Gemcitabine should only be prescribed by a physician qualified in the use of anti-cancer chemotherapy.
Recommended posology: Bladder cancer: Combination use: The recommended dose for gemcitabine is 1000 mg/m
2, given by 30-minute infusion. The dose should be given on Days 1, 8 and 15 of each 28-day cycle in combination with cisplatin. Cisplatin is given at a recommended dose of 70 mg/m
2 on Day 1 following gemcitabine or day 2 of each 28-day cycle. This 4-week cycle is then repeated. Dosage reduction with each cycle or within a cycle may be applied based upon the grade of toxicity experienced by the patient.
Pancreatic cancer: The recommended dose of gemcitabine is 1000 mg/m
2, given by 30-minute intravenous infusion. This should be repeated once weekly for up to 7 weeks followed by a week of rest. Subsequent cycles should consist of injections once weekly for 3 consecutive weeks out of every 4 weeks. Dosage reduction with each cycle or within a cycle may be applied based upon the grade of toxicity experienced by the patient.
Non small Cell lung cancer: Monotherapy: The recommended dose of gemcitabine is 1000 mg/m
2, given by 30-minute intravenous infusion. This should be repeated once weekly for 3 weeks, followed by a 1-week rest period. This 4-week cycle is then repeated. Dosage reduction with each cycle or within a cycle may be applied based upon the grade of toxicity experienced by the patient.
Combination use: The recommended dose for gemcitabine is 1250 mg/m
2 body surface area given as a 30-minute intravenous infusion on Day 1 and 8 of the treatment cycle (21 days). Dosage reduction with each cycle or within a cycle may be applied INP003based upon the grade of toxicity experienced by the patient. Cisplatin has been used at doses between 75-100 mg/m
2 once every 3 weeks.
Breast cancer: Combination use: Gemcitabine in combination with paclitaxel is recommended using paclitaxel (175 mg/m
2) administered on Day 1 over approximately 3-hours as an intravenous infusion, followed by gemcitabine (1250 mg/m
2) as a 30-minute intravenous infusion on Days 1 and 8 of each 21-day cycle. Dose reduction with each cycle or within a cycle may be applied based upon the grade of toxicity experienced by the patient. Patients should have an absolute granulocyte count of at least 1,500 (x 10
6/l) prior to initiation of gemcitabine + paclitaxel combination.
Ovarian cancer: Combination use: Gemcitabine in combination with carboplatin is recommended using gemcitabine 1000 mg/m
2 administered on Days 1 and 8 of each 21-day cycle as a 30-minute intravenous infusion. After gemcitabine, carboplatin will be given on Day 1 consistent with a target Area under curve (AUC) of 4.0 mg/ml·min. Dosage reduction with each cycle or within a cycle may be applied based upon the grade of toxicity experienced by the patient.
Monitoring for toxicity and dose modification due to toxicity: Dose modification due to non haematological toxicity: Periodic physical examination and checks of renal and hepatic function should be made to detect non-haematological toxicity. Dosage reduction with each cycle or within a cycle may be applied based upon the grade of toxicity experienced by the patient. In general, for severe (Grade 3 or 4) non-haematological toxicity, except nausea/vomiting, therapy with gemcitabine should be withheld or decreased depending on the judgement of the treating physician. Doses should be withheld until toxicity has resolved in the opinion of the physician.
For cisplatin, carboplatin, and paclitaxel dosage adjustment in combination therapy, please refer to the corresponding Summary of Product Characteristics.
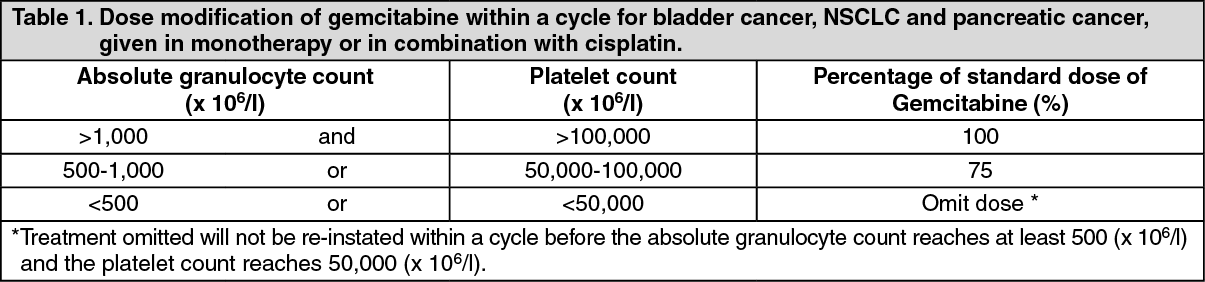
Dose modification due to haematological toxicity: Initiation of a cycle: For all indications, the patient must be monitored before each dose for platelet and granulocyte counts. Patients should have an absolute granulocyte count of at least 1,500 (x 10
6/l) and platelet account of 100,000 (x 10
6/l) prior to the initiation of a cycle. (see Table 1,2 and 3)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Dose modifications due to haematological toxicity in subsequent cycles, for all indications The gemcitabine dose should be reduced to 75% of the original cycle initiation dose, in the case of the following haematological toxicities: Absolute granulocyte count < 500 x 10
6/l for more than 5 days; Absolute granulocyte count < 100 x 10
6/l for more than 3 days; Febrile neutropaenia; Platelets < 25,000 x 10
6/l ; Cycle delay of more than 1 week due to toxicity.
Method of administration: Gemcitabine is tolerated well during infusion and may be administered ambulant. If extravasation occurs, generally the infusion must be stopped immediately and started again in another blood vessel. The patient should be monitored carefully after the administration. For instructions on reconstitution, see Cautions of Usage.
Special populations:
Patients with renal or hepatic impairment: Gemcitabine should be used with caution in patients with hepatic or renal insufficiency as there is insufficient information from clinical studies to allow for clear dose recommendations for these patient populations.
Elderly population (> 65 years): Gemcitabine has been well tolerated in patients over the age of 65. There is no evidence to suggest that dose adjustments, other than those already recommended for all patients, are necessary in the elderly.
Paediatric population (< 18 years): Gemcitabine is not recommended for use in children under 18 years of age due to insufficient data on safety and efficacy.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image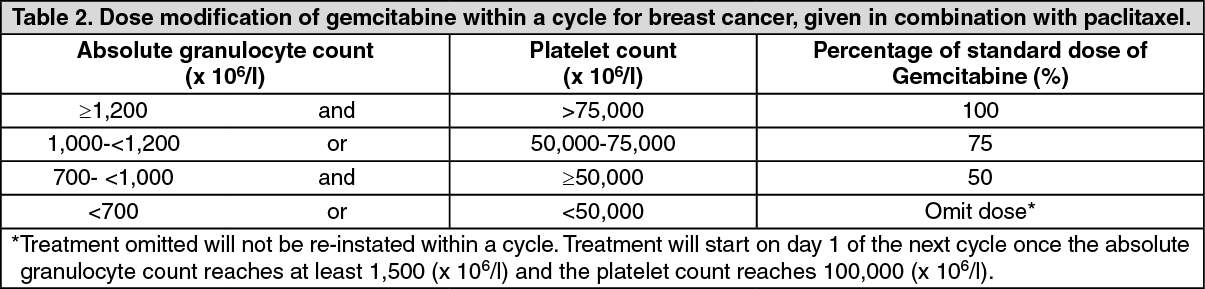 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image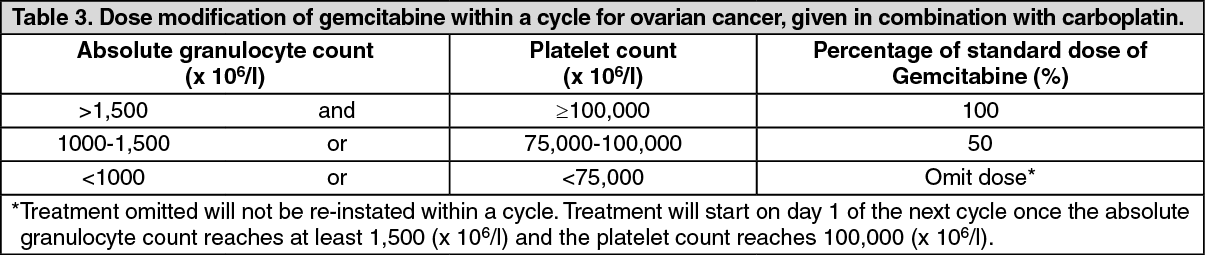 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image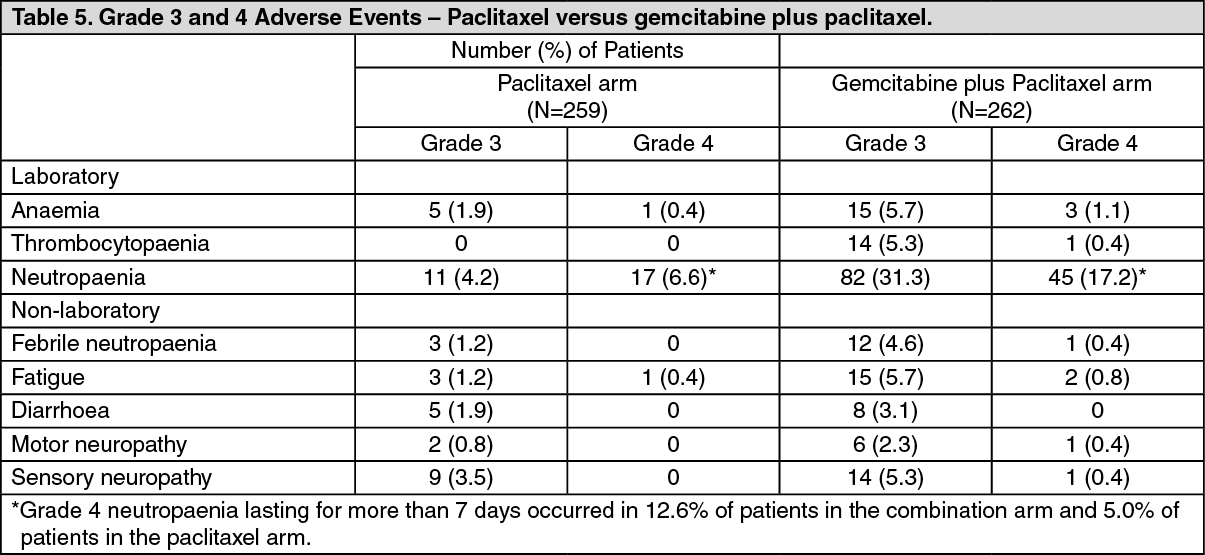 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image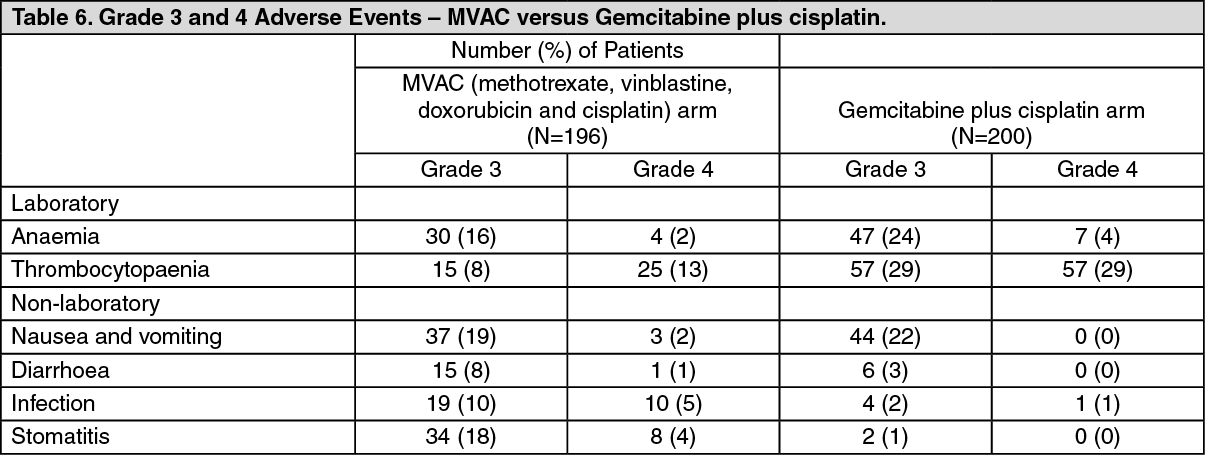 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image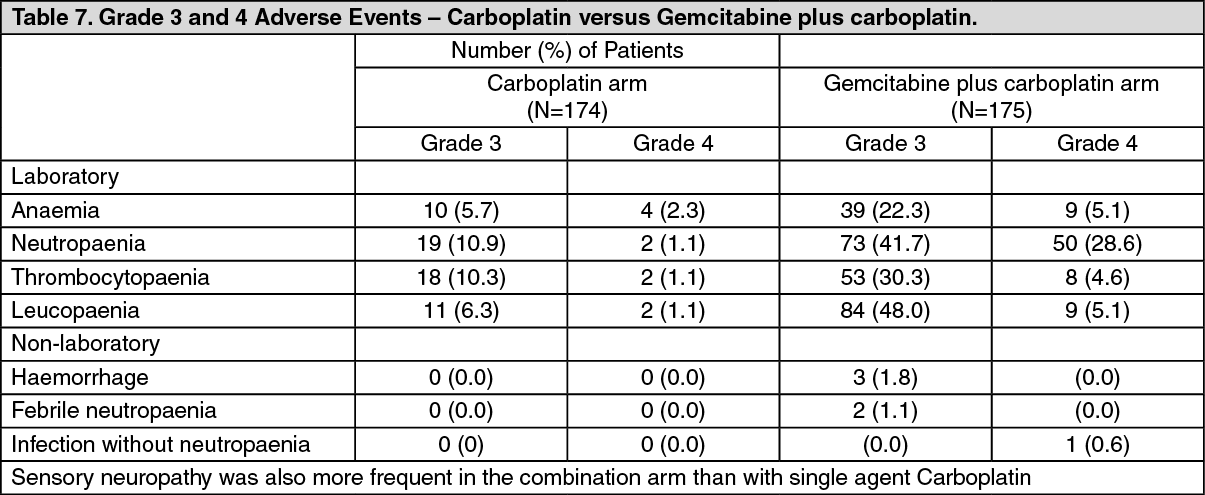 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out