One milliliter solution for intravitreal injection contains 40 mg aflibercept.
Each vial provides a usable amount to deliver a single dose of 50 microliters containing 2 mg aflibercept.
The solution has a pH of 6.2.
Excipients/Inactive Ingredients: Polysorbate 20; Sodium dihydrogen phosphate, monohydrate; Disodium hydrogen phosphate, heptahydrate; Sodium chloride; Sucrose; Water for injection.
Pharmacology: Pharmacodynamics: Mechanism of Action: Aflibercept acts as a soluble decoy receptor that binds VEGF-A and PlGF with higher affinity than their natural receptors, and thereby can inhibit the binding and activation of these cognate VEGF receptors.
Pharmacodynamic Effects: Neovascular (wet) age-related macular degeneration: The ALTAIR study enrolled patients with treatment wet AMD, showing similar outcomes to the VIEW studies using 3 initial monthly Aflibercept (Eylea) 2 mg injections, followed by one injection after 2 months, and then continued with a treat-and-extend regimen with variable treatment intervals (2-week or 4-week adjustments) up to a maximum 16 week interval according to pre-specified criteria. At week 52, there were mean decreases in central retinal thickness (CRT) on OCT of -134.4 and -126.1 microns for the 2-week adjustment group and the 4-week adjustment group, respectively. The proportion of patients without fluid on OCT at week 52 was 68.3% and 69.1% in the 2- and 4-week adjustment groups, respectively.
In patients with polypoidal choroidal vasculopathy (PCV), a subtype of wet AMD, treated with 3 monthly Aflibercept (Eylea) 2 mg injections followed by Aflibercept (Eylea) 2 mg every two months (PLANET study), similar outcomes to the VIEW studies were obtained. At week 52, there were mean decreases in retinal thickness on OCT of -138 microns for Aflibercept (Eylea) 2 mg every two months and -144 microns for Aflibercept (Eylea) 2 mg plus rescue photodynamic therapy (PDT) as indicated.
Clinical efficacy: Neovascular (wet) age-related macular degeneration: ALTAIR was a multicenter, randomized, open-label phase 4 study in 247 patients with treatment naive wet AMD, designed to assess the efficacy and safety of Aflibercept (Eylea) following two different adjustment intervals (2 weeks and 4 weeks) of a treat-and-extend dosing regimen.
All patients received 3 monthly doses of Aflibercept (Eylea) 2 mg, followed by one injection after a 2 month interval. At week 16, patients were randomized 1:1 into two treatment groups: 1) Aflibercept (Eylea) treat-and-extend with 2-week adjustments and 2) Aflibercept (Eylea) treat-and-extend with 4-week adjustments. Extension or shortening of the interval was decided based on visual and/or anatomic criteria defined by protocol with a maximum treatment interval of 16 weeks for both groups.
The primary efficacy endpoint was mean change in BCVA from baseline to week 52. The secondary efficacy endpoints were the proportion of patients who did not lose ≥15 letters and the proportion of patients who gained at least 15 letters of BCVA from baseline to week 52.
At week 52, patients in the treat-and-extend arm with 2-week adjustments gained a mean of 9.0 letters from baseline as compared to 8.4 letters for those in the 4-week adjustment group [LS mean difference in letters (95% CI): -0.4 (-3.8,3.0), ANCOVA]. The proportion of patients who did not lose ≥15 letters in the two treatment arms was similar (96.7% in the 2-week and 95.9% in the 4-week adjustment group). The proportion of patients who gained ≥15 letters at week 52 was 32.5% in the 2-week adjustment group and 30.9% in the 4-week adjustment group. The proportion of patients who extended their treatment interval to 12 weeks and beyond was 42.3% in the 2-week adjustment group and 49.6 % in the 4-week adjustment group. Furthermore, in the 4-week adjustment group 40.7% of patients were extended to 16 week intervals. At the last visit prior to week 52, 56.7% and 57.8% of patients in the 2-week and 4-week adjustment groups, respectively had their next injection scheduled at an interval of 12 weeks or more. Ocular and systemic safety profiles were similar to the safety observed in the pivotal studies VIEW1 and VIEW2.
A randomized, double-masked, multi-center, sham-controlled phase IIIb/IV study (PLANET) of Aflibercept (Eylea) monotherapy vs. Aflibercept (Eylea) plus rescue photodynamic therapy (PDT) was conducted in 333 treatment naive patients with symptomatic macular polypoidal choroidal vasculopathy (PCV), a subtype of wet AMD, as diagnosed by indocyanine green angiography (ICGA). All patients received 3 monthly doses of Aflibercept (Eylea) 2 mg and were thereafter randomized 1:1 into two treatment groups: 1) Aflibercept (Eylea) 2 mg plus sham PDT (n=157) or 2) Aflibercept (Eylea) 2 mg plus active PDT (n=161). PDT was given only if rescue criteria were met. Patients in both groups received one Aflibercept (Eylea) 2 mg injection every two months. Patients who qualified for rescue therapy received monthly injections of Aflibercept (Eylea) 2 mg plus active or sham PDT. When visual and anatomic outcomes allowed, treatment intervals were gradually extended to two months in rescue patients. Qualification for rescue therapy was based upon insufficient gain of BCVA, evidence of fluid on OCT and evidence of active polyps on ICGA.
The primary efficacy endpoint was mean change in BCVA from baseline to week 52. The secondary efficacy endpoint was the proportion of patients who did not lose ≥15 letters of BCVA from baseline to week 52.
At week 52, patients on Aflibercept (Eylea) plus sham PDT gained a mean of 10.7 letters from baseline as compared to 10.8 letters in the Aflibercept (Eylea) plus active PDT patients in the full analysis set [LS mean difference in letters (95% CI): -0.7 (-2.9,1.6), ANCOVA]. The proportion of patients who did not lose ≥15 letters was 97.5% in Aflibercept (Eylea) plus sham PDT and 96.9% in Aflibercept (Eylea) plus active PDT group [CMH adjusted difference in % (95%CI): 0.6 (-3.1; 4.3)], showing non-inferiority of both treatments for both the primary endpoint (NI margin of 5 letters) and the secondary endpoint (NI margin of 7 percentage points). No evidence of active polyps was noted in 81.7% of patients in the Aflibercept (Eylea) plus sham PDT group and 88.9% of patients in the Aflibercept (Eylea) plus active PDT group. 86.8% of patients did not require rescue therapy throughout the first year. Data obtained from patients who qualified for PDT rescue therapy (n= 42, 13.2%) did not demonstrate additional benefit on BCVA of the combined administration of verteporfin PDT and Aflibercept (Eylea) compared to Aflibercept (Eylea) monotherapy. Ocular and systemic safety profiles were similar to the safety observed in the pivotal studies VIEW1 and VIEW2.
Diabetic Macular Edema: An independent comparative trial (DRCR.net Protocol T) utilised a dosing regimen based on strict OCT and vision re-treatment criteria. In the aflibercept treatment group (n=224) at week 52, this treatment regimen resulted in patients receiving a mean of 9.2 injections, which is similar to the administered number of doses in the Aflibercept (Eylea) 2Q8 group in VIVIDDME and VISTADME, while overall efficacy of the aflibercept treatment group in Protocol T was comparable to Aflibercept (Eylea) 2Q8 group in VIVIDDME and VISTADME. A 13.3 mean letter gain with 42% of patients gaining at least 15 letters in vision from baseline was observed in Protocol T. Ocular and systemic safety profiles (including ATEs) were similar to VIVIDDME and VISTADME.
Pharmacokinetics: Aflibercept (Eylea) is administered directly into the vitreous to exert local effects in the eye.
Absorption/Distribution: Aflibercept is slowly absorbed from the eye into the systemic circulation after intravitreal administration and is predominately observed in the systemic circulation as an inactive, stable complex with VEGF; however only "free aflibercept" is able to bind endogenous VEGF.
In a pharmacokinetic sub-study with frequent sampling in AMD patients, maximum plasma concentrations of free aflibercept (systemic Cmax) were low, with a mean of approximately 0.02 microgram/mL (range: 0 to 0.054 microgram/mL) within 1 to 3 days after a 2-mg intravitreal injection, and were undetectable two weeks following dosage in almost all patients. Aflibercept does not accumulate in the plasma when administered intravitreally every 4 weeks.
It is estimated that after intravitreal administration of 2 mg to patients, the mean maximum plasma concentration of free aflibercept is more than a 100 fold lower than the concentration of aflibercept required to half-maximally bind systemic VEGF (2.91 microgram/mL) in a study of healthy volunteers. Therefore, systemic pharmacodynamic effects such as blood pressure changes are unlikely.
These pharmacokinetic results were confirmed in a pharmacokinetic sub-study in patients with CRVO (mean Cmax of free aflibercept in plasma 0.046 microgram/mL (range: 0 to 0.081 microgram/mL); undetectable concentrations reached within 1 week).
Elimination: Free aflibercept binds VEGF to form a stable, inert complex. As with other large proteins, both free and bound aflibercept are expected to be cleared by proteolytic catabolism.
Toxicology: Preclinical safety data: Effects in non-clinical studies on repeated dose toxicity were observed only at systemic exposures considered substantially in excess of the maximum human exposure after intravitreal administration at the intended clinical dose indicating little relevance to clinical use.
No studies have been conducted on the mutagenic or carcinogenic potential of aflibercept.
An effect of aflibercept on intrauterine development was shown in embryo-fetal development studies in pregnant rabbits with intravenous (3 to 60 mg/kg) as well as subcutaneous (0.1 to 1 mg/kg) administration. The maternal NOAEL was at the dose of 3 mg/kg or 1 mg/kg, respectively. A developmental NOAEL was not identified. At the 0.1 mg/kg dose, the systemic exposures based on Cmax and cumulative AUC for free aflibercept were approximately 17- and 10-fold higher, respectively, when compared to corresponding values observed in humans after an intravitreal dose of 2 mg.
Aflibercept (Eylea) is indicated for the treatment of: neovascular (wet) age-related macular degeneration (wet AMD), macular edema secondary to central retinal vein occlusion (CRVO), macular edema secondary to branch retinal vein occlusion (BRVO), diabetic macular edema (DME), myopic choroidal neovascularization (myopic CNV).
Aflibercept (Eylea) is for intravitreal injection.
It must only be administered by a qualified physician experienced in administering intravitreal injections.
Dosage regimen: Neovascular (wet) age-related macular degeneration (wet AMD): The recommended dose for Aflibercept (Eylea) is 2 mg (equivalent to 50 microliters).
Aflibercept (Eylea) treatment is initiated with one injection per month for three consecutive doses, followed by one injection every 2 months.
Based on the physician's judgement of visual and/or anatomic outcomes the treatment interval may be maintained at two months or further extended using a treat-and-extend dosing regimen, where injection intervals are gradually increased to maintain stable visual and/ or anatomic outcomes. If visual and/or anatomic outcomes deteriorate, the treatment interval should be shortened accordingly.
There is no requirement for monitoring between injections. Based on the physician's judgement the schedule of monitoring visits may be more frequent than the injections visits.
Aflibercept (Eylea) may be dosed as frequently as once per month (4 weeks).
Treatment intervals greater than 4 months (16 weeks) between injections have not been studied (see Pharmacology: Pharmacodynamics: Pharmacodynamic Effects under Actions).
Macular edema secondary to central retinal vein occlusion (CRVO): The recommended dose for Aflibercept (Eylea) is 2 mg (equivalent to 50 microliters).
After the initial injection, treatment is given monthly (every 4 weeks) until visual and/or anatomic outcomes are stable, three or more consecutive, monthly (every 4 weeks) injections may be needed. The interval between two doses should not be shorter than one month (4 weeks).
Treatment should be continued and the interval may be extended based on visual and anatomic outcomes (treat and extend regimen).
Macular edema secondary to branch retinal vein occlusion (BRVO): The recommended dose for Aflibercept (Eylea) is 2 mg (equivalent to 50 microliters).
After the initial injection, treatment is given monthly (every 4 weeks) until visual and/or anatomic outcomes are stable. Three or more consecutive, monthly (every 4 weeks) injections may be needed. The interval between two doses should not be shorter than one month (4 weeks).
Treatment should be continued and the interval may be extended based on visual and/or anatomic outcomes (treat and extend regimen).
Usually, monitoring should be done at the injection visits. During treatment interval extension through to completion of therapy, the monitoring schedule should be determined by the treating physician based on the individual patient's response and may be more frequent than the schedule of injections.
Diabetic macular edema (DME): The recommended dose for Aflibercept (Eylea) is 2 mg (equivalent to 50 microliters) administered by intravitreal injection monthly for the first 5 consecutive doses, followed by one injection every 2 months.
After the first 12 months of treatment with Aflibercept (Eylea), and based on visual and/or anatomic outcomes, the treatment interval may be extended, such as with a treat-and-extend dosing regimen, where the treatment intervals are gradually increased to maintain stable based on visual and/or anatomic outcomes; however there are insufficient data to conclude on the length of these intervals. If visual and/or anatomic outcomes deteriorate, the treatment interval should be shortened accordingly.
The schedule for monitoring should therefore be determined by the treating physician and may be more frequent than the schedule of injections.
If visual and anatomic outcomes indicate that the patient is not benefiting from continued treatment, Aflibercept (Eylea) should be discontinued.
Myopic choroidal neovascularization (myopic CNV): The recommended dose for Aflibercept (Eylea) is a single intravitreal injection of 2 mg (equivalent to 50 microliters).
Additional doses should be administered only if visual and anatomic outcomes indicate that the disease persists.
Additional information on special populations: Patients with hepatic and/or renal impairment: No specific studies in patients with hepatic and/or renal impairment have been conducted with Aflibercept (Eylea).
Available data do not suggest a need for a dose adjustment with Aflibercept (Eylea) in these patients.
Elderly: No special considerations are needed.
Method of administration: Intravitreal injections must be carried out according to medical standards and applicable guidelines by a qualified physician experienced in administering intravitreal injections. In general, adequate anesthesia and asepsis, including topical broad spectrum microbicide (e.g., povidone iodine), have to be ensured. Surgical hand disinfection, sterile gloves, a sterile drape, and a sterile eyelid speculum (or equivalent) are recommended.
Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, sterile equipment for paracentesis should be available.
Following intravitreal injection patients should be instructed to report any symptoms suggestive of endophthalmitis (e.g., eye pain, redness of the eye, photophobia, blurring of vision) without delay.
Each vial should only be used for the treatment of a single eye.
After injection any unused product must be discarded.
In clinical trials doses of up to 4 mg in monthly intervals and isolated cases of overdoses with 8 mg were generally well tolerated.
Overdosing with increased injection volume may increase intraocular pressure. Therefore, in case of an overdose intraocular pressure should be monitored and if deemed necessary by the treating physician, adequate treatment should be initiated.
Known hypersensitivity to aflibercept or to any of the excipients.
Ocular or periocular infection.
Active severe intraocular inflammation.
Endophthalmitis: Intravitreal injections, including those with Aflibercept (Eylea), have been associated with endophthalmitis (see Adverse Reactions). Proper aseptic injection technique must always be used when administering Aflibercept (Eylea).
Patients should be instructed to report any symptoms suggestive of endophthalmitis without delay and should be managed appropriately.
Increase in intraocular pressure: Increases in intraocular pressure have been seen within 60 minutes of an intravitreal injection, including with Aflibercept (Eylea) (see Adverse Reactions). Special precaution is needed in patients with poorly controlled glaucoma. In all cases, both the intraocular pressure and the perfusion of the optic nerve head must therefore be monitored and managed appropriately.
Effects on ability to drive or use machines: Patients may experience temporary visual disturbances after an intravitreal injection with Aflibercept (Eylea) and the associated eye examinations. They should not drive or use machines until visual function has recovered sufficiently.
Pregnancy: There are no data on the use of aflibercept in pregnant women.
Studies in animals have shown reproductive toxicity after systemic administration.
Aflibercept (Eylea) should not be used during pregnancy unless the potential benefit outweighs the potential risk to the fetus.
Women of childbearing potential: Women of childbearing potential have to use effective contraception during treatment and for at least 3 months after the last intravitreal injection of Aflibercept (Eylea).
Lactation: It is unknown whether aflibercept is excreted in human milk. A risk to the breast-fed child cannot be excluded.
Aflibercept (Eylea) is not recommended during breast-feeding. A decision must be made whether to discontinue breast-feeding or to abstain from Aflibercept (Eylea) therapy.
Summary of the safety profile: Serious adverse reactions related to the injection procedure have occurred in less than 1 in 2,400 intravitreal injections with Aflibercept (Eylea) and included endophthalmitis, retinal detachment, cataract traumatic, cataract, vitreous detachment and intraocular pressure increased (see Precautions).
The most frequently observed adverse reactions (in at least 5% of patients treated with Aflibercept (Eylea)) were conjunctival hemorrhage, eye pain, intraocular pressure increased, vitreous detachment, vitreous floaters and cataract.
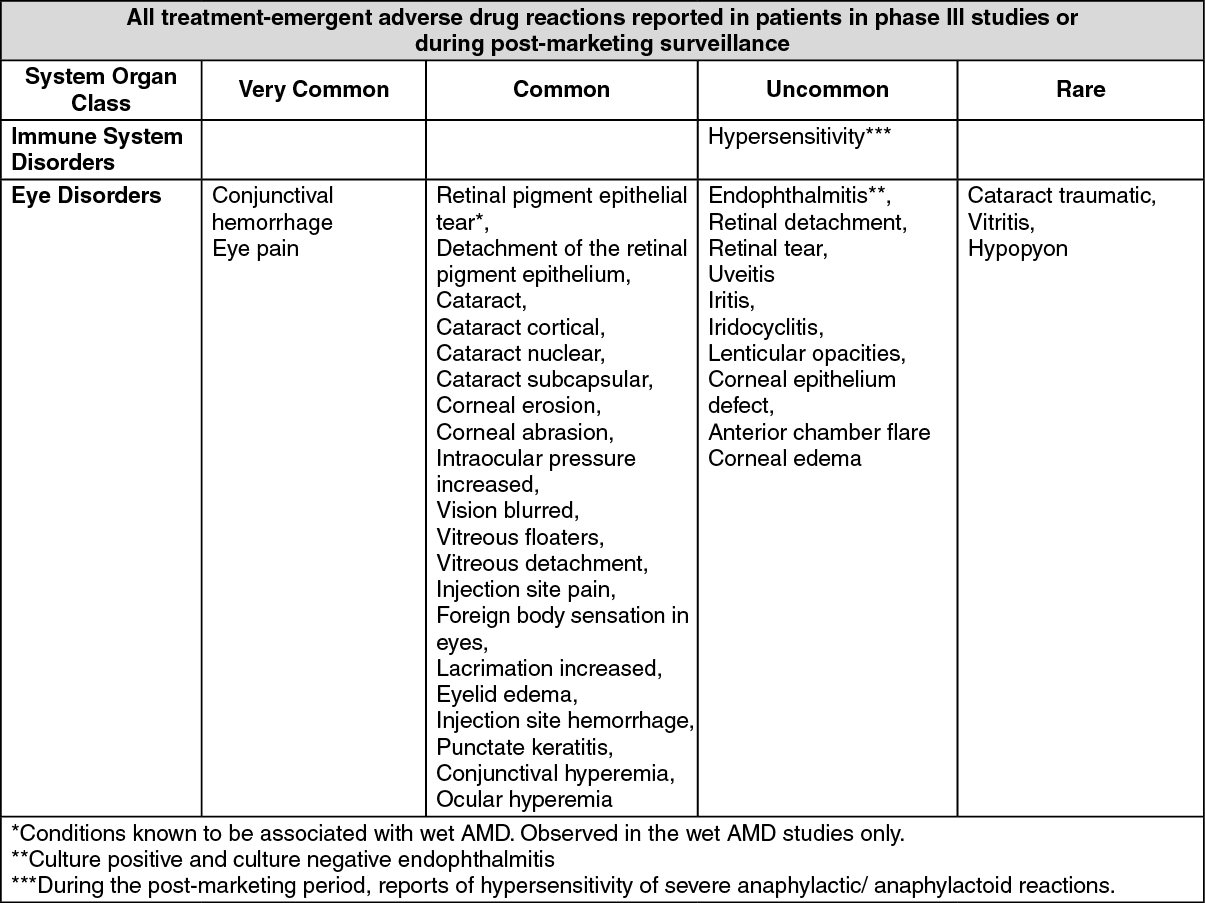
Tabulated list of adverse reactions: The safety data described below include all adverse reactions from eight phase III studies with a reasonable possibility of causality to the injection procedure or medicinal product.
The adverse reactions are listed by system organ class and frequency using the following convention: Very common (≥1/10), common (1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000).
Within each frequency grouping, adverse drug reactions are presented in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions: Arterial thromboembolic events:
Click on icon to see table/diagram/image
Description of selected adverse reactions: Arterial thromboembolic events: Arterial thromboembolic events (ATEs) are adverse events potentially related to systemic VEGF inhibition. There is a theoretical risk of ATEs following intravitreal use of VEGF inhibitors.
Immunogenicity: As with all therapeutic proteins, there is a potential for immunogenicity with Aflibercept (Eylea).
No formal drug interaction studies have been performed with Aflibercept (Eylea).
Incompatibilities: Aflibercept (Eylea) must not be mixed with other medicinal products.
Instructions for use/handling: The vial is for single use in one eye only. Extraction of multiple doses from a single vial or pre-filled syringe may increase the risk of contamination and subsequent infection.
Prior to administration visually inspect the solution for injection. Do not use the vial if particulates, cloudiness, or discoloration are visible.
Prior to usage, the unopened vial of Aflibercept (Eylea) may be stored at room temperature (25°C/77°F) for up to 24 hours. After opening the vial, proceed under aseptic conditions.
For the intravitreal injection, a 30 G x ½ inch injection needle should be used.
Vials: 1. Remove the plastic cap and disinfect the outer part of the rubber stopper of the vial.
2. Attach the 18 G, 5-micron filter needle supplied in the carton to a 1-mL sterile, Luer-lock syringe.
3. Push the filter needle into the center of the vial stopper until the needle is completely inserted into the vial and the tip touches the bottom or bottom edge of the vial.
4. Using aseptic technique withdraw all of the Aflibercept (Eylea) vial contents into the syringe, keeping the vial in an upright position, slightly inclined to ease complete withdrawal. To deter the introduction of air, ensure the bevel of the filter needle is submerged into the liquid. Continue to tilt the vial during withdrawal keeping the bevel of the filter needle submerged in the liquid.
5. Ensure that the plunger rod is drawn sufficiently back when emptying the vial in order to completely empty the filter needle.
6. Remove the filter needle and properly dispose of it.
Note: Filter needle is not to be used for intravitreal injection.
7. Using aseptic technique, firmly twist a 30 G x ½ inch injection needle to the Luer-lock syringe tip.
8. Holding the syringe with the needle pointing up, check the syringe for bubbles. If there are bubbles, gently tap the syringe with finger until the bubbles rise to the top.
9. Eliminate all bubbles and expel excess drug by slowly depressing the plunger so that the plunger tip aligns with the line that marks 0.05 mL on the syringe.
Store in a refrigerator (2°C to 8°C/36°F to 46°F). Do not freeze.
Keep the vial in the outer carton in order to protect from light.
S01LA05 - aflibercept ; Belongs to the class antineovasculatisation agents. Used in the management of neovascular macular degeneration.
Eylea soln for inj 40 mg/mL
2 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
