White coloured, elongated shaped, biconvex, both side plain film-coated tablet.
Each film-coated tablet contains: Sevelamer carbonate 800 mg.
Pharmacotherapeutic group: All other therapeutic products, drugs for treatment of hyperkalemia and hyperphosphataemia. ATC code: V03AE02.
Pharmacology: Pharmacodynamics: Patients with chronic kidney disease retain phosphorus and can develop hyperphosphataemia. High serum phosphorus can precipitate serum calcium resulting in ectopic calcifications. When the product of serum calcium and phosphorus concentrations (Ca x P) exceeds 55 mg2/dL2 there is an increased risk that ectopic calcification will occur. Hyperphosphatemia plays a role in the development of secondary hyperparathyroidism in renal insufficiency. An increase in parathyroid hormone (PTH) level is characteristic of patients with chronic kidney disease. Increased levels of PTH can lead to osteitis fibrosa. A decrease in serum phosphorus may decrease serum PTH levels.
Treatment of hyperphosphatemia includes reduction of dietary intake of phosphate, inhibition of intestinal phosphate absorption with phosphate binders and removal of phosphate with dialysis. Sevelamer Carbonate taken with meals has been shown to decrease serum phosphorus concentrations in patients with chronic kidney disease who are on hemodialysis. In vitro studies have shown that the capsule and tablet formulations bind phosphate to a similar extent.
Sevelamer Carbonate treatment also results in a lowering of low-density lipoprotein (LDL) and total serum cholesterol levels.
Mode of Action/Pharmacodynamic Characteristics: Mechanism of Action: Sevelamer Carbonate contains Sevelamer hydrochloride, a non-absorbed phosphate binding poly (allylamine hydrochloride) polymer, free of metal and calcium. It contains multiple amines separated by one carbon from the polymer backbone. These amines exist in a partially protonated form in the intestine and interact with phosphate molecules through ionic and hydrogen bonding. By binding phosphate in the dietary tract, Sevelamer hydrochloride lowers the phosphate concentration in the serum.
In clinical trials, Sevelamer hydrochloride has been shown to be effective in reducing serum phosphorus in patients receiving hemodialysis or peritoneal dialysis.
Sevelamer hydrochloride decreases the incidence of hypercalcemic episodes as compared to patients using calcium-based phosphate binders alone. The effects on phosphate and calcium were proven to be maintained throughout a study with one-year follow-up.
Sevelamer hydrochloride has been shown to bind bile acids in vitro and in vivo in experimental animal models. Bile acid binding by ion exchange resins is a well-established method of lowering blood cholesterol. In clinical trials both the mean total and LDL cholesterol declined by 15-31%. This effect is observed after 2 weeks and is maintained with long-term treatment. Triglycerides, HDL cholesterol and albumin did not change.
In the clinical studies in hemodialysis patients, Sevelamer hydrochloride alone did not have a consistent and clinically significant effect on serum intact parathyroid hormone (iPTH). In patients with secondary hyperparathyroidism Sevelamer Carbonate should be used within the context of a multiple therapeutic approach, which could include calcium supplements, and 1,25-dihydroxy vitamin D3 or one of its analogues to lower the intact parathyroid hormone (iPTH) levels.
Pharmacokinetics: Absorption: A mass balance study using 14C-Sevelamer hydrochloride, in 16 healthy male and female volunteers showed that Sevelamer hydrochloride is not systematically absorbed. No absorption studies have been performed in patients with renal disease.
Toxicology: Non-Clinical Safety Data: Non-clinical safety studies were conducted for Sevelamer Carbonate and Sevelamer hydrochloride which contains the same active moiety, Sevelamer.
Acute toxicity: In preclinical studies in rats and dogs, Sevelamer hydrochloride at a human equivalent dose of 10 times the maximum clinical trial dose of 14.4 g/day, reduced absorption of fat soluble vitamins D, E and K, and folic acid.
A single dose study with Sevelamer Carbonate at doses of 10,000, 15,000 and 20,000 mg/kg by oral route (dietary admixture) was conducted in rats. At 20,000 mg/kg/day, there were no unscheduled deaths or any clinical signs observed during the treatment or observation periods. Slightly lower food consumption was recorded for both sexes during the 24-hour treatment period, probably due to minor unpalatability of the dietary admixture at this concentration, but no evidence of a persistent effect was noted during the observation period. Both sexes also had a slightly lower mean body weight gain over the treatment period compared to controls; however, this was not evident during the observation period. Hematology, blood biochemistry and organ weights were unremarkable, and no treatment-related macroscopic findings were observed. Therefore, it was considered that the No Observed Adverse Effect Level (NOAEL) for Sevelamer Carbonate administered over a 24-hour period was 20,000 mg/kg/day.
Carcinogenicity: Standard lifetime carcinogenicity bioassays were conducted in mice and rats. Rats were given Sevelamer hydrochloride by diet at 0.3, 1, or 3 g/kg/day. There was an increased incidence of urinary bladder transitional cell papilloma in male rats (3 g/kg/day) at a human equivalent dose 2 times the maximum clinical trial dose of 12 g/day. Mice received mean dietary doses of 0.8, 3, or 9 g/kg/day. No increased incidence of tumors was observed in mice at a human equivalent dose 3 times the maximum clinical trial dose of 13 g/day, based on a comparison of relative body surface area.
To investigate the mechanism of action of proliferative effects (development of urinary bladder transitional cell papilloma) noted previously in the rat study, Sevelamer Carbonate was administered to male rats by dietary admixture for a period of 13 weeks at nominal dose-levels of 250, 1000 or 4500 mg/kg/day followed by 6 week treatment free period. Sevelamer Carbonate was well tolerated at all dose-levels. Only slightly lower body weight gain was observed in rats treated with 4500 mg/kg/day over the study period. No treatment-related changes were seen in the macroscopic or microscopic examinations. The urine of the mid and high dose Sevelamer Carbonate groups contained significant levels of calcium oxalate crystals, and plasma vitamin E levels were significantly decreased in the high dose group. Known effects of the pharmacological action of Sevelamer Carbonate include decreased vitamin E uptake and modification of other electrolytes in the blood and urine due to altered calcium metabolism. This study confirmed these effects but did not reproduce the proliferative effects observed in the urinary tract in a previous study.
Mutagenicity: In an in vitro mammalian cytogenetic test with metabolic activation, Sevelamer hydrochloride caused a statistically significant increase in the number of structural chromosome aberrations. Sevelamer hydrochloride was not mutagenic in the Ames bacterial mutation assay.
Impairment of fertility: In a study designed to assess potential impairment of fertility, female rats were given dietary doses of 0.5, 1.5, or 4.5 g/kg/day beginning 14 days prior to mating and continuing through gestation. Male rats were given the same doses and treated for 28 days before mating. Sevelamer hydrochloride did not impair fertility in male or female rats at exposures at a human equivalent dose 2 times the maximum clinical trial dose of 13 g/day, based on a comparison of relative body surface area.
Reproduction toxicity: In pregnant rats given dietary doses of 0.5, 1.5 or 4.5 g/kg/day of Sevelamer hydrochloride during organogenesis, reduced or irregular ossification of fetal bones, probably due to a reduced absorption of fat-soluble vitamin D, occurred in mid- and high-dose groups (human equivalent doses less than the maximum clinical trial dose of 13 g). In pregnant rabbits given oral doses of 100, 500 or 1000 mg/kg/day of Sevelamer hydrochloride by gavage during organogenesis, an increase or early resorptions occurred in the high-dose group (human equivalent dose twice the maximum clinical trial dose).
Sevelamer Carbonate is indicated for the control of serum phosphorous in patient with chronic kidney disease (CKD) on dialysis. It is also indicated for the control of hyperphosphatemia in adult patients receiving hemodialysis or peritoneal dialysis. It is also approved for adult CKD patients not on dialysis with serum phosphorous >1.78 mmol/L.
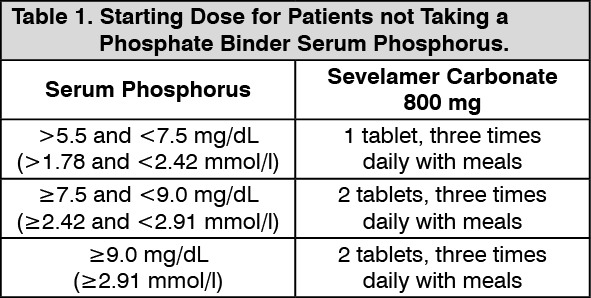
General: Adults and Elderly (>65 years): Patients Not Taking a Phosphorus Binder: The recommended starting dose for patients not taking a phosphate binder is 800 to 1600 mg, which can be administered as one to two Sevelamer carbonate 800 mg tablets with each meal based on serum phosphorus level. (See Table 1.)
 Click on icon to see table/diagram/image
Patients Switching From a Calcium-Based Binder:
Click on icon to see table/diagram/image
Patients Switching From a Calcium-Based Binder: When patients are converting from a calcium based phosphate binder, Sevelamer hydrochloride should be given in equivalent doses on a mg for mg weight basis compared to the patient's previous calcium based phosphate binder. Table 2 gives recommended starting doses of Sevelamer Carbonate based on a patient's current calcium acetate dose. (See Table 2.)
Click on icon to see table/diagram/image
Dose Titration for All Patients Taking Sevelamer Carbonate: Serum phosphorus levels should be closely monitored and the dose of Sevelamer Carbonate adjusted accordingly with the goal of lowering serum phosphorus to 1.78 mmol/L (5.5 mg/dL) or less. Serum phosphorus should be tested every 2 to 3 weeks until a stable serum phosphorus level is reached, and on a regular basis thereafter.
Special Populations: Use in Children: The safety and efficacy of Sevelamer Carbonate has not been established in patients below the age of 18 years.
Use in the Elderly: Same as adults.
Administration: Route of administration is oral.
Sevelamer Carbonate 800 mg tablets can be taken three times per day with meals at a dosage based on individual patient requirements to control phosphate levels. Tablets should be swallowed intact and should not be crushed, chewed, or broken into pieces prior to administration.
In CKD patients on dialysis, the maximum dose studied was 14.4 grams of Sevelamer Carbonate and 13 grams of Sevelamer hydrochloride. Sevelamer hydrochloride, which contains the same active moiety as Sevelamer Carbonate, has been given to normal healthy volunteers in doses of up to 14.4 grams per day for eight days with no adverse effects. There are no reports of overdosage with Sevelamer Carbonate or Sevelamer hydrochloride in patients.
Since Sevelamer is not absorbed, the risk of systemic toxicity is low.
Sevelamer Carbonate is contraindicated: in patients with hypophosphatemia or bowel obstruction.
In patients with hypersensitivity to the active substance or to any of the excipients.
The safety and efficacy of Sevelamer Carbonate in patients with dysphagia, swallowing disorders, severe gastrointestinal motility disorders including severe constipation or major gastrointestinal tract surgery have not been established. Consequently, caution should be exercised when Sevelamer Carbonate is used in patients with these disorders.
Sevelamer Carbonate treatment should be reevaluated in patients who develop severe constipation or other severe gastrointestinal symptoms.
Uncommon case reports of difficulty swallowing the tablet have been reported. Many of these cases involved patients with contributing co-morbid conditions affecting the ability to swallow including swallowing disorders or oroesophageal abnormalities. Caution should be exercised when the tablets are used in these patients. Consider using powder for oral suspension in patients with a history of difficulty swallowing.
Patients with CKD may develop low vitamin A, D, E and K levels, depending on dietary intake and the severity of their disease. Treatment with Sevelamer in preclinical studies, approximately at the equivalent of 6-10 times the maximum clinical trial dose, has been shown to reduce the absorption of vitamins D, E and K, and folic acid. Therefore, in patients not taking supplemental vitamins but on Sevelamer, serum vitamin A, D, and E levels and vitamin K status should be assessed regularly.
Abuse and Dependence: There have been no reports of abuse or dependence of Sevelamer Carbonate or Sevelamer hydrochloride in patients. Since Sevelamer is not absorbed, the risk of abuse or dependence is low.
Driving a Vehicle or Performing Other Hazardous Tasks: No effects on ability to drive and use machines have been observed.
Use in Pregnancy: Pregnancy Category C. The safety of Sevelamer Carbonate has not been established in pregnant or lactating women. Sevelamer Carbonate should only be given to pregnant or lactating women if clearly needed and after careful risk/benefit analysis has been conducted for both the mother and fetus or infant.
Studies in animals have shown minimal reproductive toxicity when Sevelamer was administered to rats at high doses.
There have been no adequate well controlled studies in women undergoing labor and delivery.
Use in Lactation: There have been no studies of the excretion of Sevelamer in human milk, but since Sevelamer is not absorbed, excretion in breast milk is not expected.
The most frequently occurring adverse reactions for the Sevelamer Carbonate tablets in a short term (8-week cross-over) study were: nausea (3%) and vomiting (3%). Most frequently occurring treatment related adverse events for Sevelamer Carbonate powder in a short term (4-week cross-over) study were: nausea (7%), constipation (3%) and vomiting (3%). In long-term studies with Sevelamer hydrochloride, which contains the same active moiety as Sevelamer Carbonate, the most common adverse events included: vomiting (22%), nausea (20%), diarrhea (19%), dyspepsia (16%), abdominal pain (9%), flatulence (8%) and constipation (8%).
In a parallel study with a treatment duration of 12 weeks, the adverse events reported for Sevelamer hydrochloride in peritoneal dialysis patients (N=97) were similar to adverse events observed in hemodialysis patients. Adverse events possibly related to Sevelamer hydrochloride included dyspepsia (12.4%), diarrhea (5.2%), nausea (5.2%), constipation (4.1%), pruritus (4.1%), abdominal distension (3.1%), vomiting (3.1%), fatigue (3.1%), and anorexia (3.1%).
In a double-blind, placebo-controlled, dose titration study with a treatment duration of 8 weeks, the adverse events experienced by the patients in the Sevelamer Carbonate and placebo groups were similar. The most frequently reported treatment-related events were gastrointestinal disorders. Adverse reactions among those treated with Sevelamer Carbonate included: constipation (7.4%), abdominal distension (4.4%), and abdominal discomfort (3.0%).
During post-marketing experience, the following adverse events have been reported in patients receiving Sevelamer Carbonate although no direct relationship to Sevelamer Carbonate could be established: hypersensitivity, pruritus, rash, abdominal pain and uncommon cases of ileus, intestinal obstruction and intestinal perforation.
Sevelamer Carbonate has also been studied in patients with CKD not on dialysis.
Drug/Drug: Interaction studies have not been conducted in patients on dialysis. In interaction studies in healthy volunteers, Sevelamer Carbonate had no effect on the bioavailability of a single-dose of digoxin, warfarin, enalapril, metoprolol or iron. However, the bioavailability of ciprofloxacin was decreased by approximately 50% when co-administered with Sevelamer Carbonate in a single dose study. Consequently, Sevelamer Carbonate should not be taken simultaneously with ciprofloxacin.
During postmarketing experience, reduced concentrations of cyclosporin, mycophenolate mofetil and tacrolimus have been reported in transplant patients when co-administered with Sevelamer hydrochloride without any clinical consequences (for example, graft rejection). The possibility of an interaction cannot be excluded and close monitoring of blood concentrations of cyclosporin, mycophenolate mofetil and tacrolimus should be considered during the use of any of these agents in combination with Sevelamer and after its withdrawal.
During post-marketing experience, very rare cases of increased TSH levels have been reported in patients co-administered Sevelamer Carbonate and levothyroxine. Closer monitoring of TSH levels is therefore recommended in patients receiving both medications. During postmarketing experience, very rare cases of increased phosphate levels have been reported in patients taking proton pump inhibitors co-administered with Sevelamer hydrochloride.
Food: In all clinical studies patients were instructed to take Sevelamer with meals.
Store at temperature not exceeding 30°C.
V03AE02 - sevelamer ; Belongs to the class of drugs used in the treatment of hyperkalemia and hyperphosphatemia.
Fosfamer FC tab 800 mg
30's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image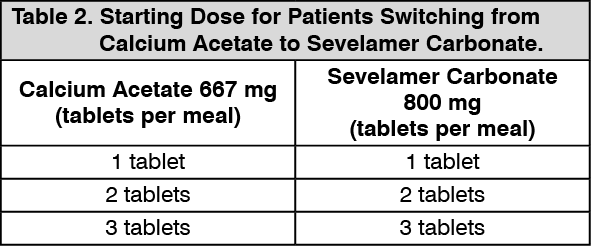 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out