Adverse effects that have been reported with nicardipine IV are as follows:
Body as a Whole: Asthenia, chest pain, fever, neck pain, malaise, fatigue, peripheral or facial edema, infection, arthralgia.
Cardiovascular: Hypotension, postural hypotension, exertional hypotension, tachycardia, ECG abnormality, ventricular extra systoles, extra systoles, hemoperiocardium, hypertension, supraventricular tachycardia, syncope, vasodilation, ventricular tachycardia, angina pectoris, atrioventricular block, ST segment depression, inverted T wave, deep-vein thrombophlebitis, sick sinus syndrome, flushing, palpitations, myocardial infarction, atrial fibrillation, pericarditis, peripheral vascular disorder.
Digestive: Abdominal pain, nausea, vomiting, dyspepsia, constipation, diarrhea, dry mouth, anorexia, heartburn.
Metabolic and Nutritional: Hypokalemia, hypophosphatemia, hyperglycemia, abnormal hepatic function test results, increased plasma renin concentration.
Nervous: Headache, dizziness, hypesthesia, intracranial hemorrhage, paresthesia, confusion, hypertonia, somnolence, insomnia, hot flashes, vertigo, hyperkinesia, impotence, mental depression, anxiety, cerebrovascular accident, cerebral ischemia, lassitude, nervousness, lightheadedness.
Hemic and Lymphatic: Thrombocytopenia.
Respiratory: Dyspnea, respiratory disorder, rhinitis, sinusitis.
Skin and Appendages: Sweating, injection site reaction and pain, rash.
Urogenital: Polyuria, hematuria, increased urinary frequency, nocturia, urinary retention.
Special Senses: Conjunctivitis, abnormal or blurred vision, ear disorder, tinnitus.


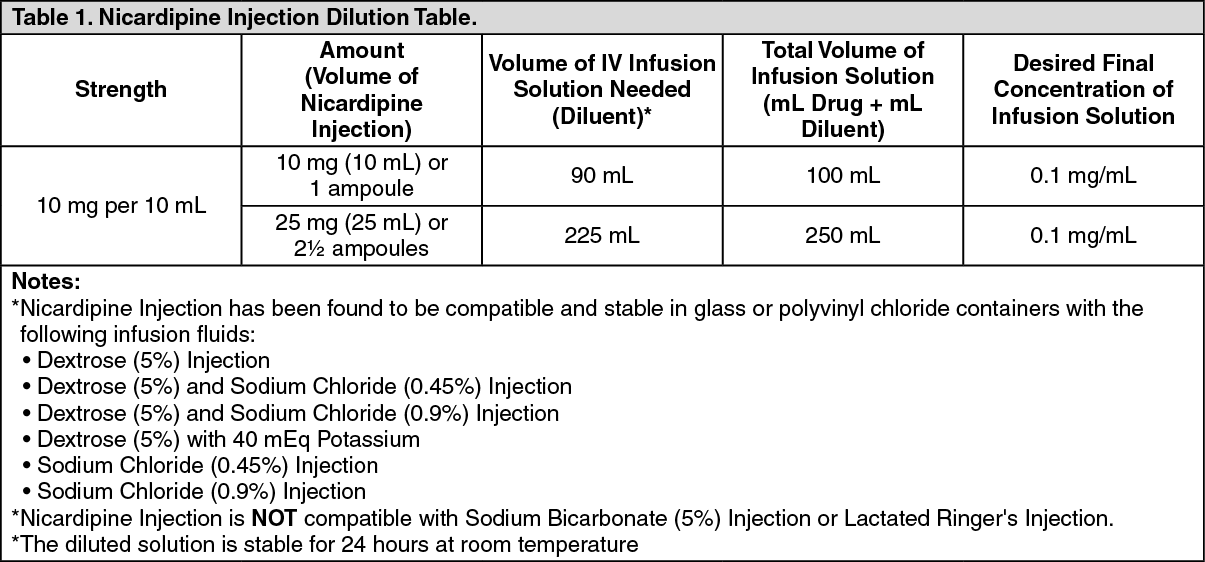 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image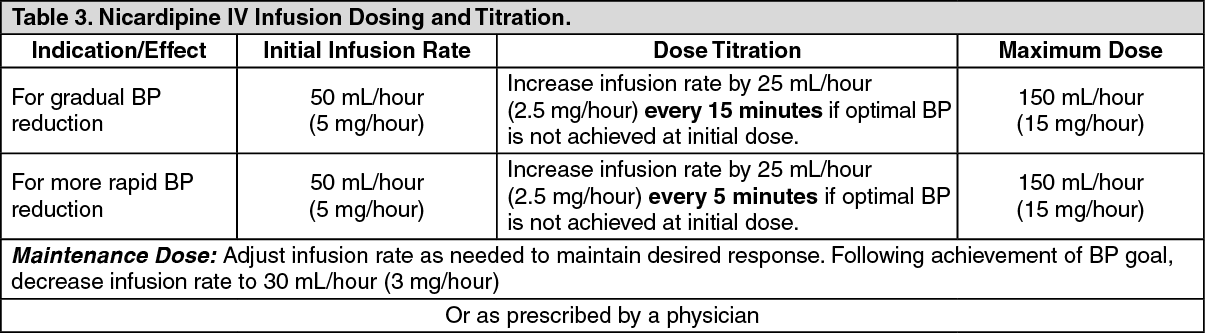 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out