Treatment: Adults: The usual adult dosage range is 1 gram to 2 grams every six to eight hours. Dosage should be determined by susceptibility of the causative organisms, severity of infection, and the condition of the patient (see Table 1 for dosage guidelines).
If C. trachomatis is a suspected pathogen, appropriate anti-chlamydial coverage should be added, because cefoxitin sodium has no activity against this organism.
Cefoxitin for injection may be used in patients with reduced renal function with the following dosage adjustments:
In adults with renal insufficiency, an initial loading dose of 1 gram to 2 grams may be given. After a loading dose, the recommendations for maintenance dosage (Table 2) may be used as a guide.
When only the serum creatinine level is available, the following formula (based on sex, weight, and age of the patient) may be used to convert this value into creatinine clearance. The serum creatinine should represent a steady state of renal function.
Males: (See equation.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Females: 0.85 x above value.
In patients undergoing hemodialysis, the loading dose of 1 to 2 grams should be given after each hemodialysis, and the maintenance dose should be given as indicated in Table 2.
Antibiotic therapy for group a beta-hemolytic streptococcal infections should be maintained for at least 10 days to guard against the risk of rheumatic fever or glomerulonephritis. In staphylococcal and other infections involving a collection of pus, surgical drainage should be carried out where indicated.
Pediatric Patients: The recommended dosage in pediatric patients three months of age and older is 80 to 160 mg/kg of body weight per day divided into four to six equal doses. The higher dosages should be used for more severe or serious infections. The total daily dosage should not exceed 12 grams.
At this time no recommendation is made for pediatric patients from birth to three months of age (see Precautions).
In pediatric patients with renal insufficiency, the dosage and frequency of dosage should be modified consistent with the recommendations for adults (see Table 2).
Prevention: Effective prophylactic use depends on the time of administration. Cefoxitin for injection usually should be given one-half to one hour before the operation, which is sufficient time to achieve effective levels in the wound during the procedure. Prophylactic administration should usually be stopped within 24 hours since continuing administration of any antibiotic increases the possibility of adverse reactions but, in the majority of surgical procedures, does not reduce the incidence of subsequent infection.
For prophylactic use in uncontaminated gastrointestinal surgery, vaginal hysterectomy, or abdominal hysterectomy, the following doses are recommended:
Adults: 2 grams administered intravenously just prior to surgery (approximately one-half to one hour before the initial incision) followed by 2 grams every 6 hours after the first dose for no more than 24 hours.
Pediatric Patients (3 months and older): 30 to 40 mg/kg doses may be given at the times designated previously.
Cesarean section patients: For patients undergoing cesarean section, either a single 2 gram dose administered intravenously as soon as the umbilical cord is clamped OR a 3-dose regimen consisting of 2 grams given intravenously as soon as the umbilical cord is clamped followed by 2 grams 4 and 8 hours after the initial dose is recommended. (See Table 1, Table 2, and Table 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Direction for Reconstitution: Table 3 is provided for convenience in constituting cefoxitin for injection for intravenous administration.
For Vials: One gram should be constituted with at least 10 mL of Sterile Water for Injection, Bacteriostatic Water for Injection, 0.9 percent Sodium Chloride Injection, or 5 percent Dextrose Injection. These primary solutions may be further diluted in 50 to 1000 mL of the diluents listed under the Vials and Bulk Packages portion of the Compatibility and Stability section.
Benzyl alcohol as a preservative has been associated with toxicity in neonates. While toxicity has not been demonstrated in pediatric patients greater than three months of age, in whom use of cefoxitin for injection may be indicated, small pediatric patients in this age range may also be at risk for benzyl alcohol toxicity. Therefore, diluent containing benzyl alcohol should not be used when cefoxitin for injection is constituted for administration to pediatric patients in this age range.
Administration: Cefoxitin for injection may be administered intravenously after constitution.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration whenever solution and container permit.
Intravenous Administration: The intravenous route is preferable for patients with bacteremia, bacterial septicemia, or other severe or life-threatening infections, or for patients who may be poor risks because of lowered resistance resulting from such debilitating conditions as malnutrition, trauma, surgery, diabetes, heart failure, or malignancy, particularly if shock is present or impending.
For intermittent intravenous administration, a solution containing 1 gram or 2 grams in 10 mL of Sterile Water for Injection can be injected over a period of three to five minutes. Using an infusion system, it may also be given over a longer period of time through the tubing system by which the patient may be receiving other intravenous solutions. However, during infusion of the solution containing cefoxitin, it is advisable to temporarily discontinue administration of any other solutions at the same site.
For the administration of higher doses by continuous intravenous infusion, a solution of cefoxitin may be added to an intravenous bottle containing 5 percent Dextrose Injection, 0.9 percent Sodium Chloride Injection, or 5 percent Dextrose and 0.9 percent Sodium Chloride Injection. BUTTERFLY (registered trademark of Abbott Laboratories, Inc.) or scalp vein-type needles are preferred for this type of infusion.
Solutions of cefoxitin, like those of most beta-lactam antibiotics, should not be added to aminoglycoside solutions (e.g., gentamicin sulfate, tobramycin sulfate, amikacin sulfate) because of potential interaction. However, cefoxitin and aminoglycosides may be administered separately to the same patient.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image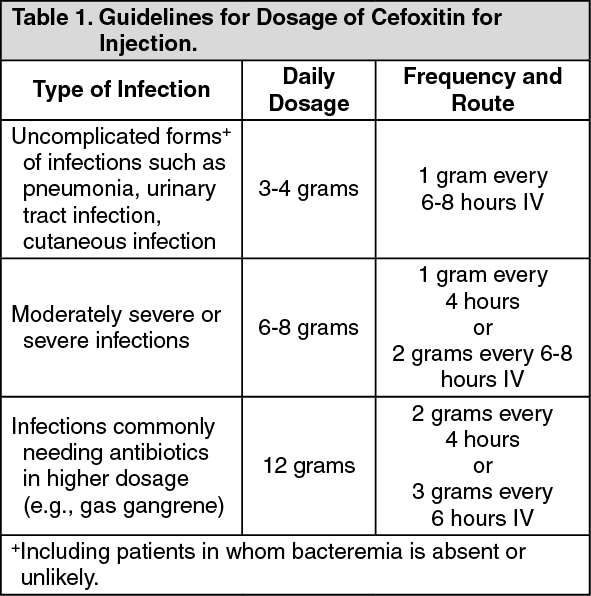 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image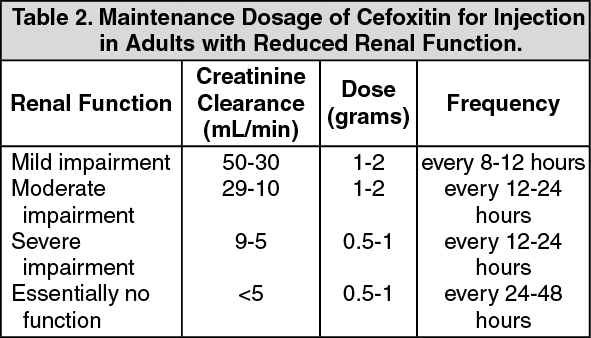 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image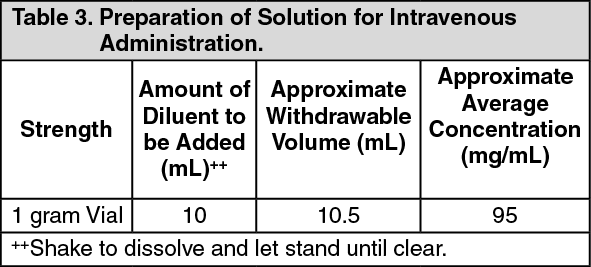 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out