


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Meropenem is a carbapenem antibiotic for parenteral use, that is stable to human dehydropeptidase-1 (DHP-1). Meropenem exerts its bactericidal action by interfering with vital bacterial cell wall synthesis. The ease with which it penetrates bacterial cell walls, its high level of stability to all serine beta-lactamases and its marked affinity for the Penicillin Binding Proteins (PBPs) explain the potent bactericidal action of meropenem against a broad spectrum of aerobic and anaerobic bacteria. The MBC (minimum bactericidal concentration) to MIC (minimum inhibitory concentration) ratios are 2 or less. Meropenem is stable in susceptibility tests and these tests can be performed using normal routine methods. In vitro tests show that meropenem acts synergistically with various antibiotics. It has been demonstrated both in vitro and in vivo that meropenem has a post-antibiotic effect on Gram-positive and Gram-negative bacteria.
A single set of meropenem susceptibility criteria are recommended based on pharmacokinetics and correlation of clinical and microbiological outcomes with zone diameter and minimum inhibitory concentrations (MIC) of the infecting organisms. (See Table 1.)
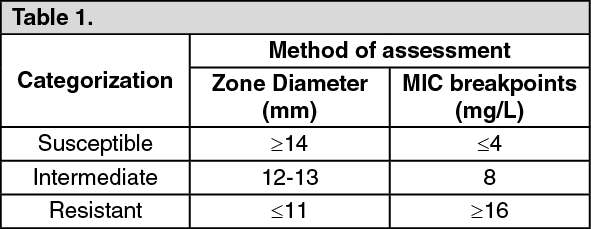 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe in vitro antibacterial spectrum of meropenem includes the majority of clinically significant Gram-positive and Gram-negative, aerobic and anaerobic strains of bacteria, as shown as follows: Gram-positive aerobes: Bacillus spp., Corynebacterium diphtheriae, Enterococcus faecalis, Enterococcus liquifaciens, Enterococcus avium, Erysipelothix rhysiopathiae, Listeria monocytogenes, Lactobacillus spp., Nocardia asteroides, Staphylococcus aureus (penicillinase negative and positive), Staphylococci-coagulase-negative; including Staphylococcus epidermidis, Staphylococcus saprophyticus, Staphylococcus capitis, Staphylococcus cohnii, Staphylococcus xylosus, Staphylococcus warneri, Staphylococcus hominis, Staphylococcus simulans, Staphylococcus intermedius, Staphylococcus sciuri, Staphylococcus lugdunensis, Streptococcus pneumoniae (penicillin susceptible and resistant), Streptococcus agalactiae, Streptococcus pyogenes, Streptococcus equi, Streptococcus bovis, Streptococcus mitis, Streptococcus mitior, Streptococcus milleri, Streptococcus sanguis, Streptococcus viridans, Streptococcus salivarius, Streptococcus morbillorum, Streptococcus cremoris, Streptococcus Group G, Streptococcus Group F, Rhodococcus equi.
Gram-negative aerobes: Achromobacter xylosoxidans, Acinetobacter anitratus, Acinetobacter lwoffii, Acinetobacter baumannii, Acinetobacter junii, Acinetobacter haemolyticus, Aeromonas hydrophila, Aeromonas sorbria, Aeromonas caviae, Alcaligenes faecalis, Bordatella bronchiseptica, Brucella melitensis, Campylobacter coli, Campylobacter jejuni, Citrobacter freundii, Citrobacter diversus, Citrobacter koseri, Citrobacter amalonaticus, Enterobacter aerogenes, Enterobacter agglomerans, Enterobacter cloacae, Enterobacter sakazakii, Escherichia coli, Escherichia hermannii, Gardnerella vaginalis, Haemophilus influenzae (including beta-lactamase positive and ampicillin resistant strains), Haemophilus parainfluenzae, Haemophilus ducreyi, Helicobacter pylori, Neisseria meningitidis, Neisseria gonorrhoeae (including beta-lactamase positive, penicillin resistant and spectinomycin resistant strains), Hafnia alvei, Klebsiella pneumoniae, Klebsiella aerogenes, Klebsiella ozaenae, Klebsiella oxytoca, Moraxella (Branhamella) catarrhalis, Morganella morganii, Proteus mirabilis, Proteus vulgaris, Proteus penneri, Providencia rettgeri, Providencia stuartii, Providencia alcalifaciens, Pasteurella multocida, Plesiomonas shigelloides, Pseudomonas aeruginosa, Pseudomonas putida, Pseudomonas alcaligenes, Pseudomonas cepacia, Pseudomonas fluorescens, Pseudomonas stutzeri, Pseudomonas pickettii, Pseudomonas pseudomallei, Pseudomonas acidovorans, Salmonella spp. including Salmonella enteritidis/typhi, Serratia marcescens, Serratia liquefaciens, Serratia rubidaea, Shigella sonnei, Shigella flexneri, Shigella boydii, Shigella dysenteriae, Vibrio cholerae, Vibrio parahaemolyticus, Vibrio vulnificus, Yersinia enterocolitica.
Anaerobic bacteria: Actinomyces odontolyticus, Actinomyces meyeri, Actinomyces israelii, Bacteroides-Prevotella-Porphyromanas spp., Bacteroides fragilis, Bacteroides vulgatus, Bacteroides variabilis, Bacteroides pneumosintes, Bacteroides coagulans, Bacteroides uniformis, Bacteroides distasonis, Bacteroides ovatus, Bacteroides thetaiotaomicron, Bacteroides eggerthii, Bacteroides capsillosis, Bacteroides gracilis, Bacteroides levii, Bacteroides caccae, Bacteroides ureolyticus, Prevotella buccalis, Prevotella melaninogenica, Prevotella intermedia, Prevotella bivia, Prevotella corporis, Prevotella splanchnicus, Prevotella oralis, Prevotella disiens, Prevotella rumenicola, Prevotella oris, Prevotella buccae, Prevotella denticola, Porphyromonas asaccharolyticus, Porphyromonas gingivalis, Bifidobacterium spp., Bilophila wadsworthia, Clostridium perfringens, Clostridium bifermentans, Clostridium ramosum, Clostridium sporogenes, Clostridium cadaveris, Clostridium difficile, Clostridium sordellii, Clostridium butyricum, Clostridium clostridiiformis, Clostridium innocuum, Clostridium subterminale, Clostridium tertium, Eubacterium lentum, Eubacterium aerofaciens, Fusobacterium mortiferum, Fusobacterium necrophorum, Fusobacterium nucleatum, Fusobacterium varium, Mobiluncus curtisii, Mobiluncus mulieris, Peptostreptococcus anaerodius, Peptostreptococcus micros, Peptostreptococcus saccharolyticus, Peptococcus saccharolyticus, Peptostreptococcus saccharolyticus, Peptostreptococcus magnus, Peptostreptococcus prevotii, Propionibacterium acnes, Propionibacterium avidium, Propionibacterium granulosum, Veillonella parvula, Wolinella recta. Stenotrophomonas (Xanthomonas) maltophilia, Enterococcus faecium and methicillin-resistant staphylococci have been found to be resistant to meropenem.
Pharmacokinetics: A 30-minute intravenous infusion of a single dose of meropenem in healthy volunteers resulted in peak plasma levels of approximately 11 μg/ml for the 250 mg dose, 23 μg/ml for the 500 mg dose and 49 μg/ml for the 1g dose. However, there is no absolute pharmacokinetic proportionality with the administered dose both as regards Cmax and AUC. Furthermore, a reduction in plasma clearance from 287 to 205 ml/min for the range of dosage 250 mg to 2 g has been observed.
A 5-minute intravenous bolus injection in healthy volunteers resulted in peak plasma levels of approximately 52 μg/ml for the 500 mg dose and 112 μg/ml for the 1g dose. Intravenous infusions of 1 g over 2 minutes, 3 minutes and 5 minutes were compared in a three-way crossover trial. These durations of infusion resulted in peak plasma levels of 110, 91 and 94 microgram/ml, respectively. After an IV dose of 500 mg, plasma levels of meropenem decline to values of 1 microgram/ml or less, 6 hours after administration. When multiple doses are administered at 8 hourly intervals to subjects with normal renal function, accumulation of meropenem does not occur.
In patients with normal renal function, meropenem's elimination half-life is approximately 1 hour. Plasma protein binding of meropenem is approximately 2%. Approximately 70% of the administered dose is recovered as unchanged meropenem in the urine over 12 hours, after which little further urinary excretion is detectable. Urinary concentrations of meropenem in excess of 10 μg/ml are maintained for up to 5 hours after the administration of a 500 mg dose. No accumulation of meropenem in plasma or urine was observed with regimens using 500 mg administered every 8 hours or 1 g administered every 6 hours in volunteers with normal renal function.
The only metabolite of meropenem is microbiologically inactive. Meropenem penetrates well into most body fluids and tissues including cerebrospinal fluid of patients with bacterial meningitis, achieving concentrations in excess of those required to inhibit most bacteria. Studies in children have shown that the pharmacokinetics of meropenem in children are similar to those in adults. The elimination half-life for meropenem was approximately 1.5 to 2.3 hours in children under the age of 2 years and the pharmacokinetics are linear over the dose range of 10 to 40 mg/kg.
Pharmacokinetic studies in patients with renal insufficiency have shown the plasma clearance of meropenem correlates with creatinine clearance. Dosage adjustments are necessary in patients with renal impairment. Pharmacokinetic studies in the elderly have shown a reduction in plasma clearance of meropenem which correlated with age-associated reduction in creatinine clearance. Pharmacokinetic studies in patients with liver disease have shown no effects of liver disease on the pharmacokinetics of meropenem.
Toxicology: Preclinical safety data: Animal studies indicate that meropenem is well tolerated by the kidney. In animal studies meropenem has shown nephrotoxic effects, only at high dose levels (500 mg/kg). Effects on the CNS, convulsions in rats and vomiting in dogs, were seen only at high doses >2000 mg/kg). For an IV dose the LD50 in rodents is greater than 2000 mg/kg. In repeat dose studies (up to 6 months) only minor effects were seen including a small decrease in red cell parameters and an increase in liver weight in dogs treated with doses of 500 mg/kg.
There was no evidence of mutagenic potential in the 5 tests conducted and no evidence of reproductive and teratogenic toxicity in studies at the highest possible doses in rats and monkeys; the no effect dose level of a (small) reduction in F1 body weight in rat was 120 mg/kg.
There was an increased incidence of abortions at 500 mg/kg in a preliminary study in monkeys. There was no evidence of increased sensitivity to meropenem in juveniles compared to adult animals.
The intravenous formulation was well tolerated in animal studies. The sole metabolite of meropenem had a similar profile of toxicity in animal studies.