If a dose is missed and cannot be taken within 12 hours, then that dose should be skipped and the next dose should be taken at the usual time of administration.
Treatment should continue as long as there is clinical benefit.
Optimal medical management for nausea, vomiting, and/or diarrhea should be initiated prior to any lenvatinib therapy interruption or dose reduction; however, gastrointestinal toxicity should be actively managed in order to reduce the risk of development of renal impairment or renal failure.
Management of some adverse reactions may require dose interruption, adjustment (modification), or discontinuation of lenvatinib therapy. Mild to moderate adverse reactions (eg., Grade 1 or 2) generally do not warrant interruption of lenvatinib unless intolerable to the patient despite optimal management. Severe (e.g., Grade 3) or intolerable adverse reactions until improvement of the reaction to Grade 0-1 or baseline, followed by dose reduction of lenvatinib once resumed.
Treatment should be discontinued in case of life-threatening reactions (eg., Grade 4) with the exception of laboratory abnormality judged to be non-life-threatening, in which case they should be managed as severe reactions (eg, Grade 3). For asymptomatic laboratory abnormalities, such as Grade >3 elevations of amylase and lipase that are not considered clinically relevant, lenvatinib continuation without dose modification may be considered. Grades are based on the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE).
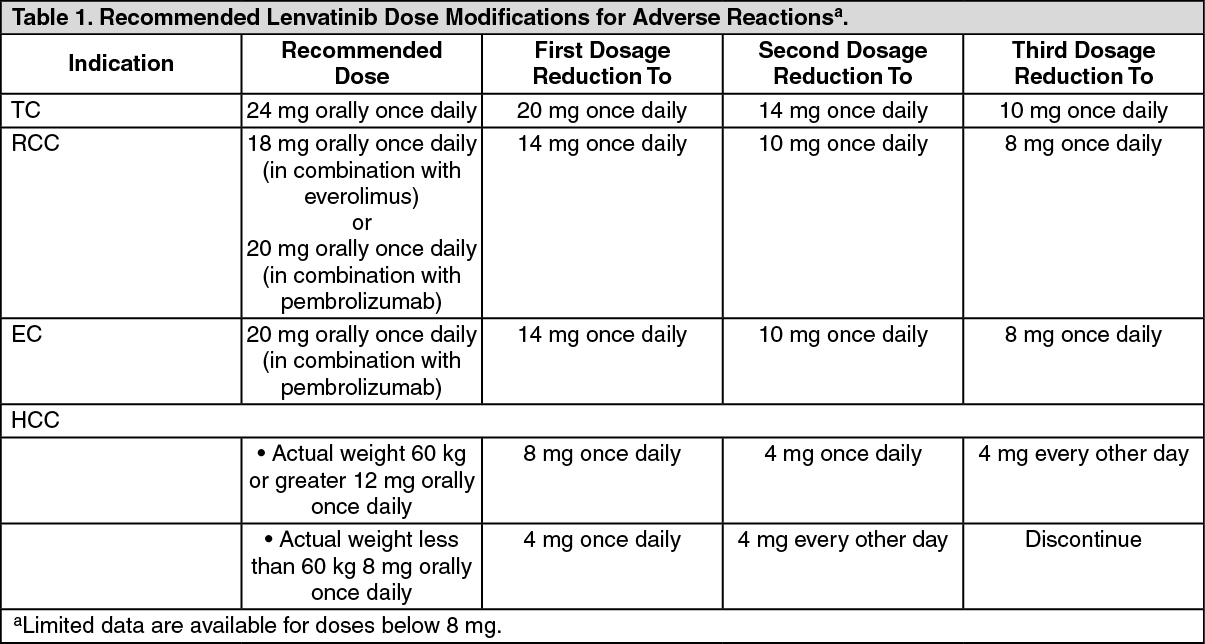
Specific recommendations for dose modification due to adverse reactions are provided as follows in Table 1, following specific information for each indication.
Posology: Thyroid Cancer:
Initial dose regimen: The recommended starting daily dose of lenvatinib is 24 mg (two 10 mg capsules and one 4 mg capsule) taken once daily.
Monitoring and dose modification and discontinuation: For lenvatinib-related toxicities, upon resolution/improvement of an adverse reaction, treatment should be resumed at a reduced dose as suggested in Table 1. (See Table 1.)
Renal Cell Carcinoma: Lenvatinib in combination with pembrolizumab.
Refer to the pembrolizumab prescribing information for other pembrolizumab dosing information.
Initial dose regimen: The recommend starting daily dose of lenvatinib is 20 mg (two 10-mg capsules) once daily in combination with pembrolizumab 200 mg administered as an intravenous infusion over 30 minutes every 3 weeks.
Monitoring and dose modification and discontinuation For lenvatinib-related toxicities, upon resolution/improvement of an adverse reaction, treatment should be resumed at a reduced dose as suggested in Table 1. When used in combination with pembrolizumab, one or both medicines should be interrupted as appropriate. Lenvatinib should be withheld, dose reduced, or discontinued as appropriate. Withhold or discontinue pembrolizumab in accordance with the instructions in the prescribing information from pembrolizumab. No dose reductions are recommended for pembrolizumab.
Lenvatinib in combination with everolimus:
Initial dose regimen: The recommended starting dose of lenvatinib is 18 mg (one 10 mg capsule and two 4 mg capsules) once daily in combination with 5 mg everolimus once daily. Or as prescribed by the physician.
Refer to the everolimus prescribing information for other everolimus dosing information.
Lenvatinib and everolimus are to be taken at the same time each day with or without food (see Pharmacology: Pharmacokinetics under Actions).
Monitoring and dose modification and discontinuation: For lenvatinib related toxicities, upon resolution/improvement of an adverse reaction to Grade 0-1 or baseline, treatment should be resumed at a reduced dose of lenvatinib as suggested in Table 1.
For toxicities thought to be related to everolimus, treatment should be interrupted, reduced to alternate day dosing, or discontinued. See the everolimus prescribing information for dose adjustment guidelines in the event of toxicity and other relevant safety information or contraindications.
For toxicities thought to be related to both lenvatinib and everolimus, lenvatinib should be reduced (see Table 1) prior to reducing everolimus.
Hepatocellular Carcinoma (HCC):
Initial dose regimen: The recommended starting daily dose of lenvatinib is 8 mg (two 4 mg capsules) once daily for patients with a body weight of < 60 kg and 12 mg (three 4 mg capsules) once daily for patients with a bodyweight of ≥ 60 kg. Or as prescribed by the physician.
Monitoring, dose modification and discontinuation: For lenvatinib-related toxicities, upon resolution/improvement of an adverse reaction, treatment should be resumed at a reduced dose as suggested in Table 1.
Posology: Endometrial Carcinoma (EC): Initial dose regimen: The recommended starting dosage of lenvatinib is 20 mg orally once daily in combination with pembrolizumab 200 mg administered as an intravenous infusion over 30 minutes every 3 weeks until unacceptable toxicity or disease progression. Or as prescribed by the physician.
Refer to the pembrolizumab prescribing information for other pembrolizumab dosing information.
Monitoring, dose modification and discontinuation: For lenvatinib-related toxicities, upon resolution/improvement of an adverse reaction, treatment should be resumed at a reduced dose as suggested in Table 1. When administering lenvatinib in combination with pembrolizumab, interrupt, dose reduce, or discontinue lenvatinib as appropriate. With-hold or discontinue pembrolizumab in accordance with the instructions in the prescribing information for pembrolizumab. No dose reductions are recommended for pembrolizumab. (See Table 1.)
 Click on icon to see table/diagram/image
Special Populations: Patients With Hepatic Impairment:
Click on icon to see table/diagram/image
Special Populations: Patients With Hepatic Impairment: Thyroid Cancer, RCC and EC: No dose adjustments are required on the basis of hepatic function in patients with mild (Child-Pugh A) or moderate (Child-Pugh B) hepatic impairment.
The recommended dosage of lenvatinib for patients with severe hepatic impairment (Child-Pugh C) is: TC: 14 mg taken orally once daily.
RCC: 10 mg taken orally once daily.
EC: 10 mg taken orally once daily.
Further dose adjustments may be necessary on the basis of individual tolerability.
Limited data are available for the combination of lenvatinib with pembrolizumab or everolimus in patients with hepatic impairment. Please refer to the respective prescribing information for pembrolizumab or everolimus for dosing in patients with hepatic impairment.
HCC: No dose adjustments are required on the basis of hepatic function in patients with HCC and mild hepatic impairment (Child-Pugh A). There are limited data in patients with HCC and moderate hepatic impairment (Child-Pugh B). On the basis of that data, the recommended starting dose in patients with moderate hepatic impairment (Child-Pugh B) is 8 mg, regardless of body weight. Patients with moderate hepatic impairment may require additional monitoring for adverse reactions requiring dose adjustments. The available data do not allow for a dosing recommendation for patients with HCC and severe hepatic impairment (Child-Pugh C).
Patients with Renal Impairment: Thyroid Cancer, RCC & EC: No dose adjustments are required on the basis of renal function in patients with mild or moderate renal impairment.
The recommended dosage of lenvatinib for patients with severe renal impairment (creatinine clearance less than 30 mL/min calculated by Cockcroft-Gault equation using actual body weight) is: TC: 14 mg taken orally once daily.
RCC: 10 mg taken orally once daily.
EC: 10 mg taken orally once daily.
Further dose adjustments may be necessary on the basis of individual tolerability.
Limited data are available for the combination of lenvatinib with pembrolizumab or everolimus in patients with renal impairment. Please refer to the respective prescribing information for pembrolizumab or everolimus for dosing in patients with renal impairment.
HCC: No dose adjustments are required on the basis of renal function in HCC patients with mild or moderate renal impairment. The available data do not allow for a dosing recommendation for patients with HCC and severe renal impairment.
Elderly Population: No adjustment of starting dose is required on the basis of age.
Pediatric Patients: The safety and efficacy of lenvatinib in children and adolescents <18 years have not been established. No data are available.
Method of Administration: Take lenvatinib at the same time each day with or without food (see Pharmacology: Pharmacokinetics under Actions).
The lenvatinib capsules should be swallowed whole with water.
Alternatively, add the lenvatinib capsules (without breaking or crushing the capsules) to a tablespoon of water or apple juice in a small glass to produce a suspension. Leave the capsules in the liquid for at least 10 minutes. Stir for at least 3 minutes. Drink the mixture. After drinking, add the same amount of water or apple juice (one tablespoon) to the glass. Swirl the contents of the glass a few times and swallow the additional liquid.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image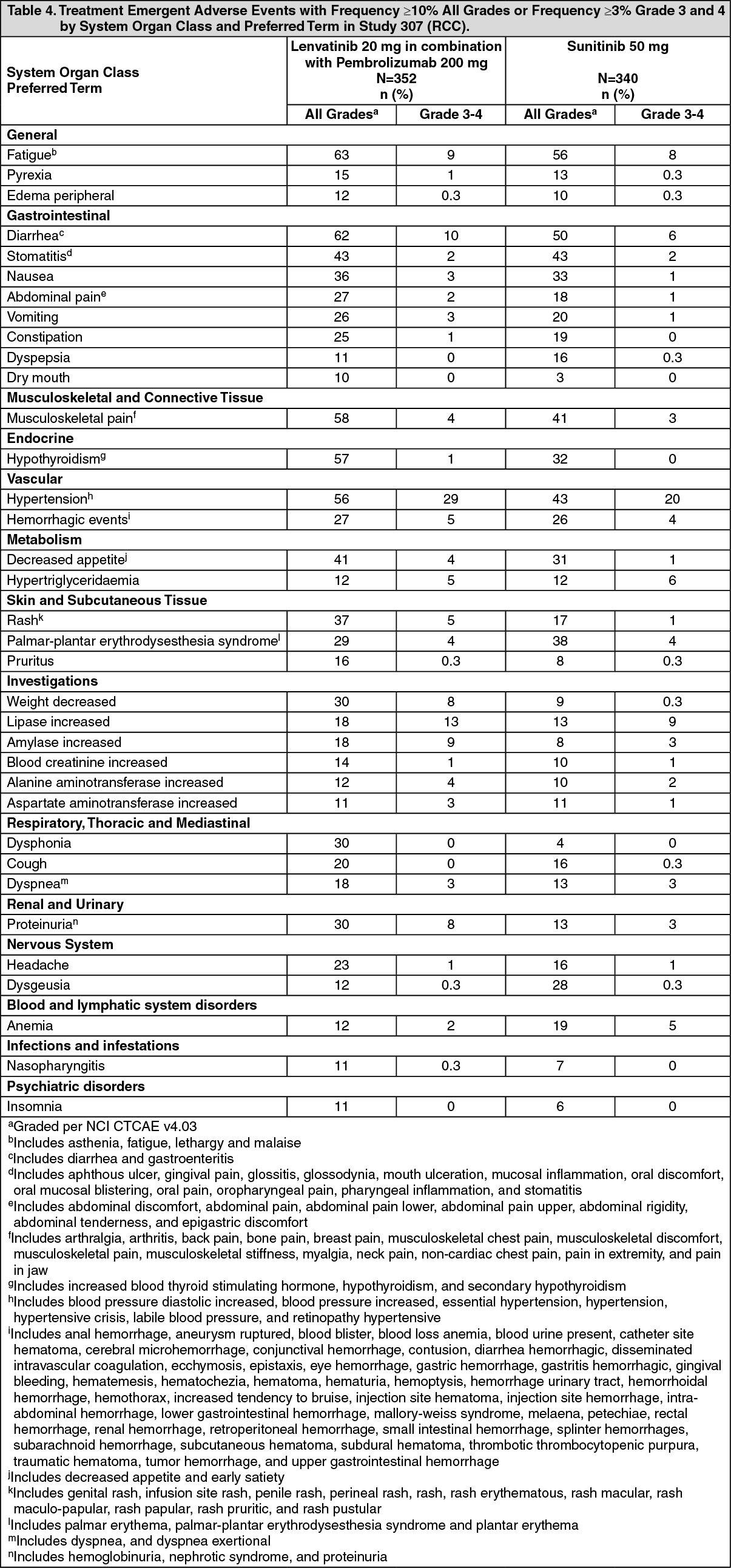 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image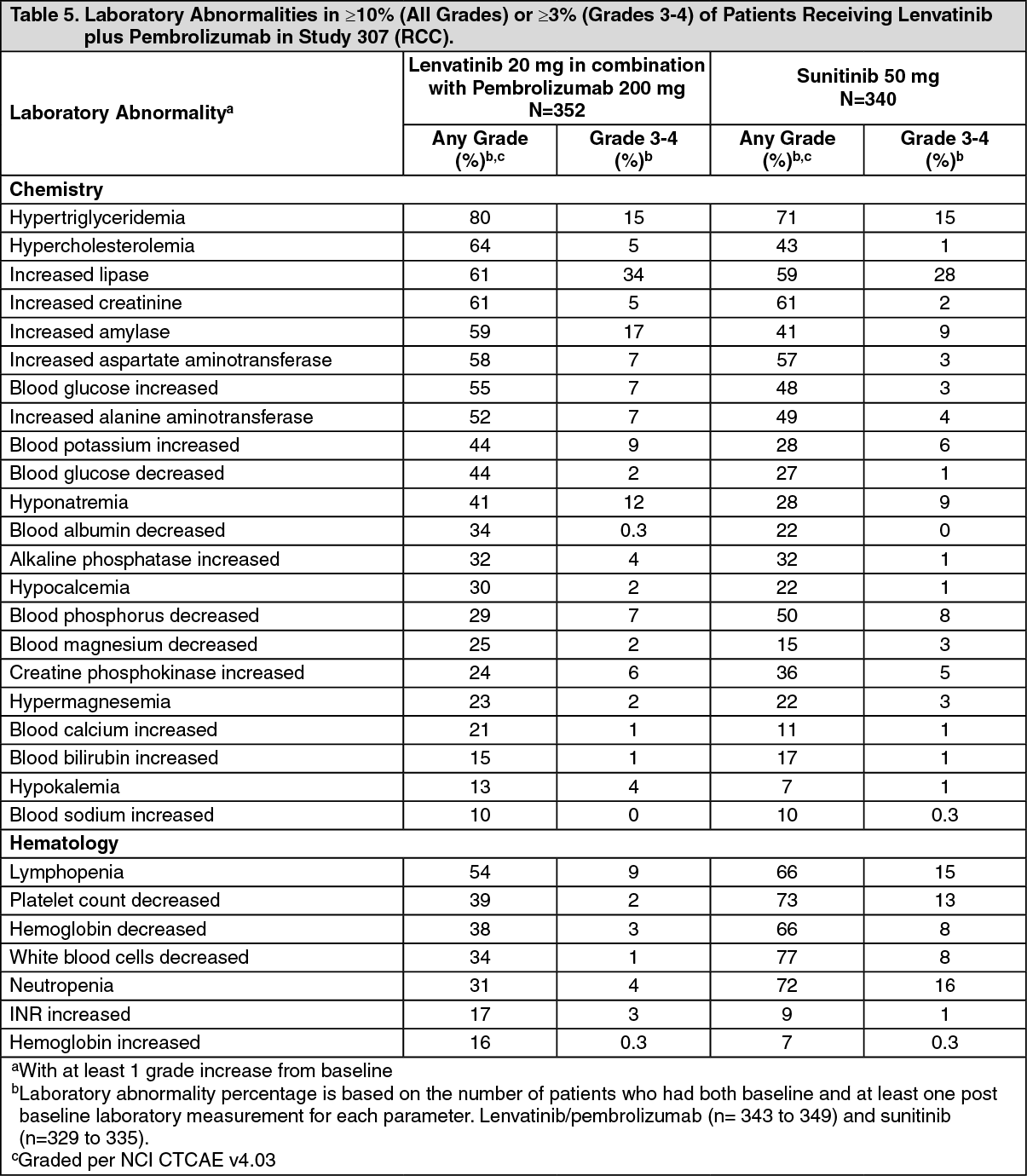 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image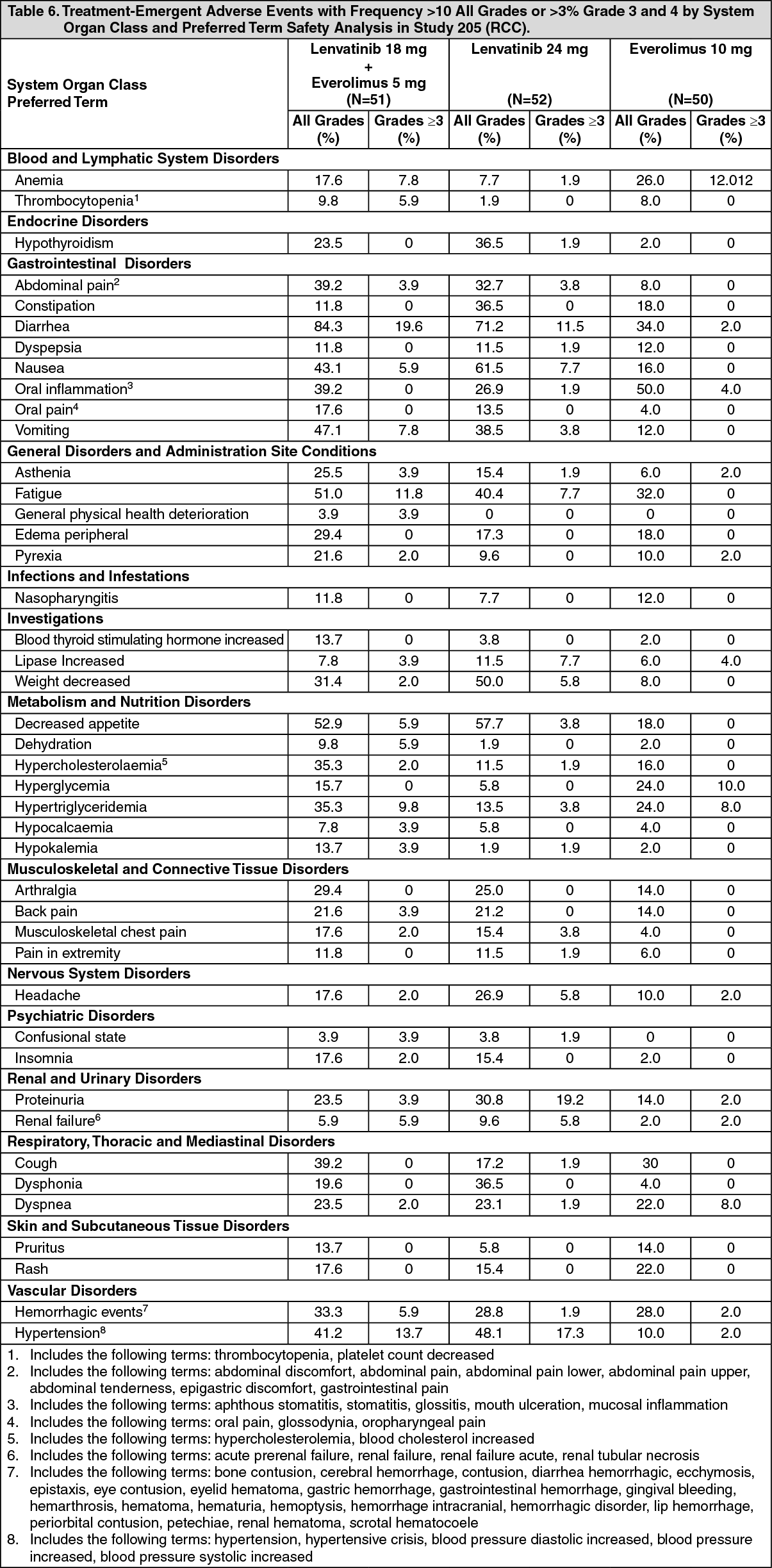 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image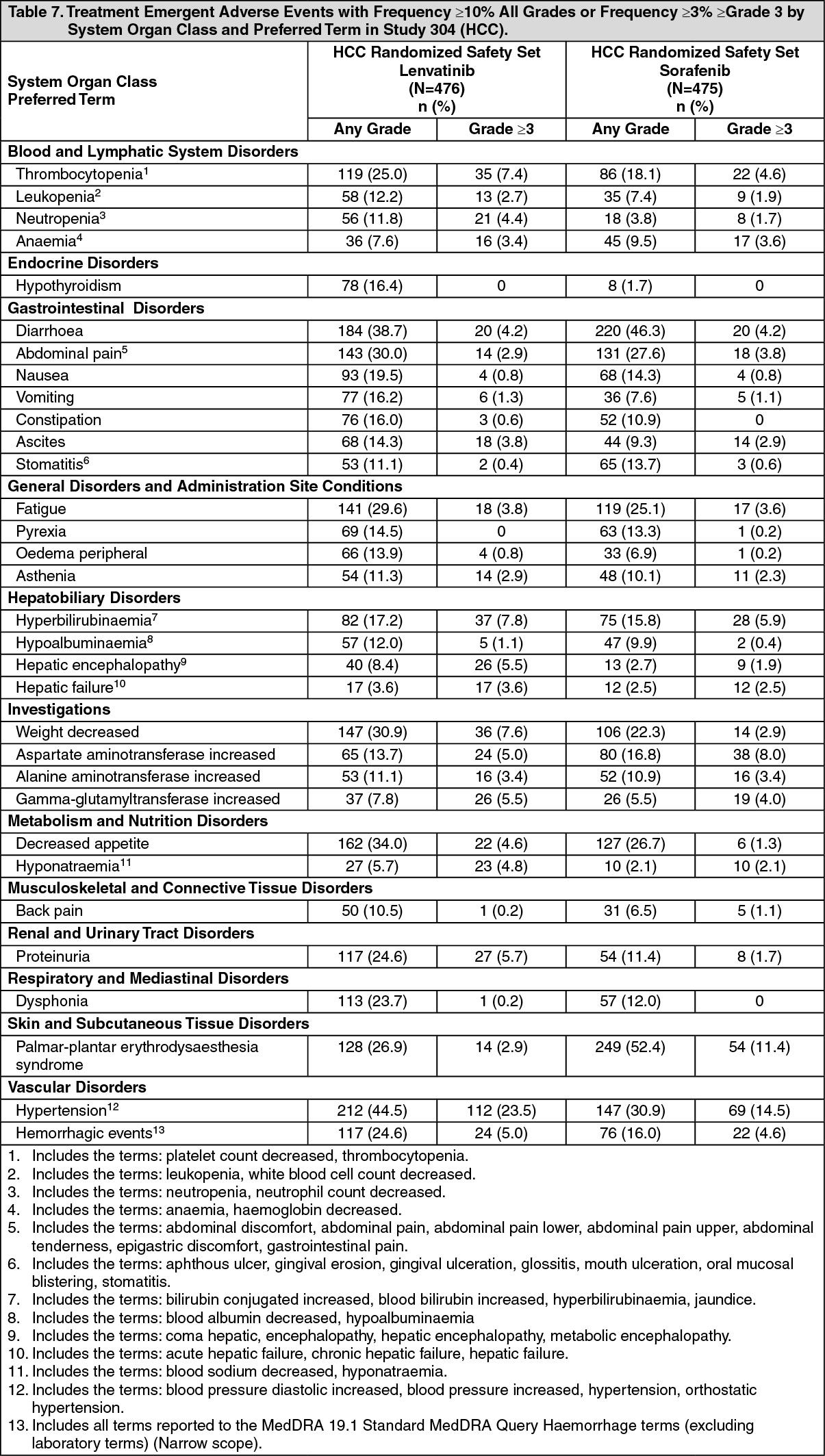 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out