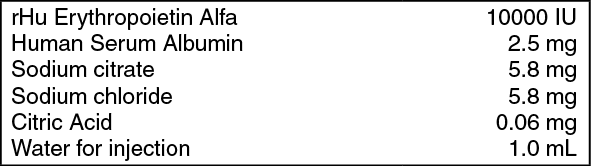
Each prefilled syringe of 1.0 mL contains: Recombinant Human Erythropoietin Alfa 10000 IU.
Erythropoietin is a glycoprotein, which stimulates red blood cell production. It is produced in the kidney and stimulates the division and differentiation of committed erythroid progenitors in the bone marrow. Recombinant human erythropoietin (Epoetin alfa), a 165 amino acid glycoprotein manufactured by recombinant DNA technology, has the same biological effects as endogenous erythropoietin. It has a molecular weight of 30,400 daltons and is produced by mammalian cells into which the human erythropoietin gene has been introduced. The product contains the identical amino acid sequence of isolated natural erythropoietin.
Recombinant Human Erythropoietin Alfa (Renogen) is a clear, colorless, preservative free liquid containing active ingredient erythropoietin alfa. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacology: Chronic Renal Failure Patients: Endogenous production of erythropoietin is normally regulated by the level of tissue oxygenation. Hypoxia and anemia generally increase the production of erythropoietin which in turn stimulates erythropoiesis. In normal subjects, plasma erythropoietin levels range from 0.01 to 0.03 Units/mL and increase up to 100- to 1000-fold during hypoxia or anemia. In contrast, in patients with chronic renal failure (CRF), production of erythropoietin is impaired, and this erythropoietin deficiency is the primary cause of their anemia.
Erythropoietin has been shown to stimulate erythropoiesis in anemic patients with CRF, including both patients on dialysis and those who do not require regular dialysis. The first evidence of a response to the three times weekly (TIW) administration of erythropoietin is an increase in the reticulocyte count within 10 days, followed by increases in the red cell count, hemoglobin, and hematocrit, usually within 2 to 6 weeks. Once the hematocrit reaches the suggested target range (30% to 36%), that level can be sustained by erythropoietin therapy in the absence of iron deficiency and concurrent illnesses.
The rate of hematocrit increase varies between patients and is dependent upon the dose of erythropoietin, within a therapeutic range of approximately 50 to 300 Units/kg. The factors affecting the rate and extent of response include availability of iron stores, the baseline hematocrit, and the presence of concurrent medical problems.
Cancer Patients on Chemotherapy: Anemia in cancer patients may be related to the disease itself or the effect of concomitantly administered chemotherapeutic agents. Erythropoietin has been shown to increase hematocrit and decrease transfusion requirements after the first month of therapy (months 2 and 3), in anemic cancer patients undergoing chemotherapy.
Zidovudine-treated HIV-infected Patients: Responsiveness to erythropoietin in HIV-infected patients is dependent upon the endogenous serum erythropoietin level prior to treatment. Patients with endogenous serum erythropoietin levels ≤500 mUnits/mL, and who are receiving a dose of zidovudine ≤4200 mg/week, may respond to erythropoietin therapy. Patients with endogenous serum erythropoietin levels >500 mUnits/mL do not appear to respond to erythropoietin therapy. Response to erythropoietin in zidovudine-treated HIV-infected patients is manifested by reduced transfusion requirements and increased hematocrit.
Pharmacodynamics: Clinical Effects: Chronic Renal Failure Patients: Response to erythropoietin was consistent across all studies. In the presence of adequate iron stores (see Iron Evaluation), the time to reach the target hematocrit is a function of the baseline hematocrit and the rate of hematocrit rise.
The rate of increase in hematocrit is dependent upon the dose of erythropoietin administered and individual patient variation.
Once the target hematocrit (32% to 38%) was achieved, statistically significant improvements were demonstrated for most quality of life parameters measured, including energy and activity level, functional ability, sleep and eating behavior, health status, satisfaction with health, sex life, well-being, psychological effect, life satisfaction, and happiness.
Adult Patients on Dialysis: The clinical studies were conducted, involving IV administration to anemic patients of erythropoietin therapy. In the three largest of these clinical trials, the median maintenance dose necessary to maintain the hematocrit to 30% to 36% was approximately 75 Units/kg TIW.
Patients with CRF Not Requiring Dialysis: The clinical trials with erythropoietin were conducted in patients with CRF not on dialysis. These patients responded to erythropoietin therapy in a manner similar to that observed in patients on dialysis. Patients with CRF not on dialysis demonstrated a dose-dependent and sustained increase in hematocrit when erythropoietin was administered by either an IV or SC route, with similar rates of rise of hematocrit when erythropoietin was administered by either route.
Zidovudine-treated HIV-infected Patients: Erythropoietin has been studied in clinical trials enrolling anemic (hematocrit <30%), HIV-infected (AIDS) patients receiving concomitant therapy with zidovudine. Erythropoietin reduced the mean cumulative number of units of blood transfused per patient by approximately 40% as compared to the placebo group.
In a 6 month open-label erythropoietin study, patients responded with decreased transfusion requirements and sustained increases in hematocrit and hemoglobin with doses of erythropoietin up to 300 Units/kg TIW.
Cancer Patients on Chemotherapy: Erythropoietin has been studied in a series of placebo-controlled, double blind trials in anemic cancer patients. Within this group, patients were treated with concomitant non cisplatin-containing chemotherapy regimens and cisplatin-containing chemotherapy regimens. Patients were randomized to erythropoietin 150 Units/kg or placebo subcutaneously TIW for 12 weeks.
Erythropoietin therapy was associated with a significantly (p <0.008) greater hematocrit response than in the corresponding placebo-treated patients.
Surgery Patients: Erythropoietin has been studied in a placebo-controlled, double-blind trial enrolling patients scheduled for major, elective orthopedic hip or knee surgery who were expected to require ≥2 units of blood and who were not able or willing to participate in an autologous blood donation program. All patients received oral iron and a low-dose post-operative warfarin regimen.
Treatment with erythropoietin 300 Units/kg significantly (p = 0.024) reduced the risk of allogeneic transfusion in patients with a pretreatment hemoglobin of >10 to ≤13 g/dL.
Efficacy of recombinant human erythropoietin alfa (Renogen) in Indian Patients: The efficacy and safety of erythropoietin was evaluated in open label, 12 weeks, phase III confirmatory trial conducted in Indian patients for the treatments of anemia due to chronic kidney disease. This multicenter study enrolled patients both on dialysis and those not on dialysis with a hematocrit of 24%. Patients were evaluated for rise in hematocrit and reticulocyte count after erythropoietin administration at the baseline and 2-weeks. The patients were also evaluated for achieving the target hematocrit >33% at 12 weeks of drug administration in a dose of 50-150 IU/kg three times in a week. The safety of Erythropoietin was assessed by reporting spontaneous and serious adverse events and laboratory investigations for liver and kidney functions.
There was significant mean increase in hematocrit of 2.63% and reticulocyte of 1.07% (corrected for hematocrit) after 2 weeks of drug administration. 63.2% of patients achieved the target hematocrit of 33% or more at 12 weeks of erythropoietin administration. The remaining 36.8% patients showed an increase in hematocrit till the end of study. No patients required blood transfusion during the treatment with Recombinant Human Erythropoietin Alfa (Renogen).
There was no alteration in liver and kidney functions after erythropoietin administration as assessed by laboratory investigations. The drug was well tolerated in all the patients and no significant adverse effects reported with erythropoietin in this study.
Pharmacokinetics: Intravenously administered erythropoietin is eliminated at a rate consistent with first order kinetics with a circulating half-life ranging from approximately 4 to 13 hours in adult patients with CRF. Within the therapeutic dose range, detectable levels of plasma erythropoietin are maintained for at least 24 hours. After SC administration of erythropoietin to patients with CRF, peak serum levels are achieved within 5 to 24 hours after administration and decline slowly thereafter.
The pharmacokinetic profile of erythropoietin in children and adolescents appears to be similar to that of adults. Limited data are available in neonates.
Toxicology: Preclinical Pharmacology: In-vivo bioassay was performed to assess the potency of recombinant human erythropoietin alfa (Renogen) in swiss albino mice based on European Pharmacopoeia requirements. Reticulocyte count was analyzed using parallel line assay. The analysis revealed that the Intas recombinant human erythropoietin alfa (Renogen) and the standard erythropoietin are comparable in specific biological activities.
Toxicity Studies: Acute toxicity studies were conducted in rats and mice by administering I.V. and S.C. single dose of erythropoietin. There was no death or any adverse effect in the animals at all dose levels. In repeat dose subacute toxicity studies in rats and mice a dose of 30, 300, 3000 IU/kg was administered for a period of 28 days by SC and IV routes. The animals were examined for body weight changes, food consumption, hematology, blood chemistry and histopathological examination of body organs. There was no abnormality detected in any of the parameters in both the species. Erythropoietin was well tolerated in low, medium and high dose levels in these studies.
rHu EPO was also evaluated for local irritation and allergenecity by conducting primary irritation test in rabbits and allergic contact sensitization in guinea pigs. The test drug was well tolerated and there was no evidence of any irritation in animals.
Treatment of Anemia in Cancer Patients on Chemotherapy: Erythropoietin is indicated for the treatment of anemia in patients with non-myeloid malignancies where anemia is due to the effect of concomitantly administered chemotherapy. Erythropoietin is indicated to decrease the need for transfusions in patients who will be receiving concomitant chemotherapy for a minimum of 2 months.
Treatment of Anemia in Zidovudine-treated HIV-infected Patients: Erythropoietin is indicated for the treatment of anemia related to therapy with zidovudine in HIV-infected patients. Erythropoietin is indicated to elevate or maintain the red blood cell level (as manifested by the hematocrit or hemoglobin determinations) and to decrease the need for transfusion in these patients.
Reduction of Allogeneic Blood Transfusions in Surgery Patients: Erythropoietin is indicated for the treatment of anemic patients (hemoglobin >10 to ≤13 g/dL) scheduled to undergo elective, noncardiac, nonvascular surgery to reduce the need for allogeneic blood transfusions. Erythropoietin is indicated for patients at high risk of perioperative transfusions with significant, anticipated blood loss. Erythropoietin is not indicated for anemic patients who are willing to donate autologous blood. The safety of the perioperative use of erythropoietin has been studied only in patients who are receiving anticoagulant prophylaxis.
Cancer Patients on Chemotherapy: The recommended dose of erythropoietin for adults is 150-300 Units/kg SC TIW or 40,000 Units SC once in a week. Baseline endogenous serum erythropoietin levels varied among patients with cancer related anemia. Treatment of patients with grossly elevated serum erythropoietin levels (eg. >200 mUnits/mL) is not recommended. The hematocrit should be monitored on a weekly basis in patients receiving erythropoietin therapy until hematocrit becomes stable.
Zidovudine-treated HIV-Infected Patients: Starting Dose: For adult patients with serum erythropoietin that the endogenous serum erythropoietin level be determined (prior to transfusion). Available evidence suggests that patients receiving zidovudine with endogenous serum erythropoietin levels >500 mUnits/mL are unlikely to respond to therapy with erythropoietin.
Surgery Patients: The recommended dose of erythropoietin is 300 Units/kg/day subcutaneously for 10 days before surgery, on the day of surgery and for 4 days after surgery. Prior to initiating treatment with erythropoietin, a hemoglobin should be obtained to establish that it is >10 to ≤13 g/dL. An alternate dose schedule is 600 Units/kg erythropoietin subcutaneously in once weekly doses (21, 14, and 7 days before surgery) plus a fourth dose on the day of surgery.
All patients should receive adequate iron supplementation. Iron supplementation should be initiated no later than the beginning of treatment with erythropoietin and should continue throughout the course of therapy.
Preparation and Administration of Erythropoietin: Do not shake as vigorous shaking may denature any glycoprotein, rendering it biologically inactive. Use aseptic techniques in drug administration. Use one dose pre-filled syringe. Discard unused portion, do not dilute or administer in conjunction with other solutions.
The maximum amount of erythropoietin that can be safely administered in single or multiple doses has not been determined. Doses of up to 1500 Units/kg for 3 to 4 weeks have been administered to adults without any direct toxic effects of erythropoietin.
Erythropoietin is contraindicated in patients with: Uncontrolled hypertension; known hypersensitivity to mammalian cell-derived products; known hypersensitivity to Albumin (Human).
Thrombotic Events and Increased Mortality: Increased mortality was observed in patients randomized to a target hematocrit of 42% [(35% mortality)] compared to patients targeted to remain at a hematocrit of 30% [(29% mortality)].
Chronic Renal Failure Patients: Hypertension: Patients with uncontrolled hypertension should not be treated with erythropoietin; blood pressure should be controlled adequately before initiation of therapy. During the early phase of treatment when the hematocrit is increasing, approximately 25% of patients on dialysis may require initiation of, or increases in, antihypertensive therapy. Hypertensive encephalopathy and seizures have been observed in patients with CRF treated with erythropoietin.
Seizures: Seizures have occurred in patients with CRF participating in erythropoietin clinical trials. It is recommended that the dose of erythropoietin be decreased if the hematocrit increase exceeds 4 points in any 2-week period.
Thrombotic Events: During hemodialysis, patients treated with erythropoietin may require increased anticoagulation with heparin to prevent clotting of the artificial kidney.
The parenteral administration of any biologic product should be attended by appropriate precautions in case allergic or other untoward reactions occur. In clinical trials, while transient rashes were occasionally observed concurrently with erythropoietin therapy; no serious allergic or anaphylactic reactions were reported.
The safety and efficacy of erythropoietin therapy have not been established in patients with a known history of a seizure disorder or underlying hematologic disease (e.g., sickle cell anemia, myelodysplastic syndromes, or hypercoagulable disorders).
Hematology: Exacerbation of porphyria has been observed rarely in patients with CRF treated with erythropoietin. Erythropoietin should be used with caution in patients with known porphyria.
Delayed or Diminished Response: If the patient fails to respond or to maintain a response to doses within the recommended dosing range, the following etiologies should be considered and evaluated: Iron deficiency: Virtually all patients will eventually require supplemental iron therapy; Underlying infectious, inflammatory, or malignant processes; Occult blood loss; Underlying hematologic diseases (i.e., thalassemia, refractory anemia, or other myelodysplastic disorders); Vitamin deficiencies: Folic acid or vitamin B12; Hemolysis; Aluminum intoxication; Osteitis fibrosa cystica.
Iron Evaluation: Transferrin saturation should be at least 20% and ferritin should be at least 100 ng/mL. Prior to and during erythropoietin therapy, the patient's iron status, including transferrin saturation (serum iron divided by iron binding capacity) and serum ferritin, should be evaluated. Virtually all patients will eventually require supplemental iron to increase or maintain transferrin saturation to levels, which will adequately support erythropoiesis stimulated by erythropoietin.
Carcinogenesis, Mutagenesis, And Impairment Of Fertility: Carcinogenic potential of erythropoietin has not been evaluated. Erythropoietin does not induce bacterial gene mutation (Ames Test), chromosomal aberrations in mammalian cells, micronuclei in mice, or gene mutation at the HGPRT locus. In female rats treated IV with erythropoietin, there was a trend for slightly increased fetal wastage at doses of 100 and 500 Units/kg.
Pregnancy: Pregnancy Category C: There are no adequate and well-controlled studies in pregnant women. Erythropoietin should be used during pregnancy only if potential benefit justifies the potential risk to the fetus.
Nursing Mothers: It is not known whether erythropoietin is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when erythropoietin is administered to a nursing woman.
Erythropoietin is generally well tolerated. The adverse events reported are frequent sequelae of disease and are not necessarily attributable to erythropoietin therapy. The events reported in greater than 5% of patients treated with erythropoietin during the blinded phase were: hypertension, headache, arthralgia, nausea, edema, fatigue, diarrhea, vomiting, chest pain, skin reaction (administration site), asthenia, dizziness, clotted access, pyrexia, constipation, deep vein thrombosis.
Events reported to have occurred within several hours of administration of erythropoietin were rare, mild, and transient, and included injection site stinging in dialysis patients and flu-like symptoms such as arthralgias and myalgias.
No evidence of interaction of erythropoietin with other drugs was observed in the course of clinical trials.
Store at 2 to 8°C (36 to 46°F). Do not freeze or shake. Protect from light.
Shelf-life: 24 months.
B03XA01 - erythropoietin ; Belongs to the class of other antianemic preparations. Used in the treatment of anemia.
Renogen soln for inj 10,000 IU/mL
1's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out