Mometasone furoate monohydrate.
Mometasone furoate (Momenex) Aqueous nasal spray is a white or almost white suspension in HDPE bottle with HDPE pump and cap.
Each actuation contains mometasone furoate monohydrate micronized (eq to mometasone furoate anhydrous) 50 micrograms.
Preservative: Benzalkonium Chloride.
Pharmacotherapeutic group: Decongestants and Other Nasal Preparations for Topical Use-Corticosteroids. ATC code: R01A D09.
Pharmacology: Mechanism of action: Mometasone furoate is a topical glucocorticosteroid with local anti-inflammatory properties at doses that are not systemically active.
It is likely that much of the mechanism for the anti-allergic and anti-inflammatory effects of mometasone furoate lies in its ability to inhibit the release of mediators of allergic reactions. Mometasone furoate significantly inhibits the release of leukotrienes from leucocytes of allergic patients. In cell culture, mometasone furoate demonstrated high potency in inhibition of synthesis and release of IL-1, IL-5, IL-6 and TNF α; it is also a potent inhibitor of leukotriene production. In addition, it is an extremely potent inhibitor of the production of the Th2 cytokines, IL-4 and IL-5, from human CD4 + Tcells.
Pharmacodynamic effects: In studies utilising nasal antigen challenge, Mometasone Furoate Aqueous Nasal Spray has shown anti-inflammatory activity in both the early- and late-phase allergic responses. This has been demonstrated by decreases (vs placebo) in histamine and eosinophil activity and reductions (vs baseline) in eosinophils, neutrophils, and epithelial cell adhesion proteins.
In 28% of the patients with seasonal allergic rhinitis, Mometasone Furoate Aqueous Nasal Spray demonstrated a clinically significant onset of action within 12 hours after the first dose. The median (50%) onset time of relief was 35.9 hours.
Pharmacokinetics: Absorption: Mometasone furoate monohydrate administered as a nasal spray suspension has very low bioavailability (<1%) in plasma using a sensitive assay with a lower quantitation limit (LOQ) of 0.25 pcg/mL.
Distribution: The in vitro protein binding for mometasone furoate was reported to be 98% to 99% in concentration range of 5 to 500 ng/mL.
Metabolism: Studies have shown that any portion of a mometasone furoate dose which is swallowed and absorbed undergoes extensive metabolism to multiple metabolites. There are no major metabolites detectable in plasma. Upon in vitro incubation, one of the minor metabolites formed is 6β-hydroxymometasone furoate. In human liver microsomes, the formation of the metabolite is regulated by cytochrome P-450 3A4 (CYP3A4).
Elimination: Following intravenous administration, the effective plasma elimination half-life of mometasone furoate is 5.8 hours. Any absorbed drug is excreted as metabolites mostly via the bile, and to a limited extent, into the urine.
For use in adults and children 2 years of age and older to treat the symptoms of seasonal allergic or perennial rhinitis. For the treatment of nasal polyps in adults 18 years of age and older.
Treatment with Mometasone Furoate Aqueous Nasal Spray may need to be initiated some days before the expected start of the pollen season in patients who have a history of moderate to severe symptoms of seasonal allergic rhinitis. Prior to administration of the first dose, shake container well and actuate the pump 6-7 times (until a uniform spray is obtained). After initial priming of the Mometasone Furoate Aqueous Nasal Spray pump, each actuation delivers approximately 100 mg of mometasone furoate suspension, containing mometasone furoate monohydrate equivalent to 50 micrograms mometasone furoate. If the pump is not used for 14 days or longer, reprime the pump with 2 actuations until a uniform spray is observed, before next use. Shake container well before each use.
Seasonal Allergic or Perennial Rhinitis: Adults (including older patients) and children 12 years of age and older: The usual recommended dose is two actuations (50 micrograms/actuation) in each nostril once daily (total dose 200 micrograms). Once symptoms are controlled, dose reduction to one actuation in each nostril (total dose 100 micrograms) may be effective for maintenance. If symptoms are inadequately controlled, the dose may be increased to a maximum daily dose of four actuations in each nostril once daily (total dose 400 micrograms). Dose reduction is recommended following control of symptoms.
Children between the ages of 2 and 11 years: The usual recommended dose is one actuation (50 micrograms/actuation).
Nasal Polyposis: The usual recommended starting dose for polyposis is two actuations (50 micrograms/actuation) in each nostril once daily (total daily dose of 200 micrograms). If after 5 to 6 weeks symptoms are inadequately controlled, the dose may be increased to a daily dose of two sprays in each nostril twice daily (total daily dose of 400 micrograms).
Because the systemic bioavailability of Mometasone Furoate Aqueous Nasal Spray is <1%, overdose is unlikely to require any therapy other than observation, followed by initiation of the appropriate prescribed dosage.
Hypersensitivity to the active substance or to any of the excipients.
Immunosuppression: Mometasone Furoate Aqueous Nasal Spray should be used with caution, if at all, in patients with active or quiescent tuberculous infections of the respiratory tract, or in untreated fungal, bacterial, or systemic viral infections.
Patients receiving corticosteroids who are potentially immunosuppressed should be warned of the risk of exposure to certain infections (e.g., chickenpox, measles) and of the importance of obtaining medical advice if such exposure occurs.
Local Nasal Effects: Following 12 months of treatment with Mometasone Furoate Aqueous Nasal Spray in a study of patients with perennial rhinitis, there was no evidence of atrophy of the nasal mucosa; also, mometasone furoate tended to reverse the nasal mucosa closer to a normal histologic phenotype. Nevertheless, patients using Mometasone Furoate Aqueous Nasal Spray over several months or longer should be examined periodically for possible changes in the nasal mucosa. If localised fungal infection of the nose or pharynx develops, discontinuance of Mometasone Furoate Aqueous Nasal Spray therapy or appropriate treatment may be required. Persistence of nasopharyngeal irritation may be an indication for discontinuing Mometasone Furoate Aqueous Nasal Spray.
Mometasone Furoate Aqueous Nasal Spray is not recommended in case of nasal septum perforation.
In clinical studies, epistaxis occurred at a higher incidence compared to placebo. Epistaxis was generally self-limiting and mild in severity.
Mometasone Furoate Aqueous Nasal Spray contains benzalkonium chloride which may cause nasal irritation.
Systemic Effects of Corticosteroids: Systemic effects of nasal corticosteroids may occur, particularly at high doses prescribed for prolonged periods. These effects are much less likely to occur than with oral corticosteroids and may vary in individual patients and between different corticosteroid preparations. Potential systemic effects may include Cushing's syndrome, Cushingoid features, adrenal suppression, growth retardation in children and adolescents, cataract, glaucoma and more rarely, a range of psychological or behavioural effects including psychomotor hyperactivity, sleep disorders, anxiety, depression or aggression (particularly in children).
Following the use of intranasal corticosteroids, instances of increased intraocular pressure have been reported.
Visual disturbance may be reported with systemic and topical (including intranasal, inhaled and intraocular) corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for referral to an ophthalmologist for evaluation of possible causes of visual disturbances which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids.
Patients who are transferred from long-term administration of systemically active corticosteroids to Mometasone Furoate Aqueous Nasal Spray require careful attention. Systemic corticosteroid withdrawal in such patients may result in adrenal insufficiency for a number of months until recovery of HPA axis function. If these patients exhibit signs and symptoms of adrenal insufficiency or symptoms of withdrawal (e.g., joint and/or muscular pain, lassitude, and depression initially) despite relief from nasal symptoms, systemic corticosteroid administration should be resumed and other modes of therapy and appropriate measures instituted. Such transfer may also unmask pre-existing allergic conditions, such as allergic conjunctivitis and eczema, previously suppressed by systemic corticosteroid therapy. Treatment with higher than recommended doses may result in clinically significant adrenal suppression. If there is evidence for higher than recommended doses being used, then additional systemic corticosteroid cover should be considered during periods of stress or elective surgery.
Nasal Polyps: The safety and efficacy of Mometasone Furoate Aqueous Nasal Spray has not been studied for use in the treatment of unilateral polyps, polyps associated with cystic fibrosis, or polyps that completely obstruct the nasal cavities.
Unilateral polyps that are unusual or irregular in appearance, especially if ulcerating or bleeding, should be further evaluated.
Effect on Growth in Paediatric Population: It is recommended that the height of children receiving prolonged treatment with nasal corticosteroids is regularly monitored. If growth is slowed, therapy should be reviewed with the aim of reducing the dose of nasal corticosteroid if possible, to the lowest dose at which effective control of symptoms is maintained. In addition, consideration should be given to referring the patient to a paediatric specialist.
Non-nasal Symptoms: Although Mometasone Furoate Aqueous Nasal Spray will control the nasal symptoms in most patients, the concomitant use of appropriate additional therapy may provide additional relief of other symptoms, particularly ocular symptoms.
There are no or limited amount of data from the use of mometasone furoate in pregnant women. As with other nasal corticosteroid preparations, Mometasone Furoate Aqueous Nasal Spray should not be used in pregnancy unless the potential benefit to the mother justifies any potential risk to the mother, foetus or infant.
Infants born of mothers who received corticosteroids during pregnancy should be observed carefully for hypoadrenalism.
It is not known if mometasone furoate is excreted in human milk. Because other corticosteroids are excreted in human milk, caution should be used when Mometasone Furoate Aqueous Nasal Spray is administered to nursing women.
Summary of the safety profile: Epistaxis was generally self-limiting and mild in severity, and occurred at a higher incidence compared to placebo (5%), but at a comparable or lower incidence when compared to the active control nasal corticosteroids studied (up to 15%) as reported in clinical studies for allergic rhinitis. The incidence of all other adverse events was comparable with that of placebo. In patients treated for nasal polyposis, the overall incidence of adverse events was similar to that observed for patients with allergic rhinitis.
Systemic effects of nasal corticosteroids may occur, particularly when prescribed at high doses for prolonged periods.
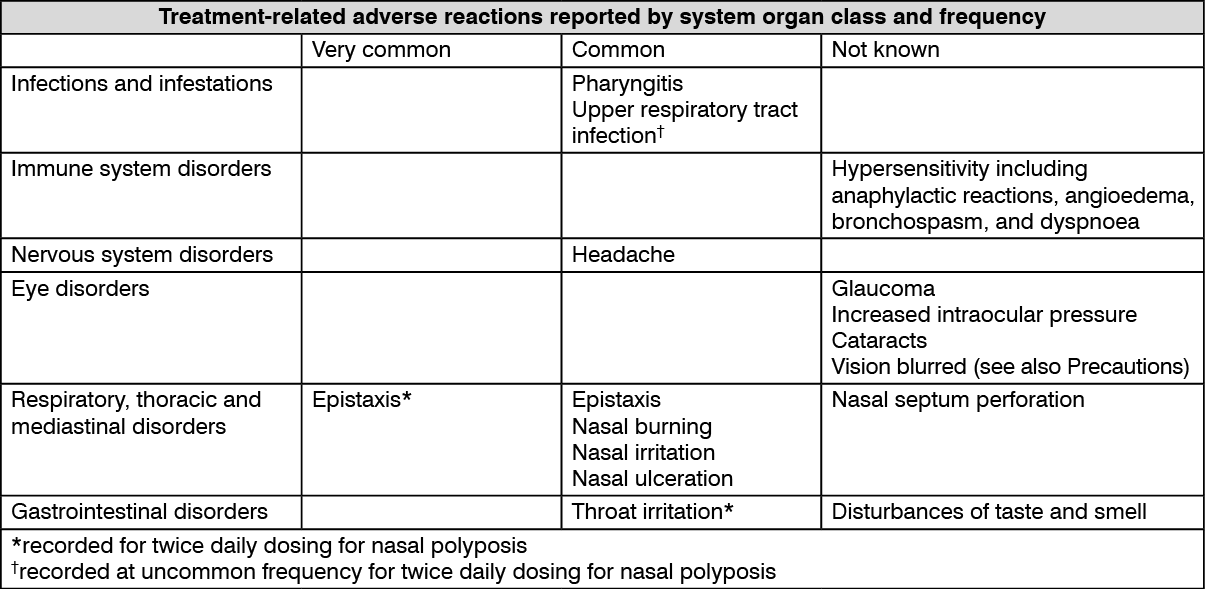
Tabulated list of adverse reactions: Treatment related adverse reactions (≥1%) reported in clinical trials in patients with allergic rhinitis or nasal polyposis and post-marketing regardless of indication are presented in the table. Adverse reactions are listed according to MedDRA primary system organ class. Within each system organ class, adverse reactions are ranked by frequency. Frequencies were defined as follows: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100). The frequency of post-marketing adverse events are considered as "not known (cannot be estimated from the available data)". (See table.)
 Click on icon to see table/diagram/image
Paediatric population:
Click on icon to see table/diagram/image
Paediatric population: In the paediatric population, the incidence of recorded adverse events in clinical studies, e.g., epistaxis (6%), headache (3%), nasal irritation (2%) and sneezing (2%) was comparable to placebo.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product.
No formal drug-drug interaction studies have been conducted with Mometasone Furoate Aqueous Nasal Spray 50 mcg.
Inhibitors of Cytochrome P450 3A4: Studies have shown that mometasone furoate is primarily and extensively metabolized in the liver of all species investigated and undergoes extensive metabolism to multiple metabolites. In vitro studies have confirmed the primary role of cytochrome CYP3A4 in the metabolism of this compound.
Concomitant administration of CYP3A4 inhibitors may inhibit the metabolism of, and increase the systemic exposure to, mometasone furoate and potentially increase the risk for systemic corticosteroid side effects. Caution should be exercised when considering the coadministration of Mometasone Furoate Aqueous Nasal Spray 50 mcg with long-term ketoconazole and other known strong CYP3A4 inhibitors (e.g., ritonavir, cobicistat-containing products, atazanavir, clarithromycin, indinavir, itraconazole, nefazodone, nelfinavir, saquinavir, telithromycin. Consider the benefit of coadministration versus the potential risk of systemic corticosteroid effects, in which case patients should be monitored for systemic corticosteroid side effects.
Store at temperatures not exceeding 30°C.
R01AD09 - mometasone ; Belongs to the class of topical corticosteroids used for prophylaxis and treatment of allergic rhinitis.
Momenex nasal spray 50 mcg/actuation
(w/ pump and cap) 20 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out