Subgroup analysis showed a significant treatment-by-region interaction was noted for the nonvertebral fracture and clinical fracture endpoints through month 12. In Central/Latin America (accounting for 43.0% of the randomised population in Study 20070337), the nonvertebral fracture rate observed in the placebo group in the first 12 months was low (1.2%), with no reduction seen with romosozumab treatment (1.5%). In addition, lower FRAX 10-year probabilities of major osteoporotic and hip fracture in Central/Latin America reflected a population with a lower than expected fracture risk, despite low baseline BMD T-scores. In the rest-of-world population, the nonvertebral fracture rate was 2.7% in the placebo group and 1.6% in the romosozumab group (relative risk reduction 42% [95% CI: 11, 63], nominal p=0.012).
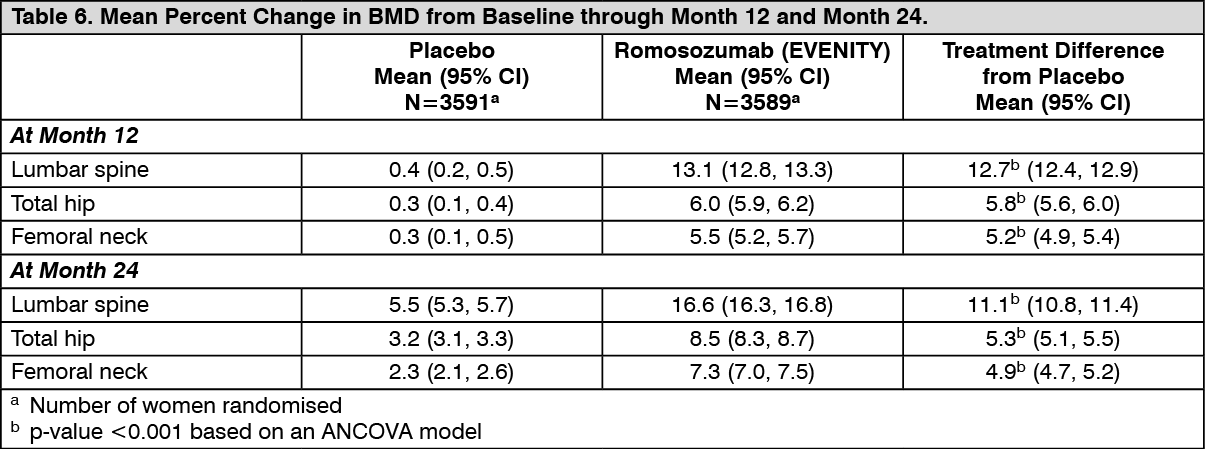
Effect on bone mineral density (BMD): In postmenopausal women with osteoporosis, romosozumab (EVENITY) significantly increased BMD at the lumbar spine, total hip, and femoral neck relative to placebo at month 12. Following 12 months of treatment, romosozumab (EVENITY) increased BMD at the lumbar spine from baseline in 99% of postmenopausal women. Ninety-two percent of women treated with romosozumab (EVENITY) achieved at least a 5% increase from baseline in BMD at lumbar spine by month 12 and 68% gained 10% or more. These effects were sustained with transition to another osteoporosis treatment; women who received romosozumab (EVENITY) followed by denosumab had greater increases in BMD at the lumbar spine, total hip, and femoral neck at month 24 compared to women who received placebo followed by denosumab (Table 6). Consistent effects on BMD were observed regardless of baseline age, baseline BMD, and geographic region at the lumbar spine and total hip. (See Table 6.)
 Click on icon to see table/diagram/image
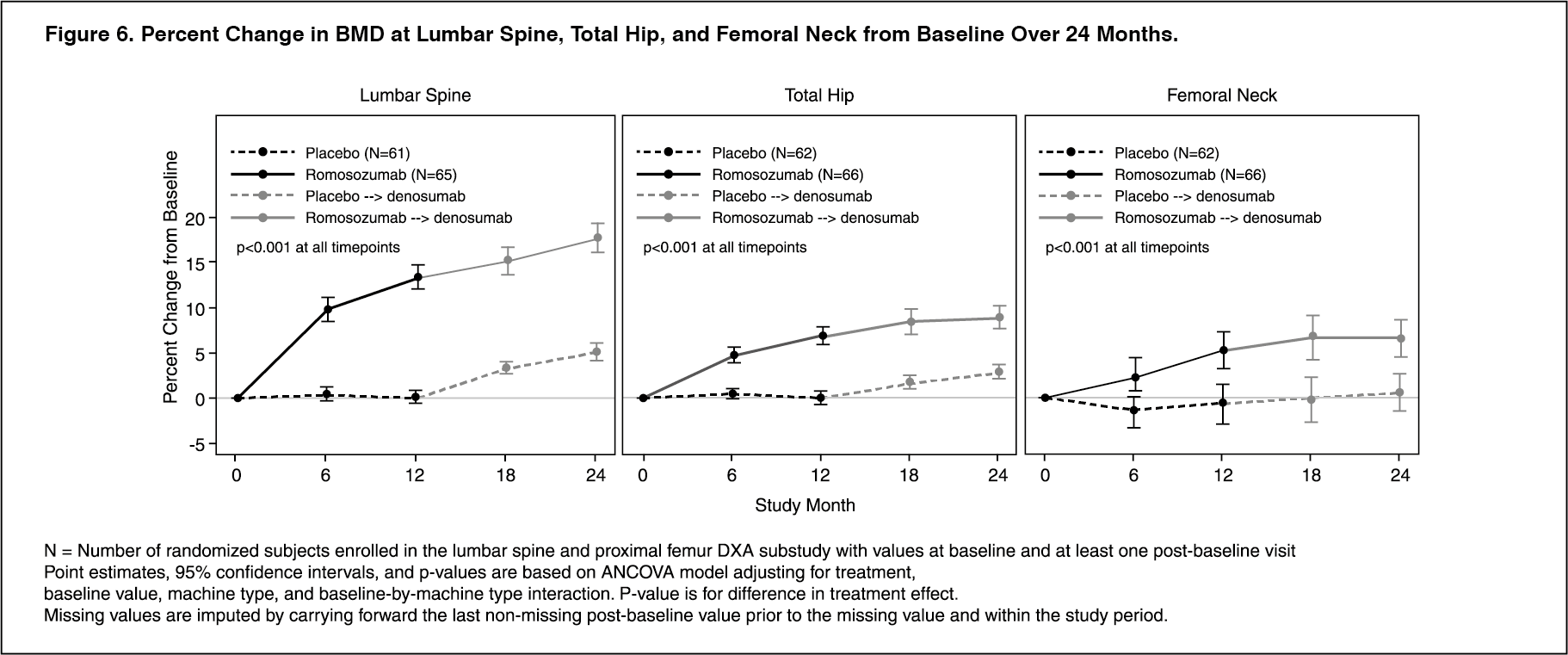
Click on icon to see table/diagram/imageAmong women with BMD assessed at baseline and every 6 months, romosozumab (EVENITY) significantly increased BMD at the lumbar spine, total hip, and femoral neck relative to placebo at 6 and 12 months. Following the transition from romosozumab (EVENITY) to denosumab, BMD continued to increase through month 24. In patients who transitioned from placebo to denosumab, BMD also increased with denosumab use. The differences in BMD achieved at month 12 between romosozumab (EVENITY) and placebo patients were overall maintained at month 24, when comparing patients who transitioned from romosozumab (EVENITY) to denosumab versus patients who transitioned from placebo-to-denosumab (Figure 6). Subgroup analyses of the primary endpoints indicated that the efficacy of romosozumab was consistent regardless of baseline characteristics examined.
Treatment differences in BMD at 6 months were 9.4% at the lumbar spine, 4.3% at the total hip, and 3.6% at the femoral neck. After 12 months, the treatment differences were 13.3% at the lumbar spine, 6.9% at the total hip, and 5.9% at the femoral neck (all p <0.001). At 18 months, women who received romosozumab (EVENITY) followed by denosumab maintained gains in BMD compared to women who received placebo followed by denosumab, with treatment differences of 11.8% at the lumbar spine, 6.8% at the total hip, and 6.8% at the femoral neck. At 24 months, women who received romosozumab (EVENITY) followed by denosumab maintained gains in BMD compared to women who received placebo followed by denosumab, with treatment differences of 12.6% at the lumbar spine, 6.0% at the total hip, and 6.0% at the femoral neck (all p <0.001). (See Figure 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBone histology and histomorphometry: A total of 154 transiliac crest bone biopsy specimens were obtained from 139 postmenopausal women with osteoporosis at month 2, month 12, and/or month 24. Of the biopsies obtained, 154 (100.0%) were adequate for qualitative histology and 138 (89.6%) were adequate for full quantitative histomorphometry assessment. Qualitative histology assessments from those treated with romosozumab (EVENITY) showed normal bone architecture and quality at all time points. There was no evidence of woven bone, mineralisation defects, or marrow fibrosis.
Histomorphometry assessments on biopsies at months 2 and 12 compared the effect of romosozumab (EVENITY) with placebo (15 specimens at month 2 and 39 specimens at month 12 in the romosozumab (EVENITY) group, 14 specimens at month 2 and 31 specimens at month 12 in the placebo group). In women treated with romosozumab (EVENITY), histomorphometric indices of bone formation were increased and bone resorption were decreased at month 2. At month 12, both bone formation and resorption indices were decreased with romosozumab (EVENITY), while bone volume and trabecular thickness were increased. Biopsies obtained at month 24 compared the effect of romosozumab (EVENITY) for 12 months followed by denosumab for 12 months (18 specimens) with placebo followed by denosumab (21 specimens). At month 24, indices of bone remodelling were low and similar in both groups, consistent with the effects of denosumab.
Study 3 Women transitioning from bisphosphonate therapy: Study evaluating effect of Romosozumab Compared with Teriparatide in postmenopausal women with osteoporosis at high risk for fracture previously treated with bisphosphonate therapy (STRUCTURE): The safety and efficacy of romosozumab (EVENITY) in postmenopausal women with osteoporosis transitioning from bisphosphonate therapy were evaluated in a multicentre, randomised, open-label study of 436 postmenopausal women aged 56 to 90 years (mean age of 71.5 years). All subjects received oral bisphosphonate therapy in the 3 years immediately prior to screening; the median duration of prior bisphosphonate use was 6.2 years (range: 3 to 27 years). This study evaluated safety and BMD changes by dual-energy X-ray absorptiometry (DXA) through 12 months of treatment with romosozumab (EVENITY) compared with 12 months of treatment with teriparatide. The study also evaluated hip strength estimated by finite element analysis (FEA) over 12 months using quantitative computed tomography images.
Enrolled women were required to have a baseline BMD T-score at the lumbar spine, total hip, or femoral neck of ≤-2.50 and any history of nonvertebral fracture after age 50 or vertebral fracture at any time. The mean baseline lumbar spine, total hip, and femoral neck BMD T-scores were -2.85, -2.24, and -2.46, respectively. At month 12, romosozumab (EVENITY) increased BMD from baseline by 9.8% (95% CI: 9.0, 10.5) at the lumbar spine, 2.9% (95% CI: 2.5, 3.4) at the total hip, and 3.2% (95% CI: 2.6, 3.8) at the femoral neck. Treatment differences in BMD at 12 months compared to teriparatide were 4.4% (95% CI: 3.4, 5.4) at the lumbar spine, 3.4% (95% CI: 2.8, 4.0) at the total hip, and 3.4% at the femoral neck (95% CI: 2.6, 4.2; p-value <0.0001 for all comparisons).
At month 12, romosozumab (EVENITY) increased estimated strength from baseline by 2.5% (95% CI: 1.7, 3.2) using finite element analysis (FEA) at the total hip. The treatment difference in estimated strength at the total hip at month 12 compared to teriparatide was 3.2% (95% CI: 2.1, 4.3; p-value <0.0001).
Adverse reactions observed in this study were generally consistent with those seen in women not transitioning from bisphosphonate therapy (see Pharmacology: Pharmacodynamics: Women transitioning from bisphosphonate therapy from previous text).
Treatment of osteoporosis in men: Study 4: A placebo-controlled study evaluating the efficacy and safety of romosozumab in treating men with osteoporosis (BRIDGE): The efficacy and safety of romosozumab (EVENITY) in men with osteoporosis was demonstrated in a 12-month, multicentre, randomised, double-blind, placebo-controlled study of 245 men aged 55 to 89 years (mean age of 72.1 years). The majority of men did not report previous use of osteoporosis medications before enrolment into the study. Use of calcitrol (1,25 dihydroxy vitamin D) was the most frequently reported (romosozumab vs placebo: 3.1% vs 2.4%), followed by denosumab (1.8% vs 3.7%) and oral bisphosphonates (0.6% vs 6.1%). Enrolled men had a baseline BMD T-score of ≤-2.50 at the lumbar spine, total hip, or femoral neck. Men with a BMD T-score of ≤-1.50 at the lumbar spine, total hip, or femoral neck were enrolled if there was a history of fragility fracture. Men with BMD T-score at the total hip or femoral neck of ≤-3.5 were excluded from this study. The mean baseline lumbar spine, total hip, and femoral neck BMD T-scores were -2.26, -1.92, and -2.33, respectively. For the total subject population, the mean 10-year probabilities of major osteoporotic fractures and of hip fractures, respectively, (calculated with BMD) were 8.9% and 3.9%. Men were randomised 2:1 to receive SC injections of either romosozumab (EVENITY) (n=163) or placebo (n=82) once every month. All men received at least 500 mg calcium and at least 600 IU vitamin D supplementation daily and could have received a loading dose of 50,000 to 60,000 IU of vitamin D after randomisation. Ninety-four percent of randomised men completed the 12-month double-blind study.
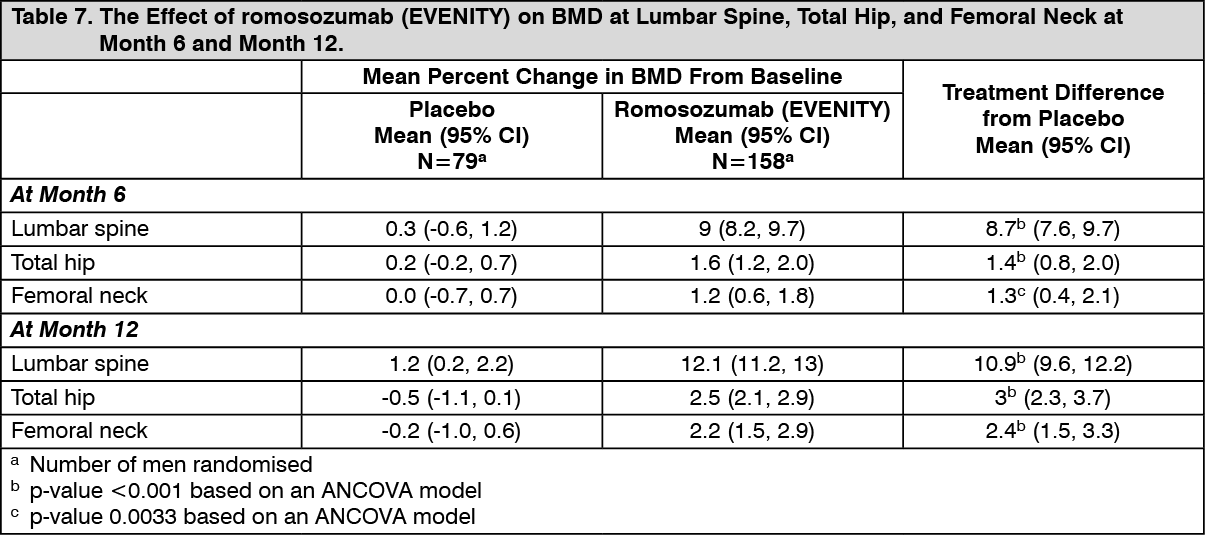
Effect on bone mineral density (BMD): The primary efficacy variable was percent change in lumbar spine BMD from baseline at month 12. Secondary efficacy variables included percent change in total hip and femoral neck BMD from baseline to month 12 and percent change in lumbar spine, total hip, and femoral neck BMD from baseline to month 6.
In men with osteoporosis, treatment with romosozumab (EVENITY) significantly increased BMD at month 12. The treatment differences in BMD at 6 months were 8.7% at the lumbar spine, 1.4% at the total hip, and 1.3% at femoral neck. At 12 months, the treatment differences were 10.9% at the lumbar spine, 3% at the total hip, and 2.4% at the femoral neck (Table 7).
Consistent effects on BMD were observed regardless of baseline age, baseline BMD, geographic region, and history of vertebral fracture. (See Table 7 and Figure 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image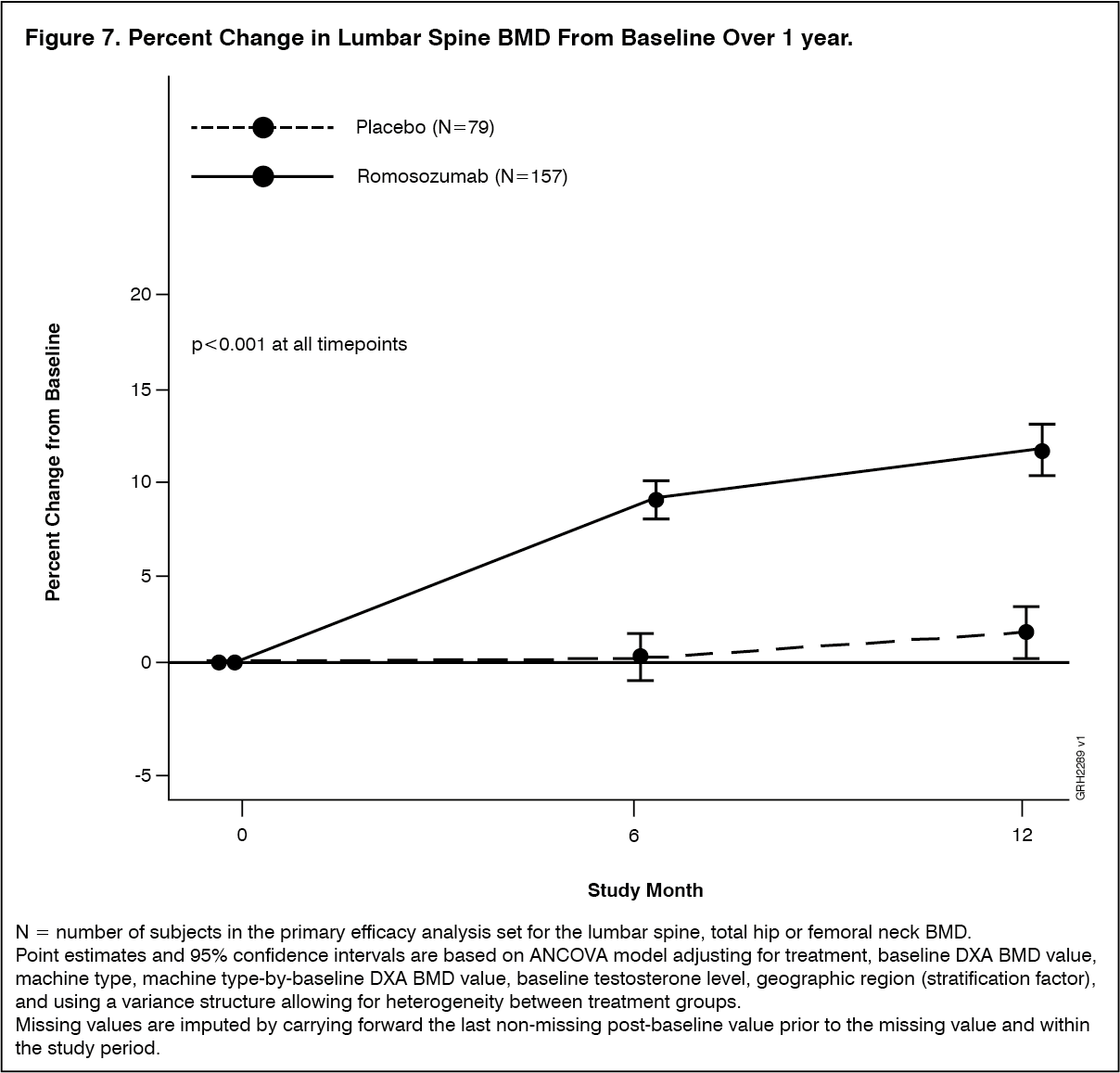 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBone histology and histomorphometry: A total of 20 transiliac crest bone biopsy specimens were obtained from men with osteoporosis at 12 months (11 specimens in romosozumab (EVENITY) group, 9 specimens in placebo group). Of the biopsies obtained, all were adequate for qualitative histology. All biopsies from placebo patients and 9 (81.8%) of biopsies from romosozumab (EVENITY) patients were adequate for full quantitative histomorphometry assessment. Qualitative histology assessments showed normal lamellar bone with no evidence of mineralisation defects, woven bone, marrow fibrosis, or clinically significant marrow abnormality in patients treated with romosozumab (EVENITY). The presence of double-labelled surface, as evidence of active bone formation, was observed in the trabecular or cortical compartments for 88.9% (8/9) of patients in the romosozumab (EVENITY) group and 77.8% (7/9) patients in the placebo group. In cancellous bone, histomorphometric analyses at month 12 revealed decreases in bone resorption parameters (percent eroded and osteoclastic surfaces) in the romosozumab (EVENITY) group with no significant difference noted in bone formation and bone structure parameters compared with the placebo group.
Pharmacokinetics: Romosozumab exhibited nonlinear pharmacokinetics across the SC dose range of 0.1 to 10 mg/kg. Exposure increased greater than dose proportionally (e.g., 550-fold increase in mean AUC from time 0 to infinity [AUCinf] for the 100-fold increase in SC dose from 0.1 to 10 mg/kg). Dose-proportional increases in exposure were observed for the doses of 140 mg and higher.
Absorption: Administration of a single dose of 210 mg romosozumab in healthy male and female volunteers (n=90, age range: 21 to 65 years) resulted in a mean (standard deviation [SD]) maximum serum concentration (Cmax) of 22.2 (5.8) μg/mL and a mean area under the concentration-time curve (AUC) of 389 (127) μg/day/mL. The median time to maximum romosozumab concentration (Tmax) was 5 days (range: 2 to 7 days). Steady-state concentrations were achieved by month 3 following the monthly administration of 210 mg to postmenopausal women. Trough serum romosozumab mean concentration values from samples collected prior to dosing at months 3, 6, 9, and 12 ranged from 8050 to 9780 ng/mL.
For a 210 mg SC dose of romosozumab the bioavailability was estimated to be 81%.
Distribution: The population PK analysis estimated volume of distribution at steady-state was approximately 3.92 L.
Metabolism: The metabolic pathway of romosozumab has not been characterised.
Excretion: The clearance of romosozumab decreased as dose increased. Mean systemic clearance (CL/F) of romosozumab (EVENITY) was estimated to be 0.383 mL/hr/kg, following a single SC administration of 3 mg/kg. The mean effective half-life was 12.8 days after 3 doses of Q4W 3 mg/kg.
Intrinsic factors: Based on a population pharmacokinetic analysis, no notable difference in pharmacokinetics with age (20-89 years), gender, race, or disease state (low bone mass or osteoporosis) was shown. The exposure of romosozumab decreased with increasing body weight.
Development of anti-romosozumab antibodies was associated with reduced serum romosozumab concentrations. In two Phase 2 dose finding studies and the pivotal Phase 3 study, the presence of binding anti-romosozumab antibodies led to a decrease in romosozumab exposure up to 25% at months 3, 6, and 9. The exposures became comparable (approximate 10% difference in mean values) at month 12 between anti-romosozumab antibody-positive and ADA negative subjects (see Immunogenicity under Adverse Reactions).
Special populations: Gender: The pharmacokinetics of romosozumab (EVENITY) were similar in postmenopausal women and in men with osteoporosis.
Renal impairment: Following a single 210 mg dose of romosozumab in a clinical study of 16 patients with severe renal impairment (eGFR 15 to 29 mL/min/1.73 m2) or end-stage renal disease (ESRD) requiring haemodialysis, mean Cmax and AUC were 29% and 44% higher in patients with severe renal impairment as compared to healthy subjects. Mean romosozumab exposure was similar between patients with ESRD requiring haemodialysis and healthy subjects.
A population pharmacokinetic analysis indicated an increase in romosozumab exposure with increasing severity of renal impairment. However, based on both the renal impairment study and population PK analysis, this increase is not clinically meaningful and no dose adjustment is necessary in these patients (see Use in renal impairment under Precautions).
Toxicology: Preclinical safety data: Genotoxicity: No genotoxicity studies have been conducted. As a monoclonal, antibody, romosozumab is not expected to interact with DNA or other chromosomal material.
Carcinogenicity: Romosozumab did not increase tumour incidence in a carcinogenicity study in rats, involving subcutaneous administration at doses up to 50 mg/kg/week for up to 91 (males) or 98 weeks (females). These doses resulted in systemic exposures that were up to 19 times higher than the systemic exposure observed in humans following a monthly subcutaneous dose of 210 mg romosozumab (based on comparison of serum AUC).