Pharmacology: Omeprazole is a racemic mixture of a pair of active optical antipodes which reduces gastric acid secretion through a high target mechanism of action. It is a specific inhibitor of the gastric proton pump in the parietal cell. It is rapidly acting and produces reversible control of gastric acid secretion with once daily dosing.
Omeprazole is a weak base, which is concentrated in the intracellular canaliculi of the parietal cell. Due to the acidic environment in these cells, omeprazole is converted to the active form, where it acts as an inhibitor of the enzyme H+, K+ -ATPase - the proton pump. There is a dose dependency on this final step in the formation of gastric acid, which provides for effective inhibition of the secretion of both basal acid and stimulated acid irrespective of the secretory enhancer. But the inhibition has nothing to do with the stimulus.
Intravenous administration of omeprazole results in dose related inhibition of acid secretion. 40 mg i.v. dose of omeprazole is recommended for the first time in order to produce similar effect immediately on intragastric acidity as repeated oral dosing with 20 mg. The IV injection produces an immediate decrease in intragastric acidity and a mean decrease over 24 hours of approximately 90%. The inhibition of acid secretion is related to the area under the plasma concentration-time curve (AUC) and not to the actual plasma concentration at a given time.
Acid digestive diseases are concerned with Helicobacter pylori, including 95% of duodenal and 70% of gastrohelcoma. Helicobacter pylori are the main factor leading to gastritis. The chief ingredients in causing peptic ulcer are Helicobacter pylori along with gastric acid. Omeprazole can eradicate Helicobacter pylori combined with proper antibiotics. This treat is related to quick relief of symptoms, high reparation rate of gastric mucosa and the long-term mitigation of peptic ulcer disease, which thus reduces the complications of gastrointestinal bleeding and cuts down the long-term need of antacid at the same time.
Decreased gastric acidity due to any means including proton pump inhibitors, increases gastric counts of bacteria normally present in the gastrointestinal tract. Treatment with acid-reducing drugs may lead to a slightly increased risk of gastrointestinal infections, such as Salmonella and Campylobacter.
Pharmacokinetics: Distribution: The apparent volume of distribution in healthy subjects is approximately 0.3 L/kg and a similar value is also seen in patients with renal insufficiency. In elderly patients, and in patients with hepatic insufficiency, the volume of distribution is slightly decreased. The plasma protein binding of omeprazole is about 95%.
Metabolism and Excretion: The average half-life of the terminal phase of the plasma concentration-time curve following IV administration of omeprazole is approximately 40 minutes. The total plasma clearance is 0.3 to 0.6 L/min. There is no change in half-life during treatment.
Omeprazole is completely metabolised by the cytochrome P450 system (CYP), mainly in the liver. The major part of its metabolism is dependent on the polymorphically expressed, specific isoform CYP2C19 (S-mephenytoin hydroxylase), responsible for the formation of hydroxyomeprazole, the major metabolite in plasma. In accordance with this, as a consequence of competitive inhibition, there is a potential for metabolic drug-drug interactions between omeprazole and other substrates for CYP2C19.
No metabolite has been found to have any effect on gastric acid secretion. Almost 80% of an intravenously given dose is excreted as metabolites in the urine, and the remainder is found in the faeces, primarily originating from bile secretion.
There is no significant change in the systemic bioavailability of omeprazole in patients with impaired renal function. Although the area under the plasma concentration-time curve is increased in patients with reduced liver function, no apparent accumulation of omeprazole has been found.
Toxicology: Gastric ECL-cell hyperplasia and carcinoids have been observed in long-term studies in rats treated with omeprazole, H2-recepter blocking agent or proton pump inhibitor, or subjected to partial fundectomy. These changes are the result of sustained hypergastrinaemia secondary to acid inhibition, and not from a direct effect of any individual drug.
Omeprazole inhibits secretion of gastric acid by irreversibly blocking the enzyme system of hydrogen/potassium adenosine triphosphatase (H+/K+ ATPase), the proton pump of the gastric parietal cell. It is used in conditions where inhibition of the gastric acid secretion may be beneficial including aspiration syndromes, dyspepsia, gastro-esophageal reflux disease, peptic ulcer disease, and the Zollinger-Ellison syndrome.
40 mg omeprazole sodium powder is dissolved in 100 mL of 0.9% NaCl solution or 100 mL of 5% Glucose solution. After reconstitution the injection should be given slowly over a period of 20~30 minutes or even longer. No other solvents or drugs for infusion should be used.
In some patients with duodenal ulcer, gastric ulcer or reflux oesophagitis refractory to oral treatment, IV drop of 40 mg, o.d, is recommended.
Intravenous doses of up to 270 mg on a single day and up to 650 mg over a three-day period have been given in clinical trials without any dose related adverse effects.
Known hypersensitivity to omeprazole and its derivatives.
This medicine should not go with other antacids or drugs of restraining acid because of its powerful and long-time acid inhibition. In order to prevent excessive acid inhibition, high-dose long-term application is not recommended in general peptic ulcer disease, Zollinger-Ellison Syndrome patients are ruled out.
The absorption of quite a lot of medicine may be influenced due to the increase in intragastric pH.
No dosage adjustment is recommended for patients with reduced renal function. Dosage extenuation based on pathogenetic condition is necessary for patients with impaired hepatic function.
If a gastric ulcer is suspected the possibility of malignancy should be excluded as treatment may mask the symptoms and delay diagnosis.
Use in Children: Safety and effectiveness in pediatric patients have not been established.
Use in Elderly: Dosage adjustment for elderly patients is not necessary.
Although no adverse effects or deleteriousness or teratogenic action on foetus during gestation period and lactation in animal experiments, it is recommended that pregnant and lactating women do not have it if possible. Safety in pregnancy and lactation has not been established.
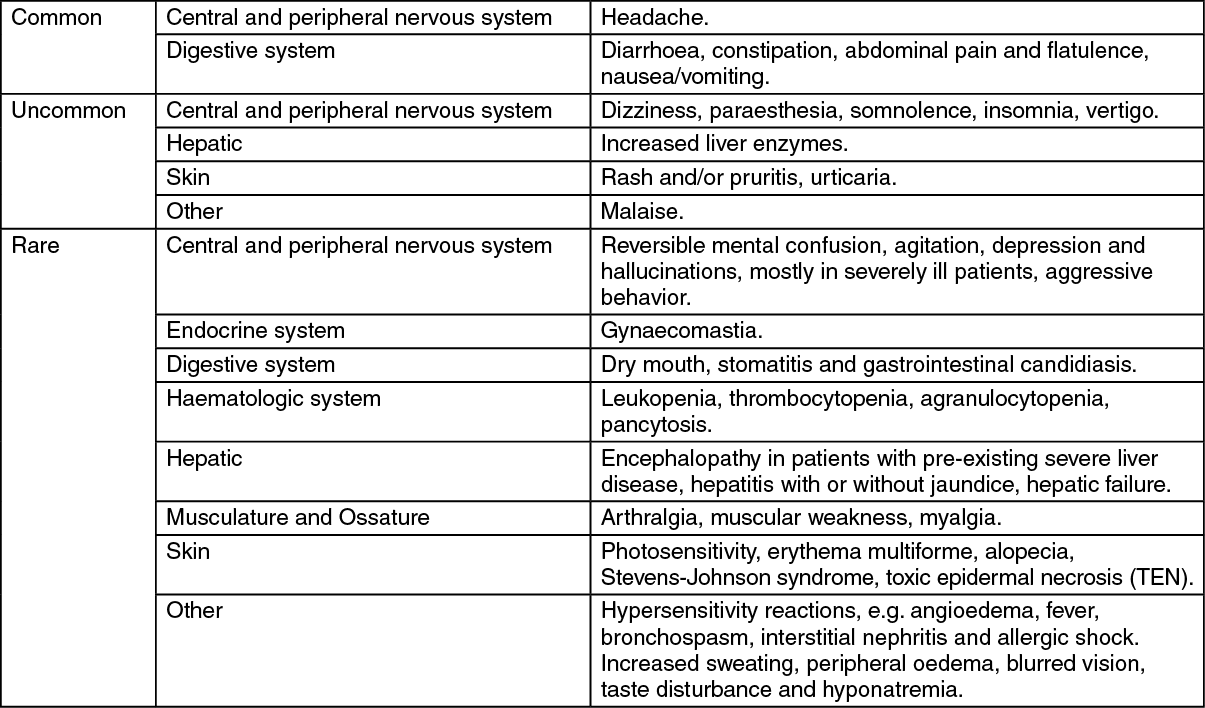
Omeprazole is well tolerated and adverse reactions are generally mild and reversible. The following have been reported as adverse events in clinical trials or reported from routine use but in many cases a relationship to treatment with omeprazole has not been established.
The following definitions of frequencies are used: "common": the incidence ≥ 1:100; "uncommon": 1:1000 ≤ the incidence <1:100; "rare": the incidence <1:1000. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Isolated cases of irreversible visual impairment have been reported in critically ill patients who have received intravenous injection of omeprazole at high dose.
There is a possibility of an alteration in the absorption of some medicine due to the increase in intragastric pH. Therefore, concomitant administration with omeprazole or other acid inhibitors or other antacids may reduce the gastric absorption of ketoconazole or itraconazole.
Omeprazole can prolong the elimination of medicines which are metabolised by oxidation in the liver, e.g. diazepam, warfarin (R-warfarin), and phenytoin because of the metabolism of omeprazole via the cytochrome F4502C19 (CYP2C19) in the liver.
Patients receiving warfarin or phenytoin concomitant with omeprazole, should be monitored closely as a reduction in dosages of warfarin or phenytoin may be required. It was however shown in patients on concurrent omeprazole treatment at a daily dosage of 20 mg and continuous phenytoin treatment, that the simultaneous use of these two medications did not influence the blood concentration of phenytoin. Concomitant treatment with omeprazole 20 mg daily also did not alter coagulation time in patients on long-term treatment.
The plasma concentrations of both omeprazole and clarithromycin may be increased during concomitant treatment with these medicines. But no interactions with arilin and amoxycillin have been recorded. The concomitant use of omeprazole and these antibiotics can eradicate the Helicobacter pylori.
Store at temperatures not exceeding 25°C. Protect from light.
A02BC01 - omeprazole ; Belongs to the class of proton pump inhibitors. Used in the treatment of peptic ulcer and gastro-oesophageal reflux disease (GERD).
Omevex infusion (lyo) 40 mg
10 × 1's (P475/vial)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 40 mg7651f574-2675-46c2-86a1-a20700db0d83.GIF)

 Sign Out
Sign Out