Each film coated tablet contains: Clarithromycin 500 mg.
Pharmacology: Pharmacodynamics: Mechanism of Action: Clarithromycin exerts its antibacterial action by binding to the 50S ribosomal sub-unit of susceptible microorganisms resulting in inhibition of protein synthesis.
Pharmacokinetics: Adsorption and Fate: Clarithromycin is rapidly absorbed from the gastrointestinal tract after oral administration. The absolute bioavailability of 500 mg clarithromycin tablets was approximately 50%. Food slightly delays both the onset of clarithromycin absorption and the formation of the antimicrobially active metabolite, 14-OH clarithromycin, but does not affect the extent of bioavailability.
Aerobic Gram-Positive Microorganism: Staphylococcus aureus, Streptococcus pneumoniae, Streptococcus pyrogens.
Aerobic Gram-negative Microorganisms: Haemophilus Influenzae, Moraxella catarrhalis.
Other Microorganism: Mycoplasma pneumoniae, Chlamydia pneumoniae (TWAR).
Mycobacteria: Mycobacterium avium complex(MAC) consisting of: Mycobacterium avium, Mycobacterium intracellulare.
Beta lactamase production should have no effect on clarithromycin activity.
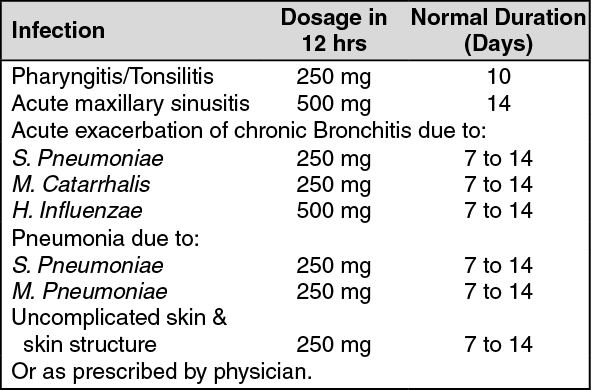
(See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Clarithromycin is contraindicated in patients with a known hypersensitivity to clarithromycin, erythromycin, or any macrolide antibiotics.
Concominant administration of clarithromycin with cisapride, pimozide or terfenadine is contraindicated. There have been post-marketing reports of drug interactions when clarithromycin and/or erythromycin are co-administered with cisapride, pimozide, or terfenadine resulting in cardiac arrythmias (QT prolongation, ventricular tachycardia, ventricular fibrillation, and torsades de pointes) most likely due to inhibition of hepatic metabolism of these drugs by erythromycin and clarithromycin. Fatalities have been reported.
Clarithromycin should not be used in pregnant women except in clinical circumstances where no alternative therapy is appropriate. If pregnancy occurs while taking this drug, the patient should be apprised of the potential hazard to the fetus. Clarithromycin has demonstrated adverse effects of pregnancy outcome and/or embryo-fetal development in monkeys, rats, mice, and rabbits at doses that produced plasma levels 2 to 17 times. The serum levels achieved in humans treated at the maximum recommended human doses.
Pseudomembranous colitis has been with nearly all antibacterial agents, including clarithromycin and may range in severity from mild to life-threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhea subsequent to the administration of antibacterial agents.
Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of clostridia. Studies indicate that a toxin produced by clostridium difficile is a primary cause of "antibiotic-associated colitis".
After the diagnosis of pseudomembranous colitis has been established, therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to discontinuation of the drug alone. In moderate to severe cases, consideration should be given to management with fluids and electrolytes, protein supplementation, and treatment with antibacterial drug clinically effective against Clostridium difficile colitis.
This product contains TARTRAZINE (FDC Yellow #5) which can cause allergic reactions such as angioedema, asthma, urticaria and anaphylactic shock. Some of the reports have dealt with cross-sensitivity, especially with aspirin, although the connection with aspirin has been questioned.
Clarithromycin is principally excreted via the liver and kidney. Clarithromycin may be administered without dosage adjustment to patients with hepatic impairment and normal renal function. However, in the presence of severe renal impairment with or without coexisting hepatic impairment, decreased dosage or prolonged dosing intervals may be appropriate.
Clarithromycin should not be used in pregnant women except in clinical circumstances where no alternative therapy is appropriate. If pregnancy occurs while taking this drug, the patient should be apprised of the potential hazard to the fetus. Clarithromycin has demonstrated adverse effects of pregnancy outcome and/or embryo-fetal development in monkeys, rats, mice, and rabbits at doses that produced plasma levels 2 to 17 times. The serum levels achieved in humans treated at the maximum recommended human doses.
Fewer than 3% of adult patients without mycobacterial infections and fewer than 2% of pediatric patients without mycobacterial infections also discontinued therapy because of drug-related side effects.
The most frequent reported events in adults were diarrhea (3%), nausea (3%), abnormal taste (3%), dyspepsia (2%), abdominal pain/discomfort (2%) and headache (2%). In pediatric patients, the most frequently reported events were diarrhea (6%), abdominal pain (3%), rash (3%) and headache (2%). Most of these were described as mild or moderate in severity. Of the reported adverse events, only 1% was described as severe.
In pneumonia studies conducted in adult comparing clarithromycin-treated patients compared to erythromycin-treated patients (13% vs 32%; p<0.01).
Clarithromycin use in patients who are receiving theophylline may be associated with an increase of serum theophylline concentrations. Monitoring of serum theophylline concentrations should be considered for patients receiving high doses of theophylline or with baseline concentrations in the upper therapeutic range. In two studies in which theophylline was administered with clarithromycin (a theophylline sustained-release formulation was dosed at either 6.5 mg/kg or 12 mg/kg together with 250 or 500 mg every 12h clarithromycin), the steady-state levels of Cmax, Cmin, and the area under the serum concentration time curve (AUC) of theophylline increased about 20%.
Concominant administration of single doses of clarithromycin and carbamazepine has been shown to result in increased plasma concentration of carbamazepine. Blood level monitoring of carbamazepine may be considered.
When clarithromycin and terfenadine were co-administered, plasma concentrations of the active metabolite of terfenadine were threefold higher, on average, than the values observed when terfenadine was administered alone. The pharmacokinetics of clarithromycin and the 14-hydroxy-clarithromycin were not significantly affected by the co-administration of terfenadine once clarithromycin reached steady state conditions. Concominant administration of clarithromycin with terfenadine is contraindicated. (See Contraindications).
Clarithromycin 500 mg every 8 hours was given in combination with omeprazole 40 mg daily to healthy adult subjects. The steady state plasma concentrations of omeprazole was increased (Cmax, AUC0-24 and T1/2 increases of 30%, 89% and 34%, respectively), by the concominant administration of clarithromycin. The mean 24 hour gastric pH value was 5.2 when omeprazole was administered alone and 5.7 when co-administered with clarithromycin.
Co-administration of clarithromycin with ranitidine, bismuth citrate resulted in increased plasma ranitidine concentrations (57%), increased plasma bismuth trough concentrations (48%) and increased 14-hydroxy-clarithromycin plasma concentrations (31%). These effects are clinically significant.
Simultaneous oral administration of clarithromycin and zidovudine to HIV infected adult patients resulted in decreased steady state zidovudine. When 500 mg of clarithromycin were administered twice daily, steady state zidovudine AUC was reduced by a mean of 12% (n=4). Individuals values ranged from a decrease of 34% to an increase of 14%. Based on limited data in 24 patients, when clarithromycin was administered 2 to 4 hours prior to oral zidovudine, the steady-state zidovudine Cmax was increased by approximately 2-folds, whereas the AUC was unaffected.
Simultaneous administration of clarithromycin and didanosine to 12 HIV infected adult patients resulted in no statistically significant change in didanosine pharmacokinetics.
Concominant administration of fluconazole 200 mg daily and clarithromycin 500 mg twice a daily to 21 healthy volunteers led to increases in the mean steady state clarithromycin Cmin and AUC of 33% and 18%, respectively. Steady-state concentrations of 14-OH clarithromycin were not significantly affected by concominant administration of fluconazole.
Store at a temperature not exceeding 30°C.
J01FA09 - clarithromycin ; Belongs to the class of macrolides. Used in the systemic treatment of infections.
Klarimed FC tab 500 mg
30's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out