


 Sign Out
Sign Out
Dosage of allopurinol may also be adjusted according to results of serum uric acid concentration, which should be maintained within the normal range.
In all patients receiving allopurinol, fluid intake should be sufficient to yield a daily urine output of at least two liters and maintenance of a neutral or, preferably, alkaline urine is desirable to: (1) avoid the possibility of formation of xanthine calculi under the influence of allopurinol therapy and (2) help prevent renal precipitation of urates in patients receiving concomitant uricosuric agents.
Management of Gout: Allopurinol is indicated in patients with frequent disabling attacks of gout. Because therapy with allopurinol is not without some serious risks, the drug is not recommended for the management of asymptomatic hyperuricemia.
Optimal treatment of gout requires both nonpharmacological (e.g., weight loss if obese, low purine diet, reduced alcohol intake especially beer) and pharmacological modalities and should be tailored according to: Specific factors (levels of serum urate, previous attacks, radiographic signs); clinical phase (acute/recurrent gout, intercritical gout, and chronic tophaceous gout); general risk factors (age, sex, obesity, alcohol consumption, urate elevating drugs, drug interactions, and comorbidity).
Associated comorbidity and risk factors such as hyperlipidemia, hypertension, hyperglycemia, obesity, and smoking should be addressed as an important part of the management of gout.
If shifting a patient from a uricosuric agent to allopurinol, the dose of the uricosuric agent should be gradually reduced over a period of several weeks and the dose of allopurinol gradually increased to the required dose needed to maintain a normal serum uric acid level.
Recommended Allopurinol Adult Oral Dose for the Management of Intercritical Gout and Chronic Tophaceous Gout: Starting Dose: 100 mg/day two weeks after the pain and swelling of acute gouty arthritis have subsided.
Dose should be titrated by 50 to 100 mg/day every 2 to 4 weeks to achieve serum uric acid <6 mg/dL (0.36 mmol/L).
Maximum dose of allopurinol is 300 mg/day.
Referral to a rheumatologist is recommended if serum uric acid persistently remains >6 mg/dL despite maximum dose of allopurinol.
Serum uric acid and serum creatinine should be periodically monitored.
Management of Leukemia, Lymphoma, and Solid Tumor Malignancies: Recommended Adult Dose: 600 to 800 mg/day for 2 to 3 days.
It is important to ensure adequate hydration to maintain optimum diuresis and to attempt alkalinization of urine to increase solubility of urinary urate/uric acid. The dose of allopurinol should be in the lower range.
It is advisable to correct existing hyperuricemia and/or hyperuricosuria with allopurinol before commencing cytotoxic therapy.
Management of Recurrent Calcium Oxalate Renal Calculi: Initial Dose: 200 to 300 mg/day in divided doses or as a single dose.
Subsequent dosage may be increased or decreased, depending on control of hyperuricosuria assessed by 24-hour urinary urate excretion determination.
Clinical experience shows that patients with recurrent calcium oxalate stones may also benefit from dietary changes such as reduction of animal protein, sodium, refined sugars, oxalate-rich foods, and excessive calcium intake, as well as an increase in oral fluids and dietary fiber.
Recommended Oral Dosage in Renal Impairment: Allopurinol and its metabolites are excreted by the kidneys, therefore impairment of renal function may lead to retention of the drug and/or its metabolites. The plasma half-lives of allopurinol and/or its metabolites may, as a consequence be prolonged.
Dosage should be reduced in patients with impaired renal function to avoid accumulation of allopurinol and its metabolite, oxipurinol.
Allopurinol and its metabolites are removed by renal dialysis. If dialysis is required two to three times a week, an alternative dosage schedule of 300 to 400 mg allopurinol immediately after each dialysis with none in the interim should be considered.
Initial Dose in Renal Impairment: (See Table 1.)
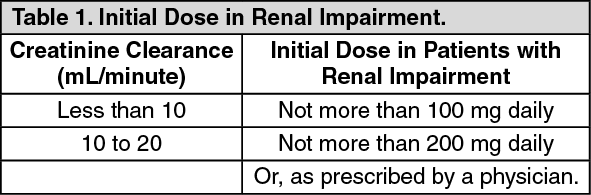 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn patients with severely impaired renal function, it may be advisable to use less than 100 mg/day or to use single doses of 100 mg at longer intervals than one day.
Maintenance Dose in Renal Impairment: (See Table 2.)
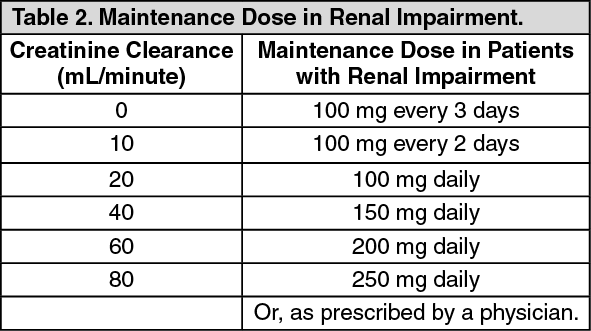 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe correct dose and frequency of dosage for maintaining the serum uric acid just within the normal range is best determined by using the serum uric acid level as an index.