Dosage: Monotherapy for adults and adolescents from 16 years of age: The recommended starting dose is 250 mg twice daily which should be increased to an initial therapeutic dose of 500 mg twice daily after two weeks. The dose can be further increased by 250 mg twice daily every two weeks depending upon the clinical response. The maximum dose is 1500 mg twice daily.
Add-on therapy for adults (≥18 years) and adolescents (12 to 17 years) weighing 50 kg or more: The initial therapeutic dose is 500 mg twice daily. This dose can be started on the first day of treatment.
Depending upon the clinical response and tolerability, the daily dose can be increased up to 1,500 mg twice daily. Dose changes can be made in 500 mg twice daily increases or decreases every two to four weeks.
Special populations: Elderly (65 years and older): Adjustment of the dose is recommended in elderly patients with compromised renal function (see "Renal impairment" as follows).
Renal impairment: The daily dose must be individualised according to renal function.
For adult patients, refer to the following table and adjust the dose as indicated. To use this dosing table, an estimate of the patient's creatinine clearance (CLcr) in ml/min is needed. The CLcr in ml/min may be estimated from serum creatinine (mg/dl) determination, for adults and adolescents weighting 50 kg or more, the following formula: See Equation 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Then CLcr is adjusted for body surface area (BSA) as follows: See Equation 2.
Click on icon to see table/diagram/image
See Table 1.
Click on icon to see table/diagram/image
For children with renal impairment, levetiracetam dose needs to be adjusted based on the renal function as levetiracetam clearance is related to renal function. This recommendation is based on a study in adult renally impaired patients.
The CLcr in ml/min/1.73 m
2 may be estimated from serum creatinine (mg/dl) determination, for young adolescents, children and infants, using the following formula (Schwartz formula): See Equation 3.
Click on icon to see table/diagram/image
ks= 0.45 in Term infants to 1 year old; ks= 0.55 in Children to less than 13 years and adolescent female; ks= 0.7 in adolescent male.
See Table 2.
Click on icon to see table/diagram/image
Hepatic impairment: No dose adjustment is needed in patients with mild to moderate hepatic impairment. In patients with severe hepatic impairment, the creatinine clearance may underestimate the renal insufficiency. Therefore a 50% reduction of the daily maintenance dose is recommended when the creatinine clearance is < 60 ml/min/1.73m
2.
Paediatric population: The tablet formulation is not adapted for use in infants and children under the age of 6 years and children weighing less than 25 kg for administration of doses below 250 mg.
Monotherapy: The safety and efficacy of Levetiracetam in children and adolescents below 16 years as monotherapy treatment have not been established.
No data are available.
Add-on therapy for children (6 to 11 years) and adolescents (12 to 17 years) weighing less than 50 kg: Levetiracetam oral solution is the preferred formulation for use in infants and children under the age of 6 years.
For children 6 years and above, Levetiracetam oral solution should be used for doses under 250 mg, for doses not multiple of 250 mg when dosing recommendation is not achievable by taking multiple tablets and for patients unable to swallow tablets.
The lowest effective dose should be used. The starting dose for a child or adolescent of 25kg should be 250mg twice daily with a maximum dose of 750mg twice daily. Dose in children 50 kg or greater is the same as in adults.
Method of administration: Tablets must be taken orally, swallowed with a sufficient quantity of liquid and may be taken with or without food. The daily dose is administered in two equally divided doses.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image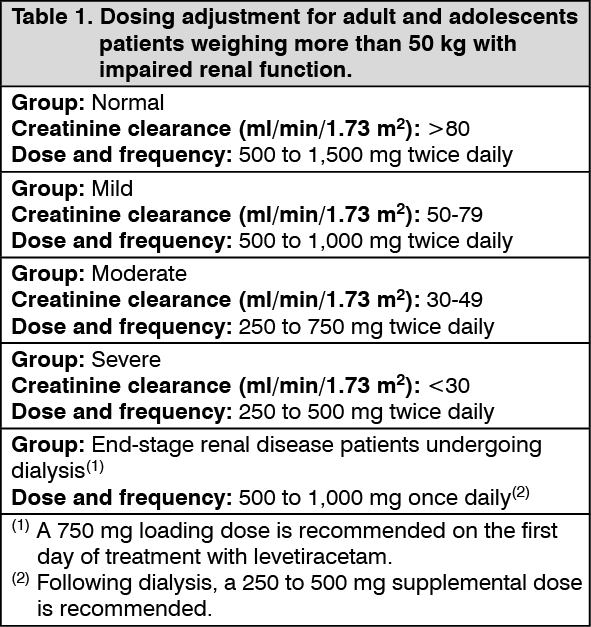 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image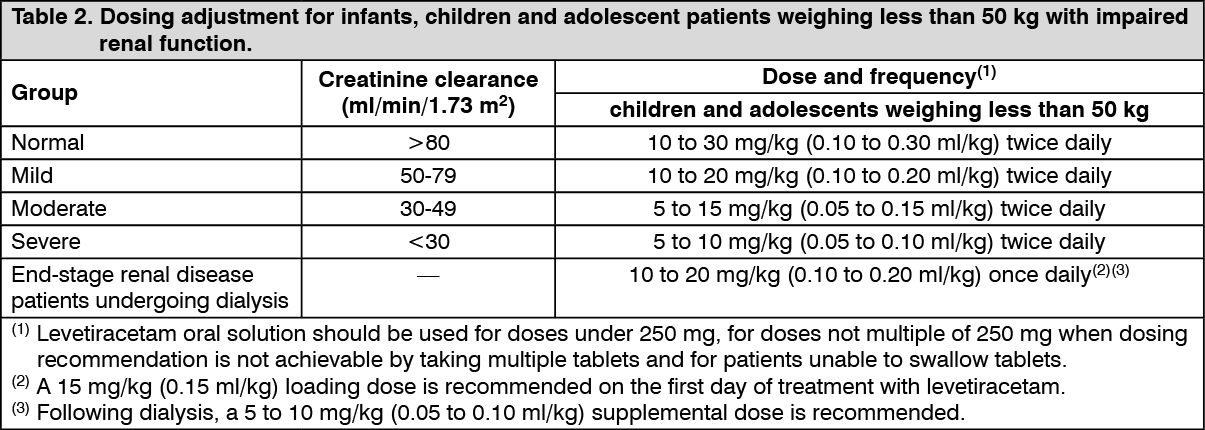 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out