


 Sign Out
Sign Out
Neuropsychiatric Adverse Events: Partial Onset Seizures: Adults: Somnolence and fatigue: In controlled trials of adult patients with epilepsy experiencing partial onset seizures, 14.8% of Levetiracetam tablet-treated patients reported somnolence, compared to 8.4% of placebo patients. There was no clear dose response up to 3000 mg/day. In a study where there was no titration, about 45% of patients receiving 4000 mg/day reported somnolence. The somnolence was considered serious in 0.3% of the treated patients, compared to 0% in the placebo group. About 3% of Levetiracetam tablet-treated patients discontinued treatment due to somnolence and 1.4% of treated patients reduced the dose. (0.7% and 0.9% in the placebo patients, respectively) 0.3% of Levetiracetam tablet treated patients were hospitalized due to somnolence. In non-comparative, phase 3 clinical trials of patients with epilepsy experiencing uncontrolled partial onset seizures (n=100), incidence of somnolence was 36.0 % (36/100), that was incidence (18.8%) in the same designed foreign non-comparative, clinical trial (n=1541). In controlled trials of adult patients with epilepsy experiencing partial onset seizures, 14.7% of treated patients reported asthenia, compared to 9.1% of placebo patients. Treatment was discontinued in 0.8% of treated patients as compared to 0.5% of placebo patients. In 0.5% of treated patients and in 0.2% of placebo patients the dose was reduced.
Coordination difficulties: A total of 3.4% of Levetiracetam-treated patients experienced coordination difficulties, (reported as either ataxia, abnormal gait, or incoordination) compared to 1.6% of placebo patients. A total of 0.4% of patients in controlled trials discontinued levetiracetam treatment due to ataxia, compared to 0% of placebo patients. In 0.7% of treated patients and in 0.2% of placebo patients the dose was reduced due to coordination difficulties, while one of the treated patients was hospitalized due to worsening of preexisting ataxia.
Behavioral abnormalities: In controlled trials of patients with epilepsy experiencing psychotic symptoms, 5 (0.7%) of Levetiracetam tablet treated patients experienced psychotic symptoms compared to 1 (0.2%) placebo patient. Two (0.3%) Levetiracetam tablet-treated patients were hospitalized and their treatment was discontinued. Both events, reported as psychosis, developed within the first week of treatment and resolved within 1 to 2 weeks following treatment discontinuation. Two other events, reported as hallucinations, occurred after 1-5 months and resolved within 2-7 days while the patients remained on treatment. In one patient experiencing psychotic depression occurring within a month, symptoms resolved within 45 days while the patient continued treatment. A total of 13.3% of Levetiracetam tablet patients experienced other behavioral symptoms (reported as aggression, agitation, anger, anxiety, apathy, depersonalization, depression, emotional lability, hostility, irritability, etc.) (6.2% of placebo patients). Approximately half of these patients reported these events within the first 4 weeks. A total of 1.7% of treated patients discontinued treatment due to these events and the treatment dose was reduced in 0.8% of treated patients (0.2% and 0.5% of placebo patients, respectively). A total of 0.8% of treated patient behavioral event (0.2% of placebo patients) and were had a serious behavioral event (0.2% of placebo patients) hospitalized. 4 (0.5%) of Levetiracetam tablet treated patients experienced suicidal attempt (0% of placebo patients). One patient committed suicide. The other 3 patients didn't discontinue therapy or didn't reduce the dose, due to adverse reaction. Such adverse reaction occurred after treatment during 4 weeks~6 months.
Pediatric Patients: Somnolence and fatigue: In the double-blind, controlled trial in children with epilepsy experiencing partial onset seizures, 22.8 % of Levetiracetam-treated patients experienced somnolence, compared to 11.3% of placebo patients. The design of the study prevented accurately assessing dose-response effects. No patients discontinued treatment for somnolence. In about 3.0% of Levetiracetam-treated patients and in 3.1% of placebo patients the dose was reduced as a result of somnolence.
Asthenia: Asthenia was reported in 8.9% of Levetiracetam-treated patients, compared to 3.1% of placebo patients. No patient discontinued treatment for asthenia, but asthenia led to a dose reduction in 3.0% of Levetiracetam treated patients compared to 0% of placebo patients.
Behavioral abnormalities: A total of 37.6% of the Levetiracetam-treated patients experienced behavioral symptoms (reported as agitation, anxiety, apathy, depersonalization, depression, emotional lability, hostility, hyperkinesia, nervousness, neurosis, and personality disorder) (18.6% of placebo patients). One Levetiracetam-treated patients experienced suicidal ideation. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA total of 3.0% of Levetiracetam-treated patients discontinued treatment due to psychotic and nonpsychotic adverse events, compared to 4.1% of placebo patients. Overall, 10.9% of Levetiracetam-treated patients experienced behavioral symptoms associated with discontinuation or dose reduction, compared to 6.2% of placebo patients.
Primary Generalized Tonic-Clonic Seizures: Primary generalized Tonic: In the double-blind, controlled trial in patients with idiopathic generalized epilepsy experiencing primary generalized tonic-clonic seizures, irritability was the most frequently reported psychiatric adverse event occurring in 6.3% of Levetiracetam-treated patients compared to 2.4% of placebo patients. Additionally, non-psychotic behavioral disorders (reported as abnormal behavior, aggression, conduct disorder, and irritability) occurred in 11.4% of the Levetiracetam-treated patients compared to 3.6% of placebo patients. Of the Levetiracetam-treated patients experiencing non-psychotic behavioral disorders, one patient discontinued treatment due to aggression. Non-psychotic mood disorders (including anger, apathy, depression, mood altered, mood swings, negativism, and tearfulness) occurred in 12.7% of Levetiracetam-treated patients compared to 8.3% of placebo patients. No Levetiracetam-treated patients discontinued or had a dose reduction as a result of these events. One Levetiracetam-treated patients experienced suicidal ideation. One patient experienced delusional behavior that required the lowering of the dose of Levetiracetam.
In a long-term open label study that examined patients with various forms of primary generalized epilepsy, along with the non-psychotic behavioral disorders, 2 of 192 patients studied exhibited psychotic-like behavior. Behavior in one case was characterized by auditory hallucinations and suicidal thoughts and led to Levetiracetam discontinuation. The other case was described as worsening of preexistent schizophrenia and did not lead to drug discontinuation.
Adverse reactions from controlled clinical studies: Levetiracetam has been administered to >3000 subjects and patients. One thousand and twenty three (1,023) patients with epilepsy participated in controlled clinical studies.
Pooled safety data from these studies conducted in adult patients showed that 46.4% and 42.2% of the patients experienced adverse reactions in the Levetiracetam and placebo groups, respectively, and that 2.4% and 2% of the patients experienced serious adverse reactions in the Levetiracetam and placebo groups, respectively. The most commonly reported adverse reactions were somnolence, asthenia and dizziness. In the pooled safety analysis, there was no evidence of dose-response relationship but incidence and severity of the CNS-related adverse reactions decreased over time.
In monotherapy, 49.8% of the subjects experienced at least 1 adverse reaction. The most frequently reported adverse reactions were fatigue and somnolence.
A study conducted in pediatric patients (4-16 years) showed that 55.4% of the patients in the Levetiracetam group and 40.2% of the patients in the placebo group experienced adverse reactions. Serious adverse reactions were experienced in 0% of the patients in the Levetiracetam group and 1% of the patients in the placebo group. The most commonly reported adverse reactions were somnolence, hostility, nervousness, emotional lability, agitation, anorexia, asthenia and headache in the pediatric population. Safety results in pediatric patients were consistent with the safety profile of Levetiracetam in adults except for behavioral and psychiatric adverse reactions which were more common in children than in adults (38.6% vs 18.6%). However, the relative risk was similar in children as compared to adults.
A study conducted in pediatric patients (1 month to <4 years) with partial onset seizures showed that 21.7% of the patients in the LEV group and 7.1% of the patients in the placebo group experienced adverse reactions. No serious adverse reactions were experienced in patients in the LEV or placebo group. During the long-term follow-up study N01148, the most frequent adverse reactions in the 1-month to <4-year group were irritability (7.9%), convulsion (7.2%), somnolence (6.6%), psychomotor hyperactivity (3.3%), sleep disorder (3.3%), and aggression (3.3%). Safety results in pediatric patients were consistent with the safety profile of Levetiracetam in older children 4-16 years.
A study conducted in adults and adolescents with myoclonic seizures (12-65 years) showed that 33.3% of the patients in the Levetiracetam group (30% of the patients in the placebo group) experienced adverse reactions. The most commonly reported adverse reactions were headache and somnolence. The incidence of adverse reactions in patients with myoclonic seizures was lower than that in adult patients with partial onset seizures (33.3% vs 46.4%).
A study conducted in adults and children (4-65 years) with idiopathic generalized epilepsy with primary generalized tonic-clonic seizures showed that 39.2% of the patients in the Levetiracetam group and 29.8% of the patients in the placebo group experienced adverse reactions. The most commonly reported adverse reaction was fatigue.
The most commonly reported adverse reactions with LEV IV solution were headache and dizziness.
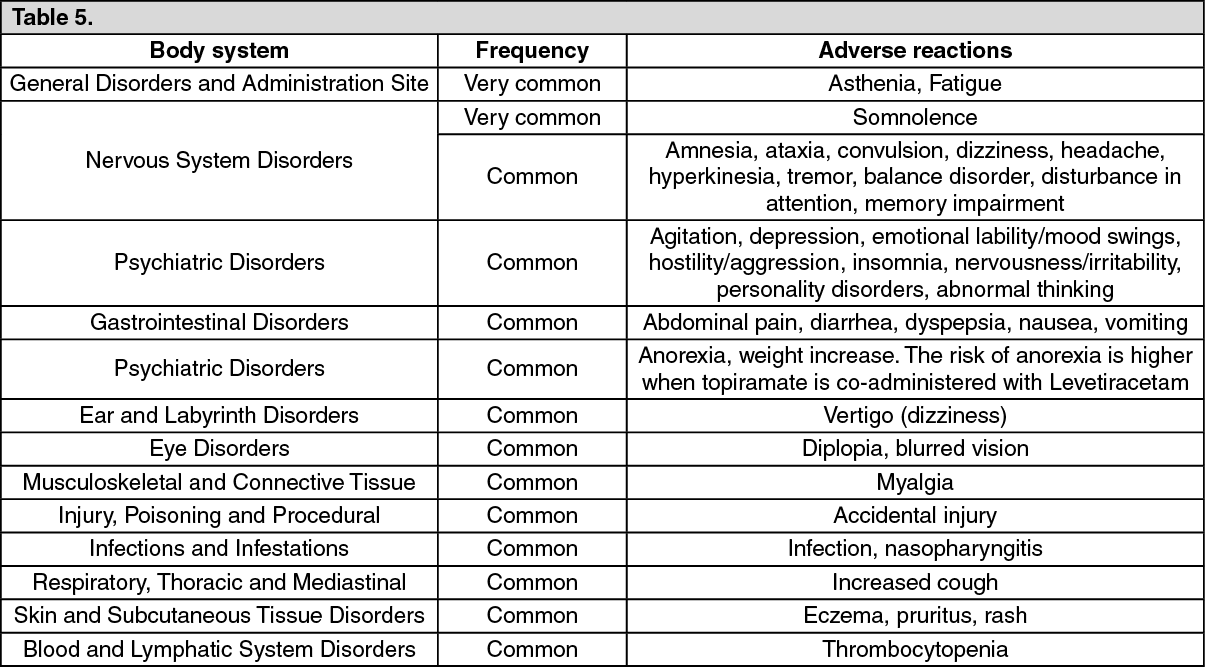
Adverse reactions reported in clinical studies (adults and children) are listed in the following table per System Organ Class and per frequency. The frequency is defined as follows: very common (1/10); common (1/100 to <1/10); uncommon (1/1,000 to <1/100); rare (1/10,000 to <1/1,000) and very rare (<1/10,000). (See Table 5.)
 Click on icon to see table/diagram/image
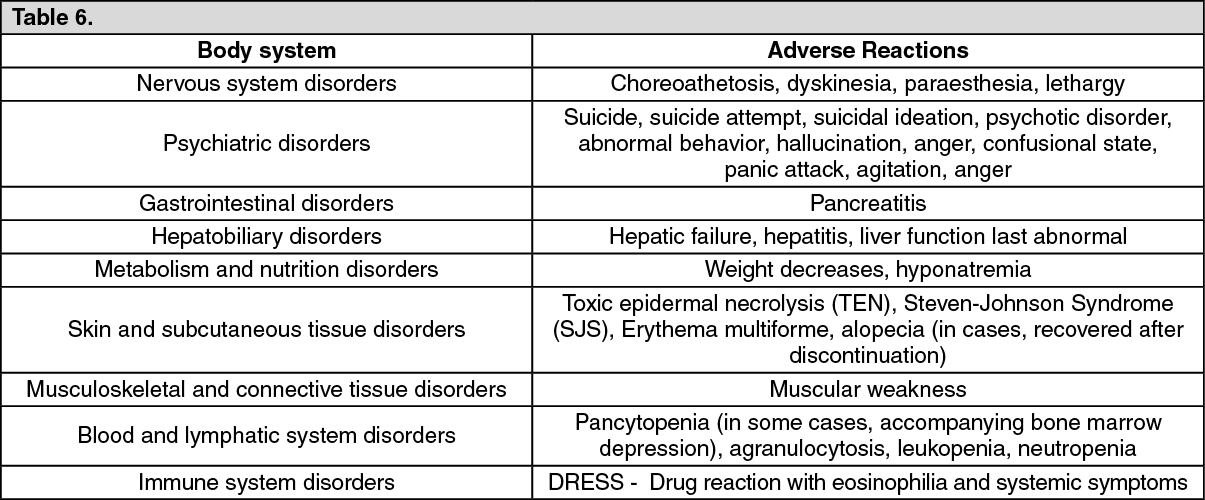
Click on icon to see table/diagram/imageAdverse reactions from domestic post marketing surveillance in post marketing surveillance, adverse reactions of Nervous system disorders and Psychiatric disorders have been most frequently reported. The following adverse reactions have been additionally reported in post marketing surveillance. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDomestic post marketing surveillance of Levetiracetam tablet and liquid products. In domestic post marketing surveillance for 4,896 patients over 6 years for re-evaluation, onset of AEs was 7.76% (n: 380/4896, 438 cases), with or without causality. Major AE was somnolence 2.23% (n: 109/4896, 110 cases), convulsion 1.21% (n: 59/4896, 59 cases), dizziness 1.04% (n: 51/4896, 52 cases), and headache 0.59% (n: 29/4896, 30 cases). Most of AEs were mild or moderate.
Onset of ADE whose causality with this drug cannot be excluded was 7.25% (n: 355/4896, 406 cases), major ADR was somnolence 2.23% (n: 109/4896, 110 cases), convulsion 1.06% (n: 52/4896, 52 cases), dizziness 0.98% (n: 48/4896, 49 cases), headache and hypersensitivity, 0.49% respectively (n: 24/4896, 25 cases).
As serious ADE, suicide attempt and sepsis have been reported one case respectively. Onset of ADE whose causality with this drug cannot be excluded was suicide attempt that has been reported one case.
Onset of unexpected AE was 0.39% (n: 19/4896, 20 cases), including constipation, palpitation, aphasia, dyskinesia, impulsive act, psychomotor retardation, edema, cheilitis, abdominal distension, GI disorder, salivation, urticaria, sepsis, Musculoskeletal stiffness, neck pain, urinary frequency and dyspnea have been reported.
View ADR Monitoring Form