Active substance: 1 vial contains 45.18 mg pantoprazole sodium sesquihydrate, equivalent to 40.00 mg of pantoprazole.
Excipients/Inactive Ingredients: Sodium hydroxide (for pH adjustment), Water for injection.
Pharmacotherapeutic group: Proton pump inhibitors. ATC code: A02BC02.
Pharmacology: Pharmacodynamics: Mechanism of action: Pantoprazole is a substituted benzimidazole which inhibits the secretion of hydrochloric acid in the stomach by specific blockade of the proton pumps of the parietal cells.
Pantoprazole is converted to its active form in the acidic environment in the parietal cells where it inhibits the H+, K+-ATPase enzyme, i.e. the final stage in the production of hydrochloric acid in the stomach. The inhibition is dose-dependent and affects both basal and stimulated acid secretion. In most patients, freedom from symptoms is achieved within 2 weeks. As with other proton pump inhibitors and H2 receptor inhibitors, treatment with pantoprazole reduces acidity in the stomach and thereby increases gastrin in proportion to the reduction in acidity. The increase in gastrin is reversible. Since pantoprazole binds to the enzyme distal to the cell receptor level, it can inhibit hydrochloric acid secretion independently of stimulation by other substances (acetylcholine, histamine, gastrin). The effect is the same whether the product is given orally or intravenously.
Pharmacodynamic effects: The fasting gastrin values increase under pantoprazole. On short-term use, in most cases they do not exceed the upper limit of normal. During long-term treatment, gastrin levels double in most cases. An excessive increase, however, occurs only in isolated cases. As a result, a mild to moderate increase in the number of specific endocrine (ECL) cells in the stomach is observed in a minority of cases during long-term treatment (simple to adenomatoid hyperplasia). However, according to the studies conducted so far, the formation of carcinoid precursors (atypical hyperplasia) or gastric carcinoids as were found in animal experiments (see Preclinical safety data as follows) have not been observed in humans.
An influence of a long term treatment with pantoprazole exceeding one year cannot be completely ruled out on endocrine parameters of the thyroid according to results in animal studies.
During treatment with antisecretory medicinal products, serum gastrin increases in response to the decreased acid secretion. Also, CgA increases due to decreased gastric acidity. The increased CgA level may interfere with investigations for neuroendocrine tumours.
Available published evidence suggests that proton pump inhibitors should be discontinued between 5 days and 2 weeks prior to CgA measurements. This is to allow CgA levels that might be spuriously elevated following PPI treatment to return to reference range.
Pharmacokinetics: General pharmacokinetics: Pharmacokinetics does not vary after single or repeated administration. Concomitant food intake does not affect AUC, maximum concentration and bioavailability. In the dose range of 10 to 80 mg, the plasma kinetics of pantoprazole are linear after both oral and intravenous administration.
Absorption: Absorption information is not valid since it is directly administered to the bloodstream.
Distribution: Pantoprazole's serum protein binding is about 98%, mainly albumin. Volume of distribution is about 0.15 L/kg. Mainly distributed in the extracellular fluid. Total serum clearance is approximately 0.1 L/h/kg. The terminal half-life was approximately 1 hour.
Biotransformation: The substance is almost exclusively metabolized in the liver by the cytochrome P450 (CYP) enzyme system. Its metabolism is independent of the route of administration (oral or intravenous). The main metabolic pathway is demethylation by CYP2C19 with subsequent sulphate conjugation, other metabolic pathway includes oxidation by CYP3A4. There is no evidence of significant pharmacological activity of pantoprazole metabolites.
Elimination: Terminal half-life is about 1 hour and clearance is about 0.1 l/h/kg. There were a few cases of subjects with delayed elimination. Because of the specific binding of pantoprazole to the proton pumps of the parietal cell the elimination half-life does not correlate with the much longer duration of action (inhibition of acid secretion).
Renal elimination represents the major route of excretion (about 80%) for the metabolites of pantoprazole; the rest is excreted with the faeces. The main metabolite in both the serum and urine is desmethylpantoprazole which is conjugated with sulphate. The half-life of the main metabolite (about 1.5 hours) is not much longer than that of pantoprazole.
Linearity/non-linearity: The plasma kinetics of pantoprazole is after oral and intravenous administration at a dose range of 10-80 mg.
Special populations: Polymorphic metabolisers: Approximately 3% of the European population lack a functional CYP2C19 enzyme and are called poor metabolisers. In these individuals the metabolism of pantoprazole is probably mainly catalysed by CYP3A4. After a single-dose administration of 40 mg pantoprazole, the mean area under the plasma concentration-time curve was approximately 6 times higher in poor metabolisers than in subjects having a functional CYP2C19 enzyme (extensive metabolisers). Mean peak plasma concentrations were increased by about 60%. These findings have no implications for the posology of pantoprazole.
Renal impairment: No dose reduction is recommended when pantoprazole is administered to patients with impaired renal function (incl. dialysis patients). As with healthy subjects, pantoprazole's half-life is short. Only very small amounts of pantoprazole are dialyzed. Although the main metabolite has a moderately delayed half-life (2-3 h), excretion is still rapid and thus accumulation does not occur.
Hepatic impairment: Although for patients with liver cirrhosis (classes A and B according to Child) the half-life values increased to between 7 and 9 h and the AUC values increased by a factor of 5-7, the maximum serum concentration only increased slightly by a factor of 1.5 compared with healthy subjects.
Paediatric population: Following administration of single intravenous doses of 0.8 or 1.6 mg/kg pantoprazole to children aged 2-16 years there was no significant association between pantoprazole clearance and age or weight. AUC and volume of distribution were in accordance with data from adults.
Older people: A slight increase in AUC and Cmax in elderly volunteers compared with younger counterparts is also not clinically relevant.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard to humans based on conventional studies of safety pharmacology, repeated dose toxicity and genotoxicity.
In the two-year carcinogenicity studies in rats neuroendocrine neoplasms were found. In addition, squamous cell papillomas were found in the fore stomach of rats. The mechanism leading to the formation of gastric carcinoids by substituted benzimidazoles has been carefully investigated and allows the conclusion that it is a secondary reaction to the massively elevated serum gastrin levels occurring in the rat during chronic high-dose treatment. In the two-year rodent studies an increased number of liver tumors was observed in rats and in female mice and was interpreted as being due to pantoprazole's high metabolic rate in the liver.
A slight increase of neoplastic changes of the thyroid was observed in the group of rats receiving the highest dose (200 mg/kg). The occurrence of these neoplasms is associated with the pantoprazole-induced changes in the breakdown of thyroxine in the rat liver. As the therapeutic dose in man is low, no harmful effects on the thyroid glands are expected.
In animal reproduction studies, signs of slight fetotoxicity were observed at doses above 5 mg/kg.
Investigations revealed no evidence of impaired fertility or teratogenic effects.
Penetration of the placenta was investigated in the rat and was found to increase with advanced gestation. As a result, concentration of pantoprazole in the foetus is increased shortly before birth.
Gastroesophageal reflux disease.
Short-term maintenance of haemostasis and prevention of recurrence in patients with acute hemorrhagic gastric or duodenal ulcer.
Gastric and duodenal ulcer.
Zollinger-Ellison-Syndrome and other pathological hyper secretory conditions.
This medicine should be administered by a healthcare professional and under appropriate medical supervision.
Intravenous administration is recommended only if oral administration is not appropriate. Data are available on intravenous use for up to 7 days. Therefore, as soon as oral therapy is possible, treatment with PANTONIL i.v. should be discontinued and 40 mg pantoprazole p.o. should be administered instead.
Posology: Gastric and duodenal ulcer, mild and severe gastroesophageal reflux: The recommended intravenous dose is one vial of PANTONIL (40 mg pantoprazole) per day.
Short-term maintenance of haemostasis and prevention of recurrence in patients with acute hemorrhagic gastric or duodenal ulcer: In patients with acute haemorrhagic gastric or duodenal ulcer, 80 mg should be administered as bolus infusion for 2-15 minutes followed by continuous intravenous infusion at 8 mg/hr for 3 days (72 hours).
Zollinger-Ellison-Syndrome and other pathological hyper secretory conditions: For the long-term management of Zollinger-Ellison-Syndrome and other pathological hyper secretory conditions patients should start their treatment with a daily dose of 80 mg PANTONIL. Thereafter, the dose can be titrated up or down as needed using measurements of gastric acid secretion to guide. With doses above 80 mg daily, the dose should be divided and given twice daily. A temporary increase of the dose above 160 mg pantoprazole is possible but should not be applied longer than required for adequate acid control.
In case a rapid acid control is required, a starting dose of 2 x 80 mg PANTONIL is sufficient to manage a decrease of acid output into the target range (<10 mEq/h) within one hour in the majority of patients.
Oral treatment should be started as soon as clinically confirmed.
Method of administration: PANTONIL is administered as i.v. injection.
A ready-to-use solution is prepared in 10 ml of sodium chloride 9 mg/ml (0.9%) solution for injection. The prepared solution may be administered directly or may be administered after mixing it with 100 ml sodium chloride 9 mg/ml (0.9%) solution for injection or glucose 55 mg/ml (5%) solution for injection.
The medicinal product should be administered intravenously over 2-15 minutes.
PANTONIL should not be mixed with other substances than the specified solvents.
After preparation the solution must be used within 12 hours.
Additional information on special populations: Patients with renal impairment: No dose adjustment is necessary in patients with impaired renal function.
Patients with hepatic impairment: A daily dose of 20 mg pantoprazole (half a vial of 40 mg pantoprazole) should not be exceeded in patients with severe liver impairment (see Precautions). Also liver enzymes should be monitored during PANTONIL treatment. Treatment with PANTONIL should be discontinued when liver enzymes are raised.
Paediatric population: The safety and efficacy of PANTONIL 40 mg lyophilized powder for solution for injection in children aged under 18 years have not been established. Therefore, Protium 40 mg powder for solution for injection PANTONIL is not recommended for use in patients below 18 years of age.
Elderly: No dose adjustment is necessary in elderly patients.
There are no known symptoms of overdose in man.
Systemic exposure with up to 240 mg administered intravenously over 2 minutes, were well tolerated.
As pantoprazole is extensively protein bound, it is not readily dialysable.
In the case of an overdose with clinical signs of intoxication, apart from symptomatic and supportive treatment, no specific therapeutic recommendations can be made.
PANTONIL, should not be used in patients with known Hypersensitivity to the active substance, substituted benzimidazoles, or to any of the excipients listed in Description.
Hepatic impairment: In patients with severe liver impairment, the liver enzymes should be monitored during therapy. In the case of a rise of the liver enzymes, the treatment should be discontinued (see Dosage & Administration).
Gastric malignancy: Symptomatic response to pantoprazole may mask the symptoms of gastric malignancy and may delay diagnosis. In the presence of any alarm symptom (e. g. significant unintentional weight loss, recurrent vomiting, dysphagia, haematemesis, anaemia or melaena) and when gastric ulcer is suspected or present, malignancy should be excluded.
Further investigation is to be considered if symptoms persist despite adequate treatment.
Co-administration with HIV protease inhibitors: Co-administration of pantoprazole is not recommended with HIV protease inhibitors for which absorption is dependent on acidic intragastric pH such as atazanavir, due to significant reduction in their bioavailability (see Interactions).
Bone fractures: Several published observational studies suggest that proton pump inhibitor (PPI) therapy may be associated with an increased risk of osteoporosis-related fractures of the hip, wrist, or spine. Patients receiving high doses defined as multiple daily doses and prolonged PPI therapy (one year or more) have an increased risk of fracture. Patients should receive the lowest dose and shortest duration of PPI therapy appropriate for the condition being treated.
Observational studies suggest that proton pump inhibitors may increase the overall risk of fracture by 10-40%. Some of this increase may be due to other risk factors. Patients at risk of osteoporosis should receive care according to current clinical guidelines and they should have an adequate intake of vitamin D and calcium.
Hypomagnesaemia: Symptomatic and asymptomatic hypomagnesaemia has been reported in patients treated with PPIs like pantoprazole for at least three months, and in most cases for a year. Serious manifestations of hypomagnesaemia such as fatigue, tetany, delirium, convulsions, dizziness and ventricular arrhythmia can occur but they may begin insidiously and be overlooked. In most affected patients, hypomagnesaemia improved after magnesium replacement and discontinuation of the PPI. For patients expected to be on prolonged treatment or who take PPIs with digoxin or medicinal products that may cause hypomagnesaemia (e.g. diuretics), health care professionals should consider measuring magnesium levels before starting PPI treatment and periodically during treatment.
Subacute cutaneous lupus erythematosus (SCLE): Proton pump inhibitors are associated with very infrequent cases of SCLE. If lesions occur, especially in sun-exposed areas of the skin, and if accompanied by arthralgia, the patient should seek medical help promptly and the health care professional should consider stopping Pantoprazole. SCLE after previous treatment with a proton pump inhibitor may increase the risk of SCLE with other proton pump inhibitors.
Interference with laboratory tests: Increased Chromogranin A (CgA) level interfere with investigations for neuroendocrine tumours are reported. To avoid this interference, PANTONIL treatment should be stopped for at least 5 days before CgA measurements (see Pharmacology: Pharmacodynamics under Actions). If CgA and gastrin levels have not returned to reference range after initial measurement, measurements should be repeated 14 days after cessation of proton pump inhibitor treatment.
Gastrointestinal infections caused by bacteria: Pantoprazole, like all proton pump inhibitors, can be expected to increase the number of bacteria normally found in the upper gastrointestinal tract. Treatment with PANTONIL may lead to a slightly increased risk of gastrointestinal infections caused by bacteria such as Salmonella and Campylobacter (see Pharmacology: Pharmacodynamics under Actions).
Long term treatment: In long-term treatment, especially when exceeding a treatment period of 1 year, patients should be kept under regular surveillance.
Sodium: This medicinal product contains less than 1 mmol sodium (23 mg) per vial, i.e. is essentially 'sodium-free'.
Additional information related with special populations: There is no study on special populations.
Effects on ability to drive and use machines: Pantoprazole has no or negligible influence on the ability to drive and use machines.
Adverse drug reactions, such as dizziness and visual disturbances may occur (see Adverse Reactions). If affected, patients should not drive or operate machines.
General advice: Pregnancy Category: B.
Women with childbearing potential/Contraception: Specific testing with an oral contraceptive containing levonorgestrel and ethinyl estradiol did not show any clinically significant interaction (see Interactions).
Pregnancy: Data from a limited number of pregnancy exposure cases (between 300-1000 pregnancy outcomes) do not indicate that pantoprazole has adverse effects (inducing malformations or having feto/neonatal toxicity) on pregnancy or on the health of the fetus/newborn child.
No important epidemiological data have been obtained. Animal studies have shown reproductive toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions). The potential risk for humans is unknown. Pantoprazole should not be used during pregnancy unless clearly necessary.
As a precautionary measure, it is preferable to avoid the use of PANTONIL during pregnancy.
Breast-feeding: Animal studies have shown excretion of pantoprazole in breast milk. There is insufficient information on the excretion of pantoprazole in human milk but excretion into human milk has been reported. A risk to the newborns/infants cannot be excluded. Therefore, a decision on whether to discontinue breast-feeding or to discontinue/abstain from PANTONIL therapy should take into account the benefit of breast-feeding for the child, and the benefit of PANTONIL therapy for the woman.
Fertility: There was no evidence of impaired fertility following the administration of pantoprazole in animal studies (see Pharmacology: Toxicology: Preclinical safety data under Actions).
In the reproductive studies in animals, mild levels of fetotoxicity were observed at doses above 5 mg/kg. There is no evidence of fertility loss or teratogenicity (see Pharmacology: Toxicology: Preclinical safety data under Actions).
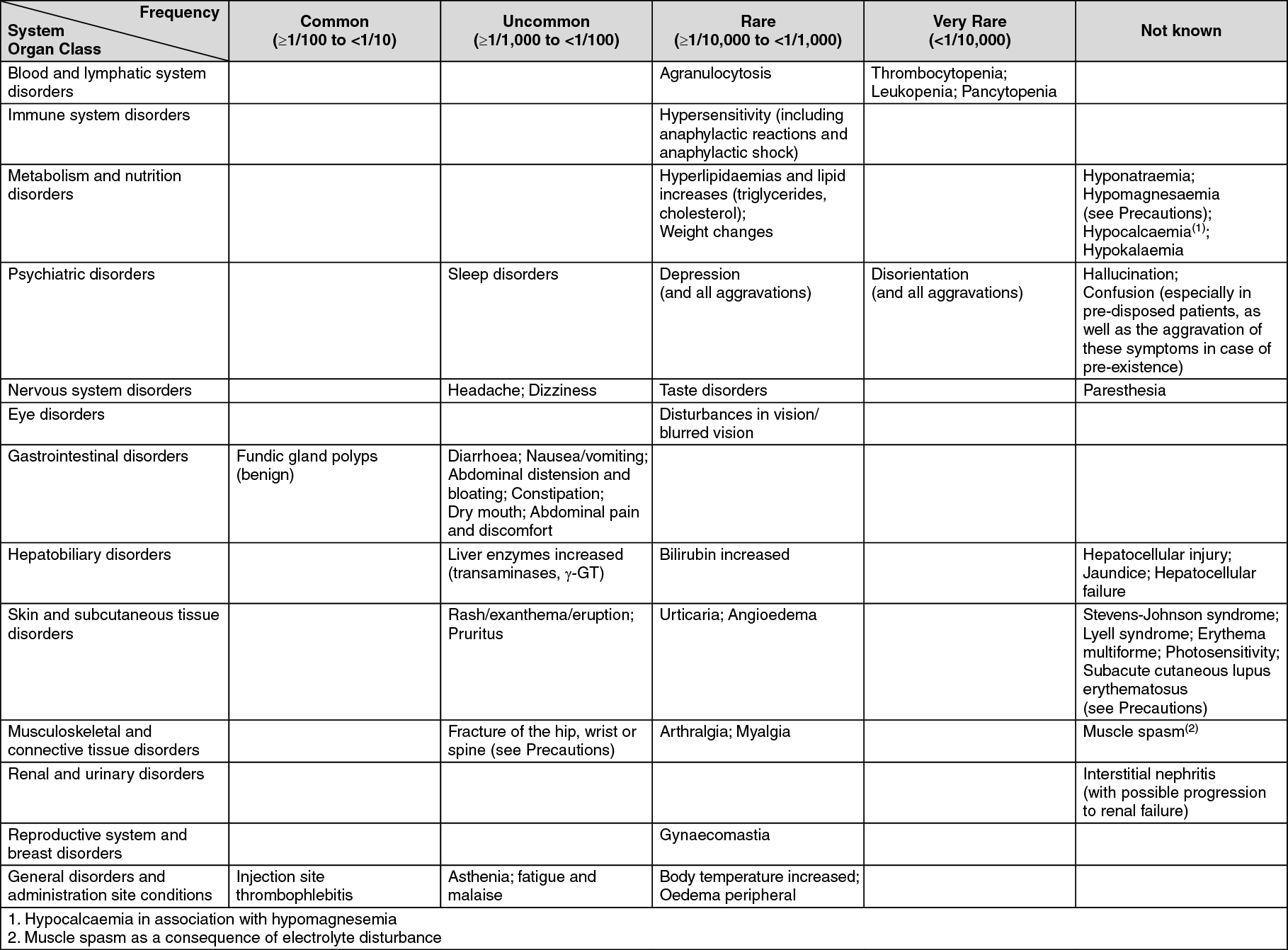
Approximately 5% of patients can be expected to experience adverse drug reactions (ADRs). The most commonly diarrhoea and headache occurred in approximately 1% of patients.
The table as follows lists adverse reactions reported with pantoprazole, ranked under the following frequency classification: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Medicinal products with pH dependent absorption pharmacokinetics: Because of profound and long-lasting inhibition of gastric acid secretion, pantoprazole may interfere with the absorption of other medicinal products where gastric pH is an important determinant of oral bioavailability, e.g. some azole antifungals such as ketoconazole, itraconazole, posaconazole and other medicine such as erlotinib.
HIV protease inhibitors: Co-administration of pantoprazole is not recommended with HIV protease inhibitors for which absorption is dependent on acidic intragastric pH such as atazanavir due to significant reduction in their bioavailability (see Precautions).
If the combination of HIV protease inhibitors with a proton pump inhibitor is judged unavoidable, close clinical monitoring (e.g. virus load) is recommended. A pantoprazole dose of 20 mg per day should not be exceeded. Dosage of the HIV protease inhibitor may need to be adjusted.
Coumarin anticoagulants (phenprocoumon or warfarin): Co-administration of pantoprazole with warfarin or phenprocoumon did not affect the pharmacokinetics of warfarin, phenoprocoumon or INR. However, there have been post-marketing reports of increased INR and prothrombin time in patients receiving PPIs and warfarin or phenoprocoumon concomitantly. Increases in INR and prothrombin time may lead to abnormal bleeding, and even death. Patients treated with pantoprazole and warfarin or phenprocoumon may need to be monitored for increase in INR and prothrombin time.
Methotrexate: Concomitant use of high dose methotrexate (e.g. 300 mg) and proton-pump inhibitors has been reported to increase methotrexate levels in some patients. Therefore, in settings where high-dose methotrexate is used, for example cancer and psoriasis, a temporary withdrawal of pantoprazole may need to be considered.
Other interactions studies: Pantoprazole is extensively metabolized in the liver via the cytochrome P450 enzyme system. The main metabolic pathway is demethylation by CYP2C19 and other metabolic pathways include oxidation by CYP3A4.
Interaction studies with medicinal products also metabolized with these pathways, like carbamazepine, diazepam, glibenclamide, nifedipine, and an oral contraceptive containing levonorgestrel and ethinyl oestradiol, did not reveal clinically significant interactions.
An interaction of pantoprazole with other medicinal products or compounds, which are metabolized using the same enzyme system, cannot be excluded.
Results from a range of interaction studies demonstrate that pantoprazole does not affect the metabolism of active substances metabolised by CYP1A2 (such as caffeine, theophylline), CYP2C9 (such as piroxicam, diclofenac, naproxen), CYP2D6 (such as metoprolol), CYP2E1 (such as ethanol), or does not interfere with p-glycoprotein related absorption of digoxin.
There were no interactions with concomitantly administered antacids.
Interaction studies have also been performed by concomitantly administering pantoprazole with the respective antibiotics (clarithromycin, metronidazole, amoxicillin). No clinically relevant interactions were found.
Medicinal products that inhibit or induce CYP2C19: Inhibitors of CYP2C19 such as fluvoxamine could increase the systemic exposure of pantoprazole. A dose reduction may be considered for patients treated long-term with high doses of pantoprazole, or those with hepatic impairment.
Enzyme inducers affecting CYP2C19 and CYP3A4 such as rifampicin and St John's wort (Hypericum perforatum) may reduce the plasma concentrations of PPIs that are metabolized through these enzyme systems.
Incompatibilities: This medicinal product must not be mixed with other medicinal products except those mentioned in Special precautions for disposal and other handling previously.
Special precautions for disposal and other handling: A ready-to-use solution is prepared by injecting 10 ml of sodium chloride 9 mg/ml (0.9%) solution for injection into the vial containing the powder. The appearance of the product after reconstitution is a colorless or pale yellowish solution. This solution may be administered directly or may be administered after mixing it with 100 ml sodium chloride 9 mg/ml (0.9%) solution for injection or glucose 55 mg/ml (5%) solution for injection. Glass or plastic containers should be used for dilution.
After reconstitution, or reconstitution and dilution, chemical and physical in use stability has been demonstrated for 12 hours at 25°C.
From a microbiological point of view, the product should be used immediately.
PANTONIL should not be prepared or mixed with solvents other than those stated.
The medicine should be administered intravenously over 2-15 minutes.
The contents of the vial are for single use only. Any product that has remained in the container or the visual appearance of which has changed (e.g. if cloudiness or precipitation is observed) should be disposed of in accordance with local requirements.
Store below 25°C at room temperature.
Keep the vial in the outer carton in order to protect from light.
For storage conditions of the reconstituted and diluted medicinal product see Shelf-life as follows.
Shelf life: Unopened vial: 2 years.
After reconstitution, or reconstitution and dilution, chemical and physical in use stability has been demonstrated for 12 hours at 25°C.
From a microbiological point of view, the product should be used immediately.
If not used immediately, in-use storage times and conditions are the responsibility of the user.
Pantonil lyo powd for inj 40 mg
1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out