Ketorolac trometamol 30 mg/mL solution for IM/IV Injection is a clear, colourless or light-yellow solution practically free from particles.
Each mL contains: Ketorolac Trometamol 30 mg.
Pharmacology: Pharmacodynamics: Mechanism of action: Ketorolac trometamol is a nonsteroidal anti-inflammatory drug (NSAID) chemically related to indomethacin and tolmetin. Ketorolac tromethamol is a racemic mixture of [-]S- and [+]R-enantiomeric forms, with the S-form having analgesic activity. Its anti-inflammatory effects are believed to be due to inhibition of both cylooxygenase-1 (COX-1) and cylooxygenase-2 (COX-2) which leads to the inhibition of prostaglandin synthesis leading to decreased formation of precursors of prostaglandins and thromboxanes from arachidonic acid. The resultant reduction in prostaglandin synthesis and activity may be at least partially responsible for many of the adverse, as well as the therapeutic, effects of these medications. Analgesia is probably produced via a peripheral action in which blockade of pain impulse generation results from decreased prostaglandin activity. However, inhibition of the synthesis or actions of other substances that sensitize pain receptors to mechanical or chemical stimulation may also contribute to the analgesic effect. In terms of the ophthalmic applications of ketorolac trometamol - ocular administration of ketorolac trometamol reduces prostaglandin E2 levels in aqueous humor, secondary to inhibition of prostaglandin biosynthesis.
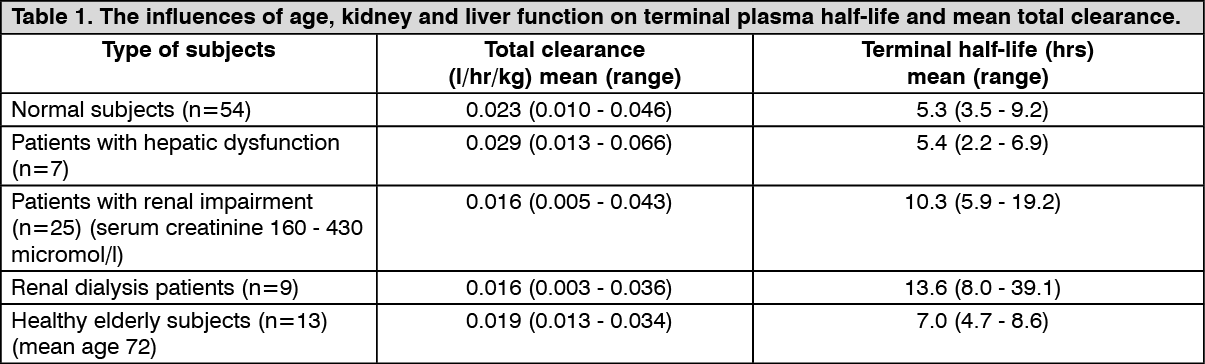
Pharmacokinetics: Following intramuscular administration, ketorolac trometamol was rapidly and completely absorbed, a mean peak plasma concentration of 2.2 mcg/mL occurring an average of 50 minutes after a single 30 mg dose. The influences of age, kidney and liver function on terminal plasma half-life and mean total clearance are outlined in the table as follows (estimated from a single 30 mg IM dose of ketorolac trometamol). (See Table 1.)
 Click on icon to see table/diagram/image
Absorption:
Click on icon to see table/diagram/image
Absorption: Rapidly and completely absorbed after parenteral administration. Ketorolac trometamol is fragmented to from anionic ketorolac molecule less hydrophilic than trometamol salt in physiological pH. Ketorolac is absorbed slower in parenteral form. More than 99% of ketorolac in plasma is protein bound. The terminal plasma half-life of ketorolac is approximately in the range of 4-6 hours. In the elderly, the mean terminal plasma half-life of ketorolac trometamol increases from 6-7 hours compared with young health volunteers (based on single dose data). The mean half-life of ketorolac trometamol in renally-impaired patients is between 9-10 hours and is dependent on the extent of the impairment (based on single dose data).
Distribution: The mean apparent volume (V
β) of ketorolac trometamol following complete distribution is approximately 13 litres (this parameter was determined from single dose data). More than 99% of ketorolac in plasma is protein bound. Even at high plasma concentrations (10 µg/mL) only approximately 5% of albumin binding sites will be occupied. Thus, the unbound fraction for each enantiomer will be constant over the therapeutic range. A decrease in serum albumin, however, will result in increased free drug concentrations. Ketorolac trometamol is excreted via human milk.
The effect of plasma dilution on free ketorolac was consistent across all volume expanders tested and for each ketorolac concentration studied. Because of the pharmacokinetic properties of ketorolac, this pharmacokinetic interaction can be expected to have only minor effects on unbound ketorolac concentrations when ketorolac is administered after the plasma expander. When ketorolac administration is followed by rapid plasma expander infusion, a transient increase of unbound ketorolac in plasma can be expected. A single dose of racemic ketorolac (30 mg of tromethamine salt) was administered by bolus intramuscular injection to four young, healthy volunteers. The concentrations of total (bound plus unbound) (R)- and (S)-ketorolac were measured in plasma for 9 h after dosing. The mean +/- s.d. clearance of (S)-ketorolac (45.9 +/- 10.1 mL h-1 kg-1) exceeded (P = 0.0032) that of the (R)-enantiomer (19.0 +/- 5.0 mL h-1 kg-1). The mean +/- s.d. AUC ratio for (S)-ketorolac:(R)-ketorolac (0.442 +/- 0.043) was significantly different from unity (P = 0.0001). The steady-state volume of distribution of (S)-ketorolac (0.135 +/- 0.022 l kg-1) was significantly different (P = 0.0013) from that of its optical antipode (0.075 +/- 0.014 l kg-1) and the half-lives of (S)- and (R)-ketorolac (2.35 +/- 0.23 h and 3.62 +/- 0.79 h, respectively) were also significantly different (P = 0.026). These data indicate that the disposition of ketorolac in man is subject to marked enantioselectivity and, because of possible differences in biological activity of (S)- and (R)-ketorolac, emphasize the need to monitor separate stereoisomer concentrations of the drug if pharmacological data are to be interpreted correctly. (See figure.)
Click on icon to see table/diagram/image
The protein binding of ketorolac and midazolam, individually and in combination, were determined in (1) human serum, (2) human albumin solution, and (3) human alpha
1-acid glycoprotein solution using ultrafiltration technology. The in vitro data derived in this study suggest that when present together, neither midazolam nor ketorolac influences the overall extent of protein binding of the other. Results are shown in Table as follows. (See Table 2.)
Click on icon to see table/diagram/image
Metabolism: Ketorolac Tromethamol is largely metabolized in the liver. The metabolic products are hydroxylated and conjugated forms of the parent drug. The products of metabolism, and some unchanged drug, are excreted in the urine. Its metabolism is primarily hepatic. Less than 50% of a dose is metabolized. The major metabolites are a glucuronide conjugate, which may also be formed in the kidney, and p-hydroxy ketorolac. Neither metabolite has significant analgesic activity.
Elimination: The principal route of elimination of ketorolac trometamol and its metabolites is renal. About 92% of a given dose is found in the urine, approximately 40% as metabolites and 60% as unchanged ketorolac. Approximately 6% of a dose is excreted in the feces. A single-dose study with 10 mg ketorolac trometamol (n=9) demonstrated that the S-enantiomer is cleared approximately two times faster than the R-enantiomer and that the clearance was independent of the route of administration. This means that the ratio of S/R plasma concentrations decreases with time after each dose. There is little or no inversion of the R- to S-form in humans.
Ketorolac trometamol (KETOVEX-30) is indicated for the short-term management of moderate to severe acute postoperative pain.
KETOVEX-30 is for administration by intramuscular or bolus intravenous injection. Bolus intravenous doses should be given over no less than 15 seconds. KETOVEX-30 should not be used for epidural or spinal administration.
The time to onset of analgesic effect following both IV and IM administration is similar and is approximately 30 minutes, with maximum analgesia occurring within one to two hours. The median duration of analgesia is generally four to six hours.
Dosage should be adjusted according to the severity of the pain and the patient response.
The administration of continuous multiple daily doses of ketorolac trometamol intramuscularly or intravenously should not exceed two days because adverse events may increase with prolonged usage. There has been limited experience with dosing for longer periods since the vast majority of patients have transferred to oral medication, or no longer require analgesic therapy after this time.
Undesirable effects may be minimised by using the lowest effective dose for the shortest duration necessary to control symptoms.
Adults: The recommended initial dose of KETOVEX-30 is 10 mg, followed by 10 to 30 mg every four to six hours as required. In the initial post-operative period, KETOVEX-30 may be given as often as every two hours if needed. The lowest effective dose should be given. A total daily dose of 90 mg for non-elderly and 60 mg for the elderly, renally-impaired patients and patients less than 50 kg should not be exceeded. The maximum duration of treatment should not exceed two days. Reduce dosage in patients under 50 kg.
Opioid analgesics (e.g. morphine, pethidine) may be used concomitantly, and may be required for optimal analgesic effect in the early post-operative period when pain is most severe. Ketorolac does not interfere with opioid binding and does not exacerbate opioid-related respiratory depression or sedation. When used in association with KETOVEX-30 IM/IV, the daily dose of opioid is usually less than that normally required. However, opioid side-effects should still be considered, especially in day-case surgery.
For patients receiving parenteral ketorolac, and who are converted to ketorolac oral tablets, the total combined daily dose should not exceed 90 mg (60 mg for the elderly, renally-impaired patients and patients less than 50 kg) and the oral component should not exceed 40 mg on the day the change of formulation is made. Patients should be converted to oral treatment as soon as possible.
Elderly: The elderly are at increased risk of the serious consequences of adverse reactions. If an NSAID is considered necessary, the lowest effective dose should be used and for the shortest possible duration. The patient should be monitored regularly for GI bleeding during NSAID therapy.
A total daily dose of 60 mg should not be exceeded.
Children: Safety and efficacy in children have not been established. Therefore, KETOVEX-30 is not recommended for use in children under 16 years of age.
Ketorolac trometamol is contraindicated in patients with previously demonstrated hypersensitivity to ketorolac, any of its excipients, or other NSAIDs and patients in whom aspirin or other prostaglandin synthesis inhibitors induce allergic reactions (severe anaphylactic-like reactions have been observed in such patients). Such reactions have included asthma, rhinitis, angioedema, or urticaria.
Ketorolac trometamol is also contraindicated in those with a history of asthma, children under 16 years of age.
Ketorolac trometamol is contraindicated in patients with active peptic ulcer, or any history of gastrointestinal bleeding, ulceration or perforation.
As with other NSAIDs, ketorolac trometamol is contraindicated in patients with severe heart failure, hepatic failure and renal failure.
Ketorolac trometamol is contraindicated in patients with moderate or severe renal impairment (serum creatinine >160 µmol/L) or in patients at risk for renal failure due to volume depletion or dehydration.
Ketorolac trometamol is contraindicated in pregnancy, labour, delivery or lactation.
Ketorolac trometamol is contraindicated as prophylactic analgesia before surgery due to inhibition of platelet aggregation and is contraindicated intra-operatively because of the increased risk of bleeding.
Ketorolac trometamol inhibits platelet function and is, therefore, contraindicated in patients with suspected or confirmed cerebrovascular bleeding, patients who have had operations with a high risk of haemorrhage or incomplete haemostasis and those at high risk of bleeding such as those with haemorrhagic diatheses, including coagulation disorders.
It is also contraindicated in patients on anticoagulants, including warfarin and low dose heparin (2500-5000 units 12 hourly).
Ketorolac trometamol is contraindicated in patients currently receiving ASA or other NSAIDs (including cyclooxygenase-2 selective inhibitors).
Ketorolac Trometamol Solution for injection is contraindicated for neuraxial (epidural or intrathecal) administration due to its alcohol content.
The combination of ketorolac with oxpentifylline is contraindicated.
Concurrent treatment with ketorolac and probenecid or lithium salts is contraindicated.
Ketorolac trometamol is contraindicated in patients with the complete or partial syndrome of nasal polyps, angioedema or bronchospasm.
Ketorolac trometamol: Epidemiological evidence suggests that ketorolac may be associated with a high risk of serious gastrointestinal toxicity, relative to some other NSAIDs, especially when used outside the licensed indications and/or for prolonged periods.
Physicians should be aware that in some patients pain relief may not occur until upwards of 30 minutes after IV or IM administration.
The use of ketorolac trometamol with concomitant NSAIDs including cyclooxygenase-2 selective inhibitors should be avoided.
Undesirable effects may be minimised by using the minimum effective dose for the shortest duration necessary to control symptoms.
KETOVEX-30 is essentially 'sodium free' as it contains less than 1 mmol sodium (23 mg per 1 mL).
This medicinal product contains ethanol (alcohol) 10% of volume, for example, 100 mg in each dose, such as equivalent to 2 mL beer in each dose, equivalent to 0.8 mL wine in each dose. This medicinal product can be dangerous for patients having alcoholism. Should be considered for pregnant or nursing mothers, children or patients with hepatopathy or patient with high risk of epilepsy.
Gastrointestinal ulceration, bleeding and perforation: GI bleeding, ulceration or perforation, which can be fatal, has been reported with all NSAIDs including ketorolac trometamol therapy, at anytime during treatment, with or without warning symptoms or a previous history of serious GI events.
In a non-randomised, in-hospital post-marketing surveillance study, increased rates of clinically serious GI bleeding were seen in patients <65 years of age who received an average daily dose of >90 mg ketorolac IM as compared to those patients receiving parenteral opioids.
The elderly have an increased frequency of adverse reactions to NSAIDs, especially gastrointestinal bleeding and perforation which may be fatal.
The risk of GI bleeding, ulceration or perforation is higher with increasing NSAID doses, including ketorolac trometamol IV, in patients with a history of ulcer, particularly if complicated with haemorrhage or perforation, and in the elderly. The risk of clinically serious gastrointestinal bleeding is dose dependent. These patients should commence treatment on the lowest dose available. Combination therapy with protective agents (e.g. misoprostol or proton pump inhibitors) should be considered for these patients, and also for patients requiring concomitant low dose aspirin, or other drugs likely to increase gastrointestinal risk. This age-related risk of gastrointestinal bleeding and perforation is common to all NSAIDs. Compared to young adults, the elderly have an increased plasma half-life and reduced plasma clearance of ketorolac. A longer dosing interval is advisable.
NSAIDs should be given with care to patients with a history of inflammatory bowel disease, (ulcerative colitis, Crohn's disease) as these conditions may be exacerbated. Patients with a history of GI toxicity, particularly when elderly, should report any unusual abdominal symptoms (especially GI bleeding) particularly in the initial stages of treatment. When GI bleeding or ulceration occurs in patients receiving ketorolac trometamol IV, treatment should be withdrawn.
Caution should be advised in patients receiving concomitant medications which could increase the risk of ulceration or bleeding, such as oral corticosteroids, selective serotonin-reuptake inhibitors or anti-platelet agents such as aspirin. Use in patients taking anticoagulants such as warfarin is contraindicated.
As with other NSAIDs the incidence and severity of gastrointestinal complications may increase with increasing dose and duration of treatment with ketorolac trometamol IV. The risk of clinically serious gastrointestinal bleeding is dose-dependent. This is particularly true in elderly patients who receive an average daily dose greater than 60 mg/day of ketorolac trometamol IV. A history of peptic ulcer disease increases the possibility of developing serious gastrointestinal complications during ketorolac trometamol therapy.
Haematological effects: Patients with coagulation disorders should not receive ketorolac trometamol (KETOVEX-30). Patients on anticoagulation therapy may be at increased risk of bleeding if given ketorolac trometamol (KETOVEX-30) concurrently. The concomitant use of ketorolac and prophylactic low dose heparin (2500-5000 units 12-hourly) and dextrans has not been studied extensively and may also be associated with an increased risk of bleeding. Patients already on anticoagulants or who require low-dose heparin should not receive ketorolac trometamol. Patients who are receiving other drug therapy that interferes with haemostasis should be carefully observed if ketorolac trometamol (KETOVEX-30) is administered. In controlled clinical studies, the incidence of clinically significant postoperative bleeding was less than 1%.
Ketorolac trometamol inhibits platelet aggregation and prolongs bleeding time. In patients with normal bleeding function, bleeding times were raised, but not outside the normal range of two to eleven minutes. Unlike the prolonged effects from aspirin, platelet function returns to normal within 24 to 48 hours after ketorolac trometamol is discontinued.
In post-marketing experience, postoperative wound haemorrhage has been reported in association with the peri-operative use of ketorolac trometamol IM/IV. Therefore, ketorolac trometamol should not be used in patients who have had operations with a high risk of haemorrhage or incomplete haemostasis. Caution should be used where strict haemostasis is critical, e.g. in cosmetic or day-case surgery, resection of the prostate or tonsillectomy. Haematomas and other signs of wound haemorrhage and epistaxis have been reported with the use of ketorolac trometamol. Physicians should be aware of the pharmacological similarity of ketorolac to other non-steroidal anti-inflammatory drugs that inhibit cyclo-oxygenase and the risk of bleeding, particularly in the elderly.
Skin reactions: Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome, and toxic epidermal necrolysis, have been reported very rarely in association with the use of NSAIDs. Patients appear to be at highest risk for these reactions early in the course of therapy: the onset of the reactions occurring in the majority of cases within the first month of treatment. Ketorolac trometamol (KETOVEX-30) should be discontinued at the first appearance of skin rash, mucosal lesions, or any other sign of hypersensitivity.
SLE and mixed connective tissue disease: In patients with systemic lupus erythematosus (SLE) and mixed connective tissue disorders there may be an increased risk of aseptic meningitis.
Sodium/fluid retention in cardiovascular conditions and peripheral oedema: Caution is required in patients with a history of hypertension and/or heart failure as fluid retention and oedema have been reported in association with NSAID therapy.
Fluid retention, hypertension and peripheral oedema has been observed in some patients taking NSAIDs including ketorolac trometamol and it should therefore be used with caution in patients with cardiac decompensation, hypertension or similar conditions.
Cardiovascular and cerebrovascular effects: Appropriate monitoring and advice are required for patients with a history of hypertension and/or mild to moderate congestive heart failure as fluid retention and oedema have been reported in association with NSAID therapy.
Clinical trial and epidemiological data suggest that use of coxibs and some NSAIDs (particularly at high doses) may be associated with a small increased risk of arterial thrombotic events (for example myocardial infarction or stroke). Although ketorolac trometamol has not been shown to increase thrombotic events such as myocardial infarction, there are insufficient data to exclude such a risk for ketorolac trometamol.
Patients with uncontrolled hypertension, congestive heart failure, established ischaemic heart disease, peripheral arterial disease, and/or cerebrovascular disease should only be treated with ketorolac trometamol after careful consideration. Similar consideration should be made before initiating treatment of patients with risk factors for cardiovascular disease (e.g. hypertension, hyperlipidaemia, diabetes mellitus and smoking).
Cardiovascular, Renal and Hepatic Impairment: Caution should be observed in patients with conditions leading to a reduction in blood volume and/or renal blood flow, where renal prostaglandins have a supportive role in the maintenance of renal perfusion. In these patients, administration of an NSAID may cause a dose-dependent reduction in renal prostaglandin formation and may precipitate overt renal failure. Patients at greatest risk of this reaction are those who are volume depleted because of blood loss or severe dehydration, patients with impaired renal function, heart failure, liver dysfunction, the elderly and those taking diuretics. Renal function should be monitored in these patients. Discontinuation of NSAID therapy is typically followed by recovery to the pre-treatment state. Inadequate fluid/blood replacement during surgery, leading to hypovolaemia, may lead to renal dysfunction which could be exacerbated when ketorolac trometamol (KETOVEX-30) is administered. Therefore, volume depletion should be corrected and close monitoring of serum urea and creatinine and urine output is recommended until the patient is normovolaemic. In patients on renal dialysis, ketorolac clearance was reduced to approximately half the normal rate and terminal half-life increased approximately three-fold.
Renal effects: As with other NSAIDs ketorolac trometamol should be used with caution in patients with impaired renal function or a history of kidney disease because it is a potent inhibitor of prostaglandin synthesis. Caution should be observed as renal toxicity has been seen with ketorolac trometamol and other NSAIDs in patients with conditions leading to a reduction in blood volume and/or renal blood flow where renal prostaglandins have a supportive role in the maintenance of renal perfusion.
In these patients administration of ketorolac trometamol or other NSAIDs may cause a dose-dependent reduction in renal prostaglandin formation and may precipitate overt renal decompensation or failure. Patients at greatest risk of this reaction are those with impaired renal function, hypovolaemia, heart failure, liver dysfunction, those taking diuretics and the elderly. Discontinuation of ketorolac trometamol or other non-steroidal anti-inflammatory therapy is usually followed by recovery to the pre-treatment state.
As with other drugs that inhibit prostaglandin synthesis, elevations of serum urea, creatinine and potassium have been reported with ketorolac trometamol and may occur after one dose.
Patients with impaired renal function: Since ketorolac trometamol and its metabolites are excreted primarily by the kidney, patients with moderate to severe impairment of renal function (serum creatinine greater than 160 micromol/L) should not receive ketorolac trometamol (KETOVEX 30). Patients with lesser renal impairment should receive a reduced dose of ketorolac trometamol (not exceeding 60 mg/day IM or IV) and their renal status should be closely monitored.
Use in patients with impaired liver function: Patients with impaired hepatic function from cirrhosis do not have any clinically important changes in ketorolac trometamol clearance or terminal half-life.
Borderline elevations of one or more liver function tests may occur. These abnormalities may be transient, may remain unchanged, or may progress with continued therapy. Meaningful elevations (greater than 3 times normal) of serum glutamate pyruvate transaminase (SGPT/ALT) or serum glutamate oxaloacetate transaminase (SGOT/AST) occurred in controlled clinical trials in less than 1% of patients. If clinical signs and symptoms consistent with liver disease develop, or if systemic manifestations occur, ketorolac trometamol (KETOVEX 30) should be discontinued.
Anaphylactic (anaphylactoid) reactions: Anaphylactic (anaphylactoid) reactions (including, but not limited to, anaphylaxis, bronchospasm, flushing, rash, hypotension, laryngeal oedema and angioedema) may occur in patients with or without a history of hypersensitivity to aspirin, other NSAIDs or ketorolac trometamol IV. These may also occur in individuals with a history of angioedema, bronchospastic reactivity (e.g. asthma) and nasal polyps. Anaphylactoid reactions, like anaphylaxis, may have a fatal outcome. Therefore, ketorolac should not be used in patients with a history of asthma and in patients with the complete or partial syndrome of nasal polyps, angioedema and bronchospasm.
Fluid retention and oedema: Fluid retention, hypertension and oedema have been reported with the use of ketorolac trometamol and it should therefore be used with caution in patients with cardiac decompensation, hypertension or similar conditions.
Caution is advised when methotrexate is administered concurrently since some prostaglandin synthesis-inhibiting drugs have been reported to reduce the clearance of methotrexate, and thus possibly enhance its toxicity.
Drug Abuse and Dependence: Ketorolac trometamol is devoid of addictive potential. No withdrawal symptoms have been observed following abrupt discontinuation of ketorolac IV.
Use in Pregnancy & Lactation: See Use in Pregnancy & Lactation section for further information.
Use in Children: Ketorolac tablets are not recommended for use in children. Ketorolac trometamol given parenterally is not recommended in children younger than 2 years of age.
Pregnancy category: C.
Pregnancy: The safety of ketorolac trometamol (KETOVEX 30) during human pregnancy has not been established. There was no evidence of teratogenicity in rats or rabbits studied at maternally-toxic doses of ketorolac. Prolongation of the gestation period and/or delayed parturition were seen in the rat. Congenital abnormalities have been reported in association with NSAID administration in man, however these are low in frequency and do not follow any discernible pattern. In view of the known effects of NSAIDs on the foetal cardiovascular system (risk of closure of the ductus arteriosus) ketorolac is contraindicated during pregnancy, labour or delivery.
Labour and Delivery: Ketorolac trometamol is contraindicated in labour and delivery because, through its prostaglandin synthesis inhibitory effect it may adversely affect foetal circulation and inhibit uterine contractions, thus increasing the risk of uterine haemorrhage.
There may be increased bleeding tendency in both mother and child.
Nursing Mothers: Ketorolac trometamol and its metabolites have been shown to pass into the foetus and milk of animals. Ketorolac has been detected in human milk at low concentrations, therefore ketorolac trometamol is contraindicated in mothers who are breast-feeding.
Precautions related to fertility: The use of ketorolac trometamol (KETOVEX-30), as with any drug known to inhibit cyclooxygenase/prostaglandin synthesis, may impair fertility and is not recommended in women attempting to conceive. In women who have difficulty conceiving or are undergoing investigation of fertility, withdrawal of ketorolac trometamol (KETOVEX-30) should be considered.
Protein Binding: Ketorolac tromethamine is highly bound to human plasma protein (mean 99.2%) and binding is independent of concentration. As ketorolac tromethamine is a highly potent drug and present in low concentrations in plasma, it would not be expected to displace other protein-bound drugs significantly. Therapeutic concentrations of digoxin, warfarin, acetaminophen, phenytoin, and tolbutamide did not alter ketorolac tromethamine protein binding.
Anticoagulant Therapy: Numerous studies have shown that the concomitant use of NSAIDs and anticoagulants increases the risk of GI adverse events such as ulceration and bleeding. Because prostaglandins play an important role in hemostasis, and NSAIDs affect platelet function, concurrent therapy of Ketorolac Tromethamol with warfarin requires close monitoring to be certain that no change in anticoagulant dosage is necessary.
Prothrombin time should be carefully monitored in patients receiving oral anticoagulant therapy concomitantly with Ketorolac Tromethamol.
Ketorolac trometamol given with two doses of 5000 U of heparin to 11 healthy volunteers, resulted in a mean template bleeding time of 6.4 min (3.2-11.4 min) compared to a mean of 6.0 min (3.4-7.5 min) for heparin alone and 5.1 min (3.5-8.5 min) for placebo.
The in vitro binding of warfarin to plasma proteins is only slightly reduced by ketorolac tromethamol (99.5% control vs. 99.3%) at plasma concentrations of 5 to 10 μg/mL.
Digoxin: Ketorolac tromethamol does not alter digoxin protein binding.
Salicylates or Other NSAIDs: The use of ketorolac trometamol in addition to any other NSAID, including those over the counter ones (such as ASA and Ibuprofen) is contraindicated due to the possibility of additive side effects.
In vitro studies indicated that, at therapeutic concentrations of salicylates (300 μg/mL), the binding of ketorolac tromethamine was reduced from approximately 99.2% to 97.5% representing a potential two-fold increase in unbound ketorolac plasma levels.
Glucocorticoids: Numerous studies have shown that the concomitant use of NSAIDs and oral glucocorticoids increases the risk of GI side effects such as ulceration and bleeding. This is especially the case in older (>65 years of age) individuals.
Enzyme Induction: There is no evidence, in animal or human studies, that ketorolac tromethamine induces or inhibits the hepatic enzymes capable of metabolizing itself or other drugs. Hence, it would not be expected to alter the pharmacokinetics of other drugs due to enzyme induction or inhibition mechanisms.
Probenecid: Concomitant administration of ketorolac tromethamine and probenecid results in the decreased clearance of ketorolac and a significant increase in ketorolac plasma levels (approximately three-fold increase) and terminal half-life (approximately two-fold increase). The concomitant use of Ketorolac Tromethamine injection and probenecid is, therefore, contraindicated.
Furosemide: Ketorolac tromethamine reduces the diuretic response to furosemide by approximately 20% in normovolemic subjects, so particular care should be taken in patients with cardiac decompensation.
Lithium: Some NSAIDs have been reported to inhibit renal lithium clearance, leading to an increase in plasma lithium concentrations and potential lithium toxicity. The effect of ketorolac tromethamine on lithium plasma levels has not been studied. Cases of increased lithium plasma concentrations during ketorolac therapy have been reported.
Methotrexate: The concomitant administration of methotrexate and some NSAIDs has been reported to reduce the clearance of methotrexate, thus enhancing its toxicity.
ACE Inhibitors: Concomitant use of ACE inhibitors and other NSAIDs may increase the risk of renal impairment, particularly in volume depleted patients.
Morphine: Intramuscular ketorolac tromethamine has been administered concurrently with morphine in several clinical trials of postoperative pain without evidence of adverse interactions.
Store at temperatures not exceeding 30°C.
M01AB15 - ketorolac ; Belongs to the class of acetic acid derivatives and related substances of non-steroidal antiinflammatory and antirheumatic products.
Ketovex-30 soln for inj 30 mg/mL
5 × 1's (P98/ampoule)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image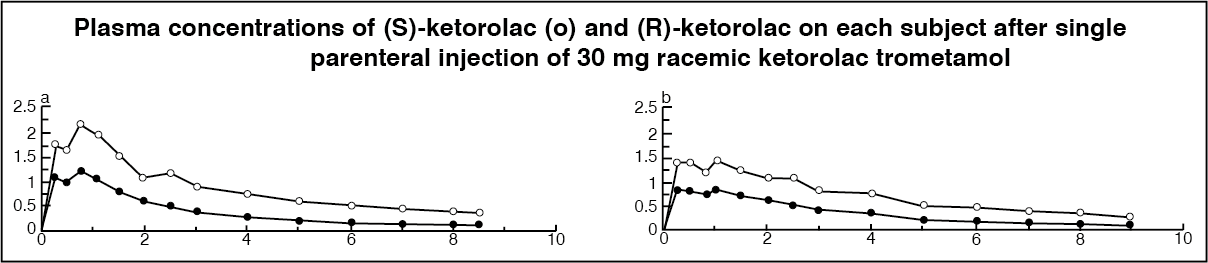 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image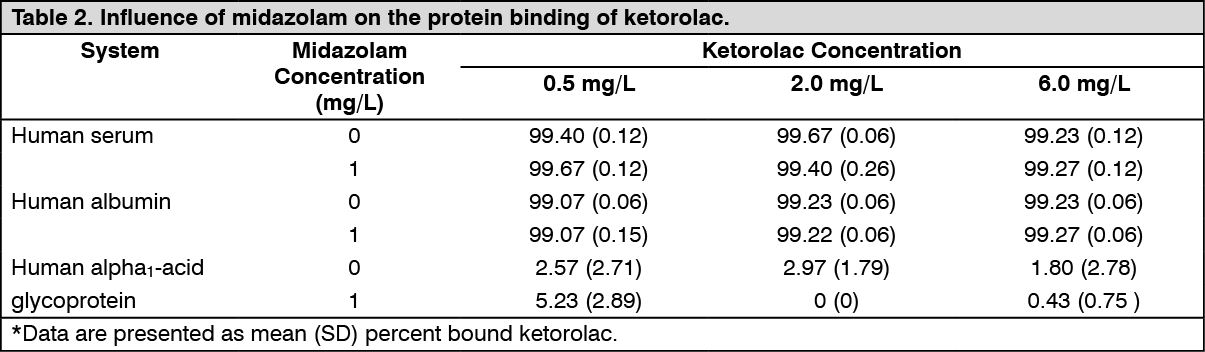 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out