Gastrointestinal/Metabolism: Occasional: Nausea, diarrhea; Rare: Anorexia, vomiting, abdominal pain, dyspepsia; Very rare: Bloody diarrhea, which in extremely rare cases may be indicative of enterocolitis, including pseudomembranous colitis; Extremely rare: Hypoglycemia, particularly in diabetic patients.
Neurological: Rare: Headache, dizziness/vertigo, drowsiness, and insomnia; Very rare: Paresthesia, tremor, anxiety, agitation, confusions, and convulsion; Extremely rare: Hypoesthesia, visual and auditory disturbances, disturbances of taste and smell and hallucinations.
Musculo-skeletal: Very rare: Arthralgia, myalgia, tendon disorders, including Tendinitis; Extremely rare: Tendon rupture, muscular weakness; Isolated case: Rhabdomyolysis.
Mucocutaneous/Anaphylactic Reactions which may sometimes occur even after the first dose: Occasional: Pain, reddening of the infusion site, phlebitis; Rare: Pruritus, rash; Very rare: Urticaria, bronchospasm/dyspnea; Extremely rare: Angioedema, hypotension, anaphylactic-like shock, photosensitisation; Isolated cases: Severe bullous eruptions such as Stevens Johnson syndrome, toxic epidermal necrolysis (Lyell's syndrome) and erythema exsudativum multiforme.
Liver/Kidney: Occasional: Increase in liver enzymes (ALT, AST); Rare: Increase in bilirubin, increase in serum creatinine; Extremely rare: Liver reactions such as hepatitis, acute kidney failure.
Blood: Rare: Eosinophilia, leukopenia; Very rare: Neutropenia, thrombocytopenia; Extremely rare: Agranulocytosis.
Others: Rare: Asthenia, fungal overgrowth and proliferation of other resistant microorganisms; Extremely rare: Allergic pneumonitis, fever; Some other fluoroquinolones are known to possibly trigger attacks of porphyria in patients with porphyria.
Other possible undesirable effects related to the class of fluoroquinolones: Extremely rare: Psychotic reactions such as acute confusional states and depressive mood changes occur.
Extrapyramidal symptoms and other disorders of muscular coordination.
Hypersensitivity vasculitis.
750 mg Infusion: The most common adverse reactions reported with the use of levofloxacin include nausea, vomiting, diarrhea, constipation, headache, insomnia, and dizziness.
The following undesirable effects of potential medical importance have occurred in patients receiving levofloxacin, regardless of relationship to the drug:
Body as a Whole: Allergic reaction, asthenia, edema, fever/pyrexia, injection/infusion site reaction (pain, reddening, inflammation), multiple organ failure, pain (including pain in back, chest, and extremities), syncope.
Dermatologic/Hypersensitivity Reactions: anaphylactic/anaphylactoid reactions, anaphylactic shock, angioneurotic edema, bullous eruption (including Stevens-Johnson syndrome, toxic epidermal necrolysis, erythema multiforme), leukocytoclastic vasculitis, photosensitivity/phototoxicity, pruritus, genital pruritus, rash serum sickness, urticaria.
Nervous System: Abnormal dreaming/dreams, abnormal electroencephalogram (EEG), abnormal gait, agitation, amnesia, anorexia, anxiety, confusion, convulsions (seizures), depression, dysphonia, encephalopathy, extrapyramidal symptoms and other disorders of muscular coordination; hallucination, , hyperkinesia, hypertonia, exacerbation of myasthenia gravis; nervousness, nightmare, paranoia, paresthesia, sensory or sensorimotor peripheral neuropathy, pseudotumor cerebri, psychosis, sleep disorders, somnolence, isolated reports of suicide attempts or suicidal ideation; tremor, vertigo.
Cardiovascular: cardiac failure/arrest, electrocardiogram QT prolonged, palpitation, phlebitis, tachycardia, vasculitis, vasodilatation, ventricular tachycardia, torsades de pointes, ventricular arrhythmia.
Respiratory: allergic pneumonitis, apnea, dyspnea, laryngeal edema, interstitial pneumonia.
Gastrointestinal (GI): Abdominal pain, hemorrhagic diarrhea which in very rare cases may be indicative of enterocolitis including CDAD and colitis; dyspepsia, esophagitis, gastritis, gastroenteritis, GI hemorrhage, glossitis, pancreatitis, stomatitis.
Metabolic and Nutritional Disorders: hyperglycemia, hypoglycemia, hyperkalemia.
Hepatobiliary: Abnormal hepatic function, increased hepatic enzymes [alkaline phosphatase, alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transpeptidase (GGT)]; jaundice/severe liver injury, hepatic failure (including fatal cases), hepatic necrosis, hepatitis.
Hematologic: Agranulocytosis, anemia (including aplastic and hemolytic anemia), epistaxis, eosinophilia, granulocytopenia, leukopenia, pancytopenia, prolonged International Normalized Ratio (INR); prolonged prothrombin time; thrombocythemia, thrombocytopenia including thrombotic thrombocytopenic purpura; neutropenia.
Genitourinary: Abnormal renal function, acute renal failure, interstitial nephritis, increased blood creatinine; glomerulonephritis, nephrosis, genital moniliasis, vaginitis.
Musculoskeletal and Connective Tissue Disorders: Arthralgia, arthritis, increased muscle enzymes; ligament rupture, myalgia, myositis, muscle injury (including rupture), rhabdomyolysis (including fatal cases), skeletal pain, tendinitis/tendinopathy/tendon disorder, tendon rupture.
Special Senses: Abnormal vision/visual disturbance including diplopia, reduced visual acuity, blurred vision; scotoma; hearing impairment/hypoacusis, tinnitus; anosmia, parosmia; ageusia, dysgeusia, uveitis.
Other Adverse Effects: fungal infection/moniliasis.
In clinical trials using multiple dose therapy, ophthalmologic abnormalities, including cataracts and multiple punctate lenticular opacities, have been observed in patients undergoing treatment with other quinolones. However, the relationship of the drugs to these events has not been definitely established.


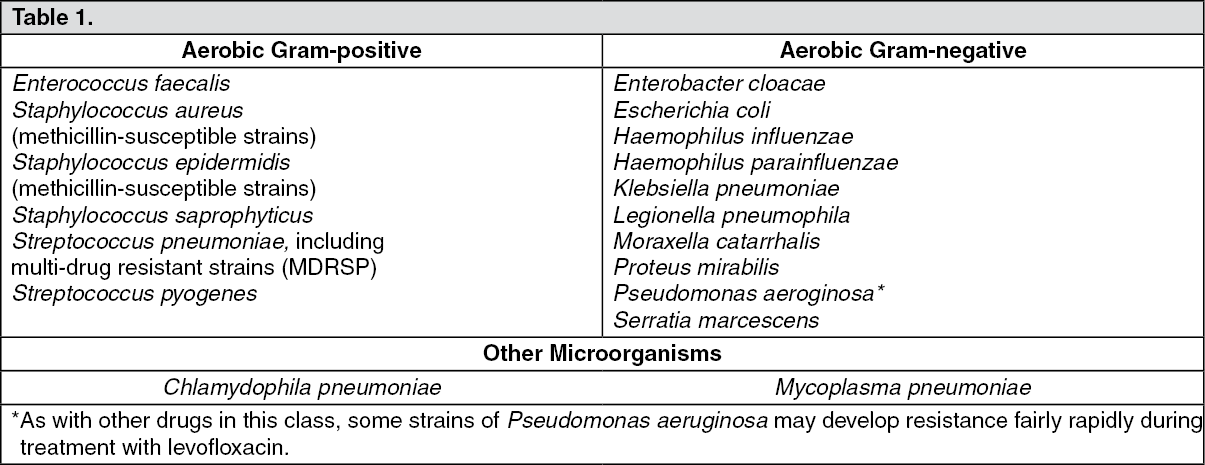 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image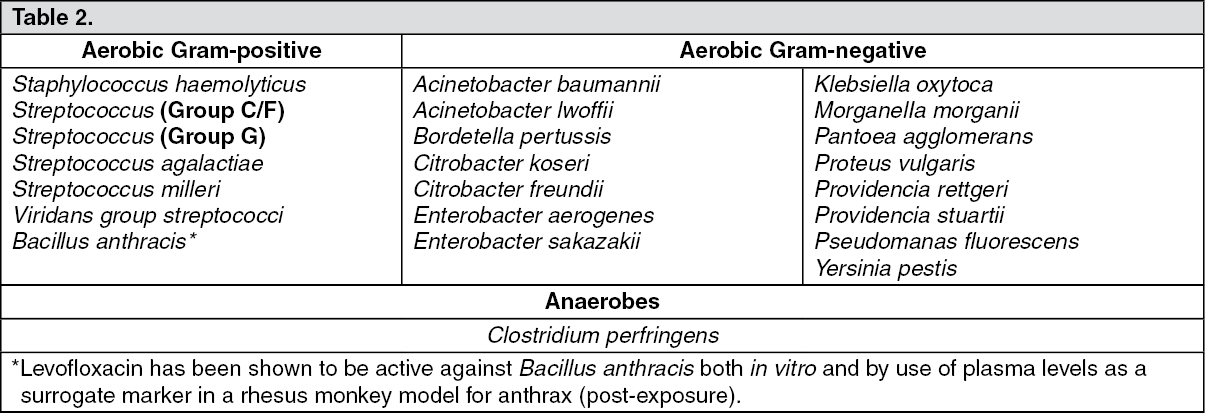 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image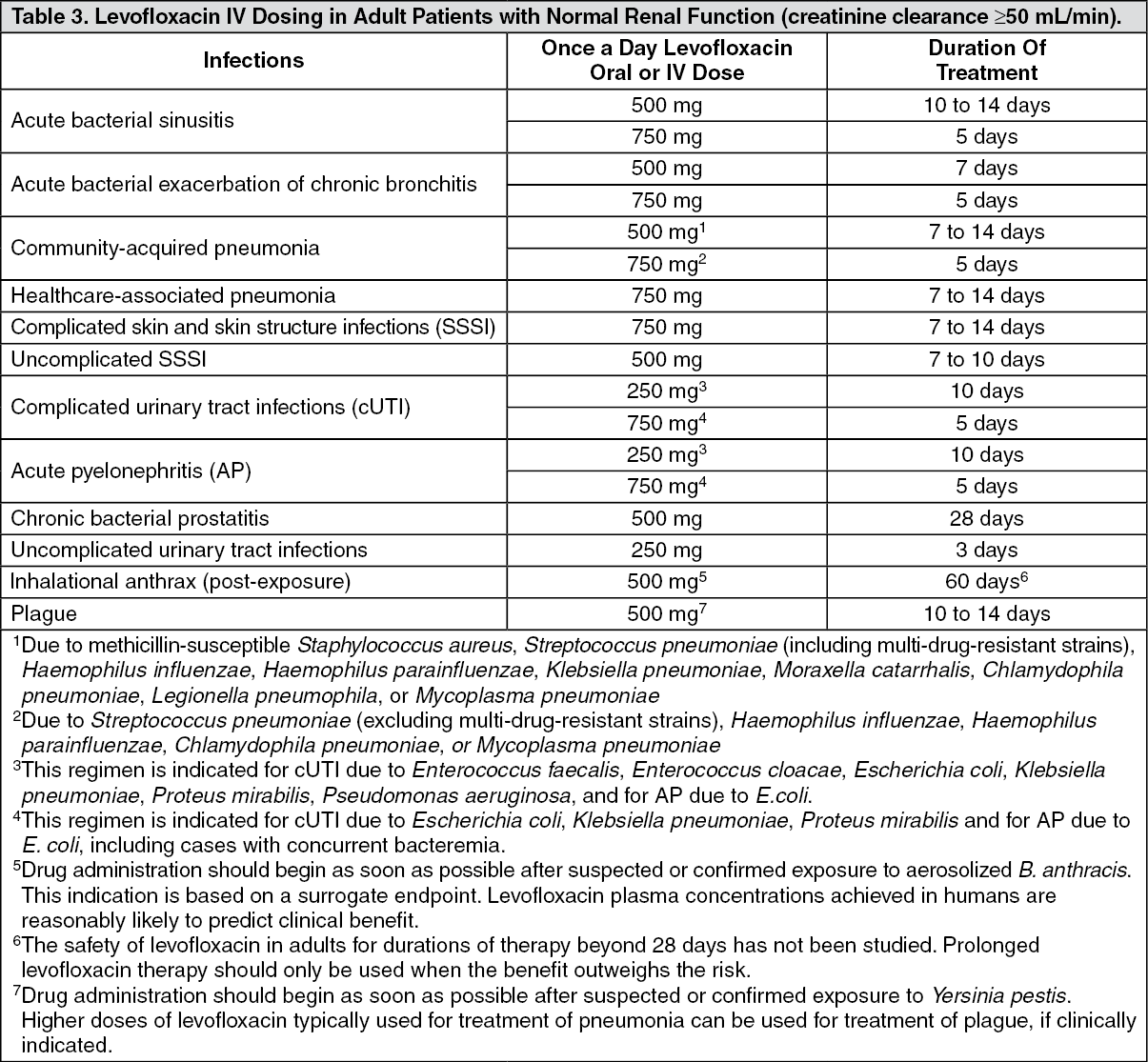 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image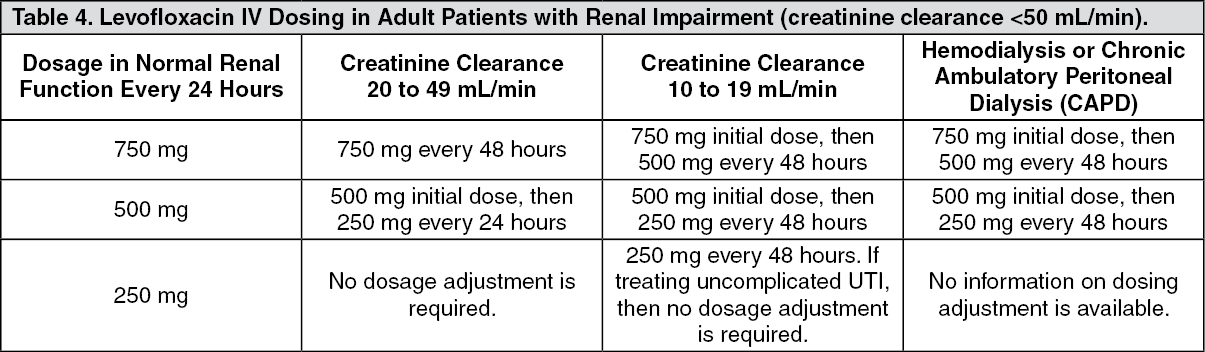 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image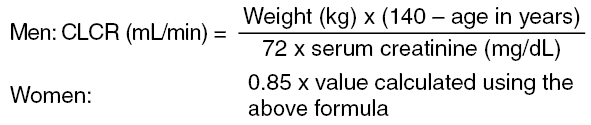 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Sign Out
Sign Out