The preparation may be administered by intravenous injection, by intravenous infusion, or by intramuscular injection. The preferred method for initial emergency use being intravenous injection. Following the initial period, consideration should be given to employing a longer acting injectable preparation or an oral preparation. In treating severe shock, there is a tendency in current medical practice to use massive (pharmacologic) doses of corticosteroids. Therapy is initiated by administering HYDROCORTISONE SODIUM SUCCINATE FOR INJECTION intravenously over a period of one to several minutes.
In general, high dose corticosteroid therapy should be continued only until the patient's condition has stabilized-usually not beyond 48 to 72 hours. Although adverse effects are associated with high dose, short-term corticoid therapy is uncommon, peptic ulceration may occur. Prophylactic antacid therapy may be indicated. When massive hydrocortisone therapy must be continued beyond 48-72 hours, hypernatremia may occur. Under such circumstances it may be desirable to replace HYDROCORTISONE SODIUM SUCCINATE for injection with corticoid such as methylprednisolone sodium succinate which causes little or no sodium retention.
Hydrocortisone may be given intravenously, by slow injection or infusion, in the form of water-soluble derivative such as hydrocortisone sodium succinate or hydrocortisone sodium phosphate when a rapid effect is required in emergencies: such conditions are acute adrenocortical insufficiency caused by Addisonian or post-adrenalectomy crises, by the abrupt accidental withdrawal of therapy in corticosteroid-treated patients, or by the inability of the adrenal glands to cope with increased stress in such patients; certain allergic emergencies such as anaphylaxis; acute severe asthma and shock. The usual dose is the equivalent of 100 to 500 mg of hydrocortisone, repeated 3 or 4 times in 24 hours, according to the severity of the condition and the patient's response.
Fluids and electrolytes should be given as necessary to correct any associated metabolic disorder. Similar doses to those specified previously may also be given intramuscularly but the response is likely to be less rapid than that observed following intravenous administration. Corticosteroids are considered to be of secondary value in anaphylactic shock because of their relatively slow onset of action, but intravenous hydrocortisone may be a useful adjunct to adrenaline to prevent further deterioration in severely affected patients.
In patients with adrenal deficiency states supplementary corticosteroid therapy may be necessary during some surgical operations and hydrocortisone sodium succinate or sodium phosphate may be given intramuscularly or intravenously before surgery. Various regimens have been proposed. In patients taking more than 10 mg of prednisolone or its equivalent by mouth daily, the British National Formulary recommends the following regimen: minor surgery under general anaesthesia, either the usual oral corticosteroid dose on the morning of surgery of hydrocortisone 25 to 50 mg (usually as the sodium succinate) intravenously at induction; the usual oral corticosteroid dose is recommenced after surgery; moderate of major surgery, the usual oral corticosteroid dose on the morning of surgery, plus hydrocortisone 25 to 50 mg intravenously at induction, and followed by similar doses of hydrocortisone 3 times daily, for 24 hours after moderate surgery and 48 to 72 hours after major surgery; the usual corticosteroid dose is resumed once hydrocortisone injections are stopped.
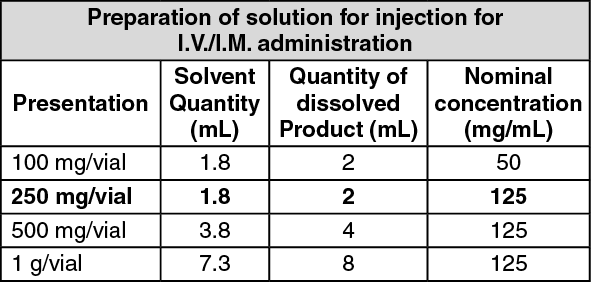
Preparation of solution for injection for I.V./I.M. administration: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Note: Discard any remaining portion after use.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out