Film-coated tablet: Levetiracetam (Leveget) is given with or without food. The dosage regimens depends on the indication, age group, dosage form & renal function. The tablets should be swallowed whole and not be chewed or crushed.
Monotherapy for adults and adolescents from 16 years of age: The recommended starting dose is 250mg twice daily which should be increased to an initial therapeutic dose of 500mg twice daily after two weeks. The dose can be further increased by 250mg twice daily every two weeks depending upon the clinical response. The maximum dose is 1500mg twice daily.
Add-on therapy: Adults (≥ 18 years) and adolescents (12 to 17 years) weighing 50 kg or more: The initial therapeutic dose is 500 mg twice daily. This dose can be started on the first day of treatment. Depending upon the clinical response and tolerability, the doily dose can be increased up to 1500 mg twice daily. Dose changes can be made in 500 mg twice daily increases or decreases every two to four weeks.
Dosing for Partial Onset Seizures: Adults 16 Years and Older: Initiate treatment with a daily dose of 1g/day, given as twice-daily dosing (500mg twice daily). Additional dosing increments may be given (1g/day additional every 2 weeks) to a maximum recommended daily dose of 3 g. There is no evidence that doses greater than 3 g/day confer additional benefit.
Pediatric Patients (6 Years to < 16 Years): Initiate treatment with a daily dose of 20mg/kg in 2 divided doses (10mg/kg twice daily). Increase the daily dose every 2 weeks by increments of 20mg/kg to the recommended daily dose of 60mg/kg (30mg/kg twice daily). If a patient cannot tolerate a daily dose of 60mg/kg, the daily dose may be reduced. In the clinical trial, the mean daily dose was 44mg/kg. The maximum daily dose was 3 g/day.
For Levetiracetam (Leveget) Tablet, dosing in pediatric patients weighing 20kg to 40kg, initiate treatment with a daily dose of 500mg given as twice daily dosing (250mg twice daily). Increase the daily dose every 2 weeks by increments of 500mg to a maximum recommended daily dose of 1500mg (750mg twice daily).
For Levetiracetam (Leveget) Tablet, dosing in pediatric patients weighing more than 40kg, initiate treatment with a daily dose of 1g/day given as twice daily dosing (500mg twice daily). Increase the daily dose every 2 weeks by increments of 1g/day to a maximum recommended daily dose of 3 g (1500mg twice daily).
Dosing for Myoclonic Seizures in Patients 12 Years of Age and Older with Juvenile Myoclonic Epilepsy: Initiate treatment with a dose of 1g/day, given as twice-daily dosing (500mg twice daily). Increase the dosage by 1g/day every 2 weeks to the recommended daily dose of 3 g. The effectiveness of doses lower than 3 g/day has not been studied.
Dosing for Primary Generalized Tonic-Clonic Seizures: Adults 16 Years and Older: Initiate treatment with a dose of 1g/day, given as twice-daily dosing (500mg twice daily). Increase dosage by 1g/day every 2 weeks to the recommended daily dose of 3 g. The effectiveness of doses lower than 3 g/day has not been adequately studied.
Pediatric Patients (Ages 6 to <16 Years): Initiate treatment with a daily dose of 20mg/kg in 2 divided doses (10mg/kg twice daily). Increase the daily dose every 2 weeks by increments of 20mg/kg to the recommended daily dose of 60mg/kg (30mg/kg twice daily). The effectiveness of doses lower than 60mg/kg/day has not been adequately studied.
Discontinuation: If Levetiracetam (Leveget) has to be discontinued it is recommended to withdraw it gradually (e.g. in adults and adolescents weighing more than 50kg: 500mg decreases twice daily every two to four weeks; in children and adolescents weighting less than 50kg: dose decrease should not exceed 10mg/kg twice daily every two weeks).
Special populations: Elderly (65 years and older): Adjustment of the dose is recommended in elderly patients with compromised renal function.
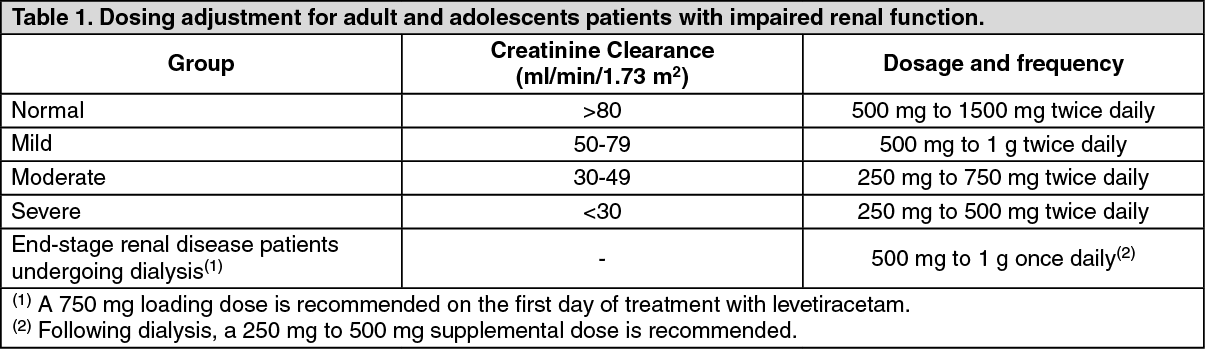
Renal impairment: The daily dose must be individualized according to renal function.
For adult patients, refer to the following table and adjust the dose as indicated. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For children with renal impairment, levetiracetam dose needs to be adjusted based on the renal function as levetiracetam clearance is related to renal function. (See Table 2.)
Click on icon to see table/diagram/image
Hepatic impairment: No dose adjustment is needed in patients with mild to moderate hepatic impairment. In patients with severe hepatic impairment, the creatinine clearance may underestimate the renal insufficiency.
Therefore a 50% reduction of the daily maintenance dose is recommended when the creatinine clearance is < 60mL/min/1.73m
2.
Pediatric population: Monotherapy: The safety & efficacy of levetiracetam in children and adolescents below 16 years as monotherapy treatment have not been established.
Add-on therapy for children (6 to 11 years) and adolescents (12 to 17 years) weighing less than 50kg: The lowest effective dose should be used. The starting dose for a child or adolescent of 25kg should be 250mg twice daily with a maximum dose of 750mg twice daily.
Dose in children 50kg or greater is the same as in adults or as prescribed by physician.
Solution for injection: Dosing for Partial Onset Seizures: Adults 16 Years and Older: Initiate treatment with a daily dose of 1000mg/day, given as twice-daily dosing (500mg twice daily). Additional dosing increments may be given (1000mg/day additional every 2 weeks) to a maximum recommended daily dose of 3000mg. There is no evidence that doses greater than 3000mg/day confer additional benefit.
Pediatric Patients:
1 Month to < 6 Months: Initiate treatment with a daily dose of 14mg/kg in 2 divided doses (7mg/kg twice daily). Increase the daily dose every 2 weeks by increments of 14mg/kg to the recommended daily dose of 42mg/kg (21mg/kg twice daily). In the clinical trial, the mean daily dose was 35mg/kg in this age group.
6 Months to < 4 Years: Initiate treatment with a daily dose of 20mg/kg in 2 divided doses (10mg/kg twice daily). Increase the daily dose in 2 weeks by an increment of 20mg/kg to the recommended daily dose of 50mg/kg (25mg/kg twice daily). If a patient cannot tolerate a daily dose of 50mg/kg, the daily dose may be reduced. In the clinical trial, the mean daily dose was 47mg/kg in this age group.
4 Years to < 16 Years: Initiate treatment with a daily dose of 20mg/kg in 2 divided doses (10mg/kg twice daily). Increase the daily dose every 2 weeks by increments of 20mg/kg to the recommended daily dose of 60mg/kg (30mg/kg twice daily). If a patient cannot tolerate a daily dose of 60mg/kg, the daily dose may be reduced. In the clinical trial, the mean daily dose was 44mg/kg. The maximum daily dose was 3000mg/day.
Dosing for Myoclonic Seizures in Patients with Juvenile Myoclonic Epilepsy: Initiate treatment with a dose of 1000mg/day, given as twice-daily dosing (500mg twice daily). Increase the dosage by 1000mg/day every 2 weeks to the recommended daily dose of 3000mg.
Dosing for Primary Generalized Tonic-Clonic Seizures: Adults 16 Years and Older: Initiate treatment with a dose of 1000mg/day, given as twice-daily dosing (500mg twice daily). Increase dosage by 1000mg/day every 2 weeks to the recommended daily dose of 3000mg.
Pediatric Patients Ages 6 to <16 Years: Initiate treatment with a daily dose of 20mg/kg in 2 divided doses (10mg/kg twice daily). Increase the daily dose every 2 weeks by increments of 20mg/kg (10mg/kg twice daily) to the recommended daily dose of 60mg/kg (30mg/kg twice daily).
Switching from Oral Dosing: When switching from oral levetiracetam, the initial total daily intravenous dosage of levetiracetam should be equivalent to the total daily dosage and frequency of oral levetiracetam.
Switching to Oral Dosing: At the end of the intravenous treatment period, the patient may be switched to levetiracetam oral administration at the equivalent daily dosage and frequency of the intravenous administration.
Preparation and Administration Instructions: Levetiracetam (Leveget) IV Injection is for intravenous use only and should be diluted in 100mL of a compatible diluent prior to administration. If a smaller volume is required (e.g. pediatric patients), the amount of diluent should be calculated to not exceed a maximum levetiracetam concentration of 15mg per mL of diluted solution. Consideration should also be given to the total daily fluid intake of the patient. Levetiracetam (Leveget) IV Injection should be administered as a 15-minute IV infusion.
Levetiracetam (Leveget) IV Injection may be mixed with the following diluents and antiepileptic drugs. The diluted solution should not be stored for more than 4 hours at controlled room temperature [15°C-30°C].
Diluents: Sodium chloride (0.9%) Solution for Injection, Lactated Ringer's Solution for Injection, Dextrose 5% Solution for Injection.
Other Antiepileptic Drugs: Lorazepam, Diazepam, Valproate sodium.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration whenever solution and container permit. Product with particulate matter or discoloration should not be used. Any unused portion of the Levetiracetam (Leveget) IV Injection contents should be discarded.
Adults: See Table 3 for the recommended preparation and administration of Levetiracetam (Leveget) IV Injection for adults to achieve a dose of 500mg, 1000mg, or 1500mg. (See Table 3.)
Click on icon to see table/diagram/image
For example, to prepare a 1000mg dose, dilute 10mL of Levetiracetam (Leveget) IV Injection in 100mL of a compatible diluent and administer intravenously as a 15-minute infusion.
Pediatric Patients: When using Levetiracetam (Leveget) IV Injection for pediatric patients, dosing is weight-based (mg per kg).
The following calculation should be used to determine the appropriate daily dose of Levetiracetam injection for pediatric patients: See Equation 1.
Click on icon to see table/diagram/image
Dosage Adjustments in Adult Patients with Renal Impairment: Levetiracetam dosing must be individualized according to the patient's renal function status. Recommended dosage adjustments for adults with renal impairment are shown in Table 4. Information is unavailable for dosage adjustments in pediatric patients with renal impairment. In order to calculate the dose recommended for adult patients with renal impairment, creatinine clearance adjusted for body surface area must be calculated. To do this an estimate of the patient's creatinine clearance (CLcr) in mL/min must first be calculated using the following formula: See Equation 2.
Click on icon to see table/diagram/image
Then CLcr is adjusted for body surface area (BSA) as follows: See Equation 3 and Table 4.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Method of Administration: Levetiracetam (Leveget) IV Injection is for intravenous use only and the recommended dose must be diluted in at least 100mL of a compatible diluent and administered intravenously as a 15-minute intravenous infusion.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image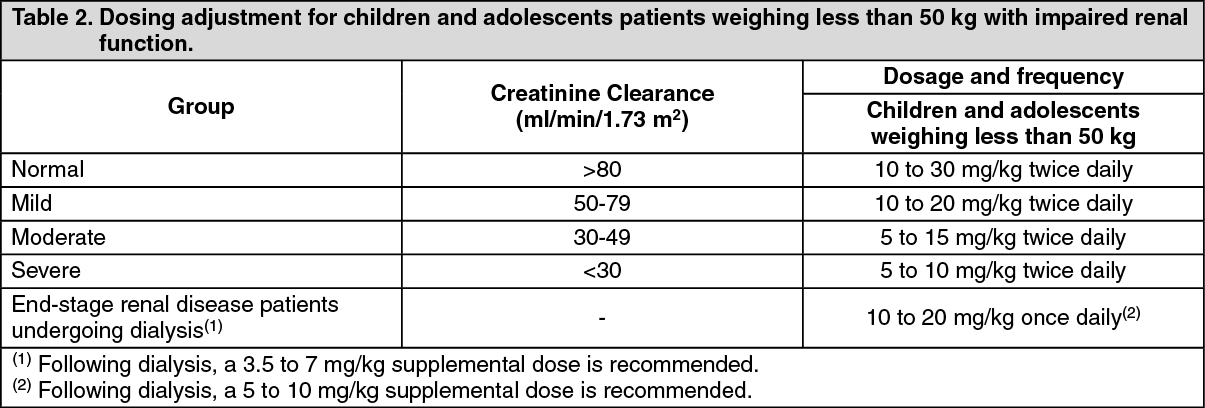 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image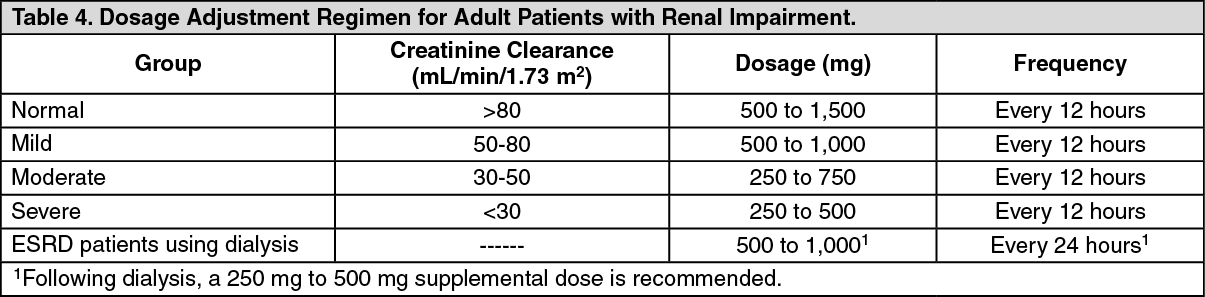 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Sign Out
Sign Out