Infections and Infestations: Infection, viral infection, flu syndrome, otitis media, influenza.
Blood and Lymphatic System Disorders: Thrombocytopenia, leukopenia, pancytopenia, pancytopenia with bone marrow suppression, neutropenia, agranulocytosis, ecchymosis.
Immune System Disorders: Hypersensitivity (including angioedema and anaphylaxis), Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS).
Metabolism and Nutrition Disorders: Anorexia, weight decreased, weight increased, hyponatremia, dehydration.
Psychiatric Disorders: Depression, hostility/aggression, anxiety, insomnia, nervousness/irritability, suicide attempt, suicidal ideation, psychotic disorder, abnormal behavior, hallucination, anger, confusional state, panic attack, affect lability/mood swings, agitation, completed suicide, personality disorder, thinking abnormal, hypersomnia.
Nervous System Disorders: Somnolence, headache, convulsion, balance disorder, dizziness, lethargy, tremor, amnesia, memory impairment, coordination abnormal/ataxia, paresthesia, disturbance in attention, choreoathetosis, dyskinesia, hyperkinesia, ataxia, balance disorder, disturbance in attention, sedation, emotional lability, reflexes increased.
Eye Disorders: Diplopia, vision blurred, amblyopia, conjunctivitis.
Ear and Labyrinth Disorders: Vertigo, ear pain.
Respiratory, Thoracic and Mediastinal Disorders: Cough, chest pain, bronchitis, pharyngitis, rhinitis, sinusitis, asthma, nasal congestion, pharyngolaryngeal pain, nasopharyngitis.
Gastrointestinal Disorders: Abdominal pain, diarrhea, dyspepsia, vomiting, nausea, pancreatitis, gastroenteritis, gingivitis, tooth disorder, constipation.
Hepatobiliary Disorders: Liver function test abnormal, hepatic failure, hepatitis.
Skin and Subcutaneous Tissue Disorders: Rash, alopecia, eczema, pruritus, toxic epidermal necrolysis, Stevens-Johnson syndrome, erythema multiforme, skin discoloration, vesiculobullous rash.
Musculoskeletal and Connective Tissue Disorders: Muscular weakness, myalgia, back pain, neck pain, arthralgia.
Renal and Urinary Disorders: Urinary tract infection, albuminuria, urine abnormality.
General Disorders and Administration Site Conditions: Asthenia/fatigue, fever, pain, face edema.
Investigations: Drug level increased.
Injury, Poisoning and Procedural Complications: Injury, head injury, contusion, fall, joint sprain.


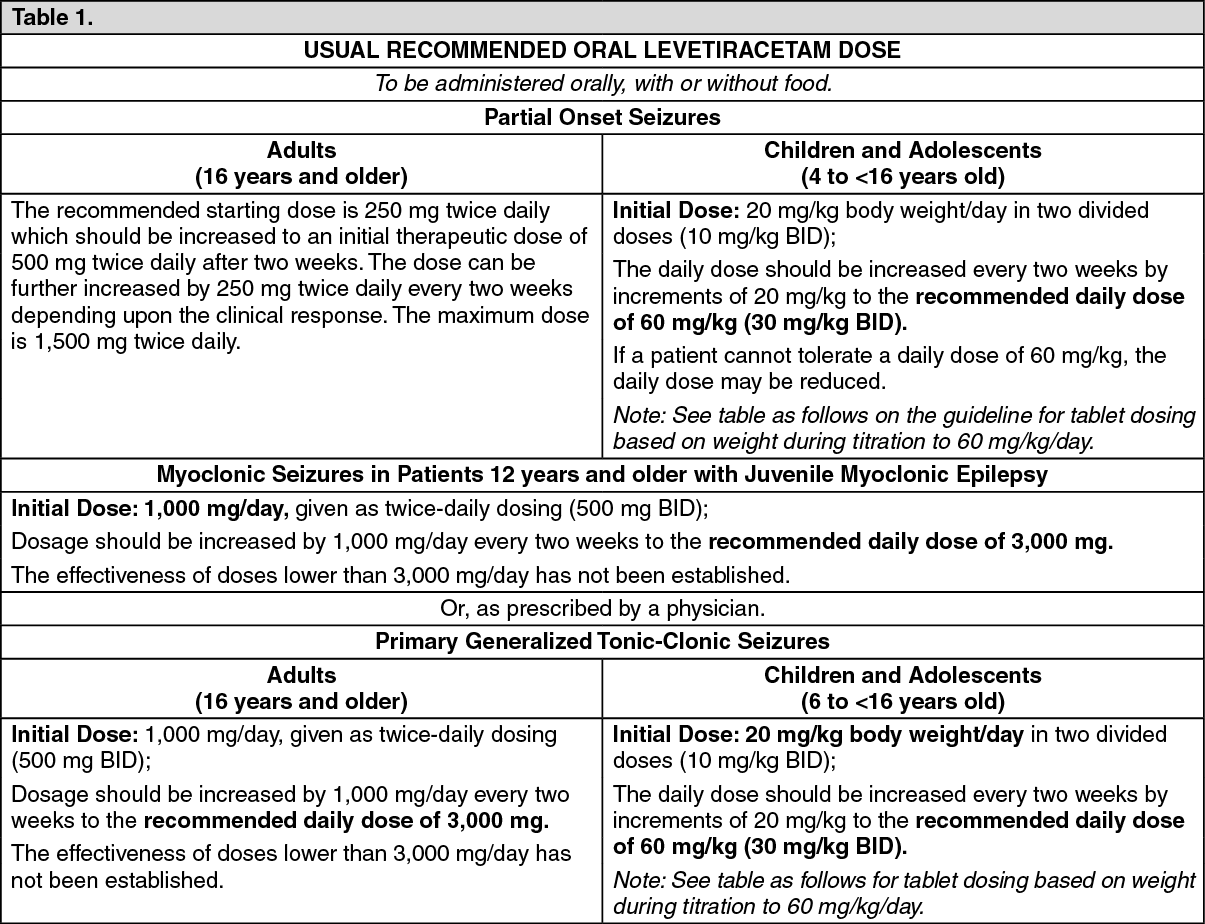 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image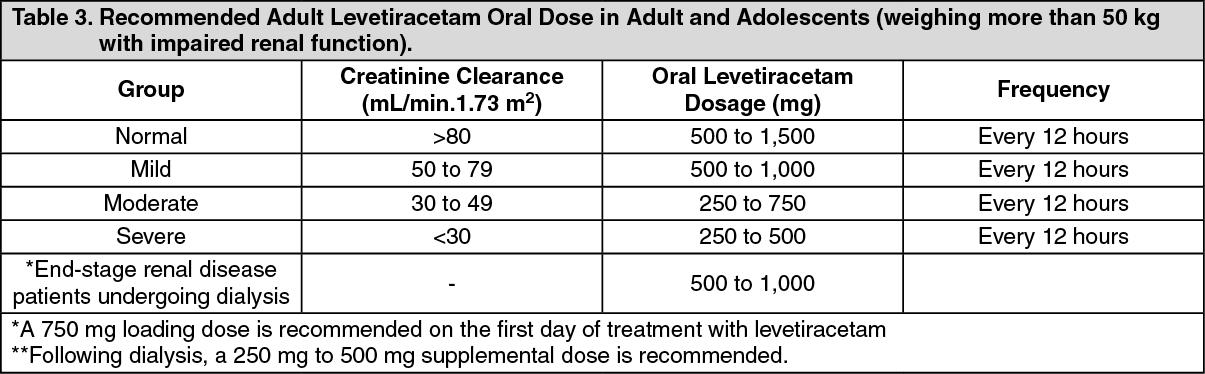 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image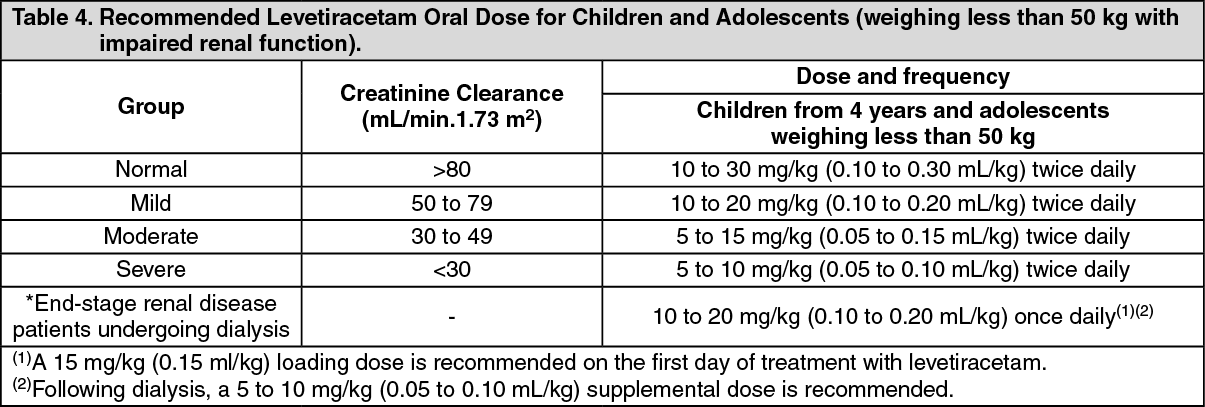 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out